Chapter 28
ENDOPHTHALMITIS

Endophthalmitis is an uncommon but devastating consequence of open globe injury.1 The relatively poor visual prognosis of traumatic endophtalmitis is due to:
• the higher frequency of organisms that are more virulent than those in postoperative cases;
• the associated trauma;
• the frequent delay in diagnosis; and
• the frequent delay in the initiation of treatment.2–13
Traumatic endophthalmitis therefore presents difficult diagnostic and management issues distinct from endophthalmitis occurring in other settings.
EPIDEMIOLOGY
The incidence of endophthalmitis after open globe injury is 5 to 14%;1,9,12,13 In the USEIR, the incidence is 2.6%.
Traumatic endophthalmitis constitutes approximately 10 to 30% of all infectious endophthalmitisa,4–8,12 cases. It is more common in males (85%).10 In the USEIR, the rate is 2.8% among males and 1.4% among females.
Riskfactors for the development of traumatic endophthalmitis include:
• >24 hours of delay in primary wound closure;
• presence of an IOFB (6.9–13%, independent of IOFB type)14 ;
• rural setting:
 soil contamination is believed to result in a higher rate of endophthalmitis (30%) for open globe injuries occurring in a rural versus a nonrural setting11; and
soil contamination is believed to result in a higher rate of endophthalmitis (30%) for open globe injuries occurring in a rural versus a nonrural setting11; and
• rupture of the lens capsule.13
CLINICAL DIAGNOSIS
The symptoms and signs are similar to those in other categories of endophthalmitis, but the diagnosis is often delayed due to masquerading signs that usually accompany severe ocular trauma. Early symptoms may include:
• photophobia;
• pain out of proportion to the clinical findings;
• visual loss worse than media opacities might suggest;
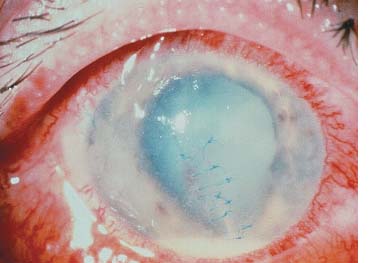
• hypopyon (Fig. 28–1);
• vitritis; and
• retinal periphlebitis.15
Other, less specific signs include:
• lid edema;
• conjunctival erythema and edema;
• corneal edema;
• fibrinous membrane formation on the iris, lens, or the IOL; and
• loss of the red reflex or progressively worsening view of the posterior pole.
Fungal infection is more common in the following injuries:
• IOFB, especially if it is vegetable matter (e.g., thorn, wood); or
• soil contamination.
Characteristic signs of intraocular fungal infection include:
• slowly progressive inflammation after initial trauma repair;
• white “snowball-like” opacities or “string-of-pearls” configuration in the vitreous;
• chronic vitritis; and
• persistent white infiltrates around the primary wound side.16
PEARL… Retinal periphlebitis is an early sign of endophthalmitis. However, it is often not recognized because of the common presence of media opacities.
MICROBIOLOGY
The microbiology of traumatic endophthalmitis is significantly different from that in other categories. Infections with more than one organism are common (up to 48%).10,14 The organism is often virulent.
Gram-positive bacteria (usually cocci such as Streptococcus and Staphylococcus species) are the predominant isolates in both the adult and pediatric age groups.8,10–12 There is a high incidence of Bacillusspecies. These infections are notable for their:
• rapid (<24 hours) onset;
• high risk of progression to panophthalmitis; and
• rate of poor visual outcome.
Endophthalmitis caused by Bacillus species is characterized by:
• severe pain;
• hypopyon;
• chemosis; and
• rapidly progressive proptosis and lid edema.
Additional information regarding Bacillus endophthalmitis includes the following.
• The characteristic ring-shaped corneal infiltrate is a late sign.
