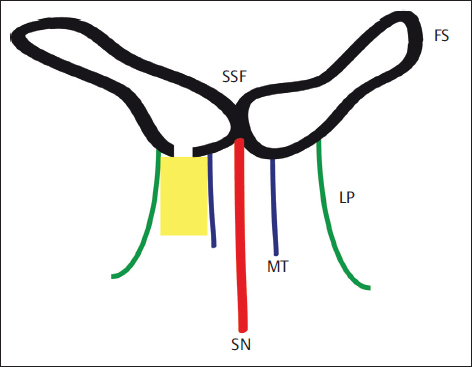
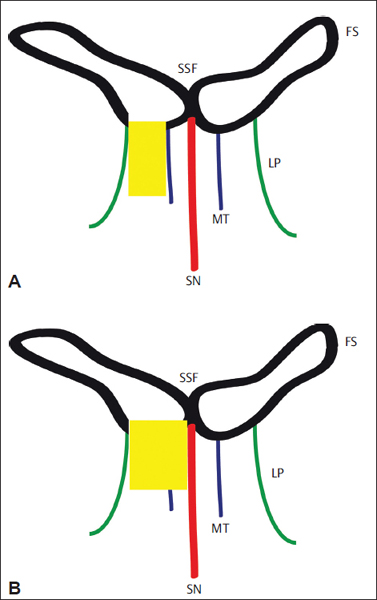
16 Endonasal Endoscopic Frontal Sinus Surgery Modern endonasal sinus surgery started roughly around the beginning of the 20th century.1,2 The endonasal approach to the ethmoid cells was first described by Riberi in 1838, who then reported a case involving the management of the frontal sinus by resection of the lamina papyracea using a chisel.3 Halle, in 1906, reported on successful endonasal drainage of the frontal sinus using just headlight and the naked eye.2 However, in the English-speaking literature, Mosher is regarded as the founder of endonasal ethmoid sinus surgery describing a more detailed and structured surgical technique. In 1912, Mosher indicated that the natural ostium of the frontal sinus could be reached more easily through an endonasal approach.3 At the establishment of this new period in rhinology, only a few surgeons were able to achieve a successful ethmoidectomy and simple drainage of the frontal sinus. In this preantibiotic and pre-endoscopic time, endonasal surgery of the paranasal sinuses performed by less-gifted surgeons was a life-threatening treatment with a high incidence of catastrophic complications including brain abscess, meningitis, and encephalitis. Consequently, despite the early successes of endonasal surgery, Mosher stated that the intranasal ethmoidectomy had “proven to be one of the easiest ways to kill a patient.” Lothrop in 1914 described opening of both frontal sinuses using a unilateral external approach for uniting both frontal sinus infundibula and resecting the adjacent upper nasal septum but seriously warning to try this via an endonasal approach.4 Further-more, anesthesia techniques were insufficient to provide a satisfactory, bloodless operative field. It was for this reason, that for many decades, most paranasal sinus surgeries were dominated by external approaches.5 Therefore, between 1920 and almost 1980, endonasal surgery was generally neglected worldwide and practiced in only a few centers. The new era of endonasal sinus surgery was revolutionized by the introduction of operating microscope(s) and endoscopes in sinus surgery. In the middle of the century, Heermann (1958) introduced the microscope in endonasal sinus surgery.6 However, it was the advent of endoscopes, mainly associated with the British physicist Harold Hopkins,7,8 that promoted a renewed interest in endonasal endoscopy as a diagnostic and therapeutic technique.9,10 Major steps within rhinology such as the introduction of endoscopic and microscopic visualization techniques and developments in radiology including computer-assisted tomography, magnetic resonance imaging, and interventional radiology facilitated the benefits of endonasal endoscopic frontal sinus surgery (EEFSS).11,12 These developments have been recently complemented through the use of intraoperative navigation systems and powered instrumentation that have helped to optimize the results.13 Between 1980 and 1984, the Fulda school developed a system of endonasal drainage procedures directed to the frontal sinuses.14 This rebirth of endonasal frontal sinus surgery was also a contribution of general anesthesia, which was, unlike other centers, routinely applied in the Fulda school. The Fulda concept of frontal sinus surgery started as a microendoscopic technique, which developed within the next three decades to an almost exclusively endoscopic approach. For EEFSS, general anesthesia, if necessary, with controlled hypotension is required. In addition, we recommend using a local decongestant and epinephrine to achieve a maximal bloodless operative field. The most important instruments are 0- and 45-degree endoscopes and a pair of straight/curved through-cutting forceps. In experienced hands the shaver allows gentle removal of polyps. In combination with curved diamond and cutting drills, further areas of the frontal sinus can be accessed. Especially in revision surgery of the frontal sinus and in tumor surgery, navigation systems nowadays have gained major importance.15 EEFSS is performed with the patient under combined local and general anesthesia.14,15 To reach a bloodless field, a topical decongestant is applied by packing the inferior and middle portions of the nasal meatus with gauze strips soaked in naphazoline hydrochloride and 2 mL of cocaine 10% solution. Xylocaine 1% with 1:120,000 units of epinephrine is injected in the region of uncinate process and agger nasi. Wait for at least 10 minutes to take the effect of local anesthesia and vasoconstriction. Bleeding is