• Although rare in postoperative cases, it is rather common (up to 46% after open globe trauma) in the United States,11 representing the second most common group after Staphylococcus species in IOFB injuries.14
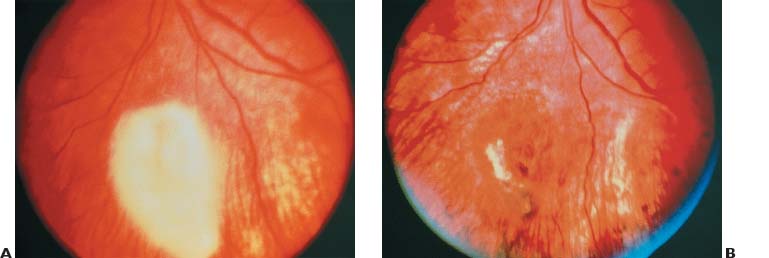
• Although it was previously considered to have a uniformly poor visual prognosis, early recognition and prompt treatment of infection caused by Bacillus species (Fig. 28–2) may occasionally result in good visual outcome.17,18
Culturing for Microbiologic Analysis
The first question is: in which cases should a sample be taken?
PEARL… When traumatic endophthalmitis is suspected, one should attempt to culture intraocular contents in all cases.
CONTROVERSY
Following an open globe injury, the ophthalmologist may consider routinely culturing all cases, but such an approach will yield a fair number of false-positive results and probably adds little to the clinical care of the patient (see Chapter 24).
The second question is: where should the sample be taken from?
• We do not routinely culture the wound or conjunctiva: the high risk of contamination makes a positive culture difficult to interpret.
• We do culture the wound if there is a specific indication of infection present.
In reported series of traumatic endophthalmitis, vitreous specimens have a higher rate of positive culture than aqueous samples.19,20 The extent of vitrectomy performed to obtain samples depends on the visibility of the posterior segment and the surgeon’s experience (see the Appendix for more details).
The third question is: which culture media should be used? Commonly used plates for bacterial and fungal cultures are:
• blood agar; and
• chocolate agar.
With a larger intraocular specimen, smears can be sent for:
• Gram, Giemsa, and fungal stains;
• sabouraud’s media (fungi);
• thioglycollate broth (all-purpose holding media); and
• anaerobic blood culture bottle.
Because the initial surgery is often performed in “off-hours,” the standard culture media may not be immediately available (see also the Appendix).
PEARL… After hours or on the weekends, when the microbiology personnel may not be available to process the vitreous specimen, the vitreous aspirate can be directly injected into blood culture bottles. The culture yield of this technique appears to be comparable to that of conventional methods21,22 (see also the Appendix).
Fungal cultures are indicated in cases in which initial bacterial cultures were negative or when fungal infection is strongly suspected.
PREVENTION:
PROPHYLACTIC ANTIBIOTICS
Systemic antibiotics, although not confirmed in a randomized prospective study, may reduce the incidence of endophthalmitis in eyes with open globe injury. The selected antibiotic should:
• provide coverage against the most common pathogens known to cause traumatic endophthalmitis (i.e., Bacillus species and gram-positive organisms); and
• have adequate intraocular penetration after systemic administration.
The ideal antibiotic regimen remains controversial; Table 28–1 shows one protocol for prophylaxis of traumatic endophthalmitis.
| Systemic antibiotic therapy* | Vancomycin hydrochloride, 1 g iv every 12 h |
| Ceftazidime, 1 g iv every 12 h | |
| Subconjunctival antibiotic and corticosteroid therapy | Vancomycin hydrochloride, 25 mg |
| Ceftazidime, 100 mg | |
| Dexamethasone, 12 mg | |
| Topical therapy (started on the first postoperative day) | Antibiotic (physician’s choice, commercially available antibiotic in nonfortified concentration) |
| Topical cycloplegics and corticosteroids | |
| Optional: fortified antibiotic drops may be substituted in high-risk injuries with suspicion of infection |
* Intravitreal antibiotic and corticosteroid therapy generally reserved for selected injuries with high risk of infection or when considering outpatient management of open globe injury.
• Although a first-generation cephalosporin may provide coverage for gram-positive organisms,23 intravenous vancomycin is an excellent choice because it:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


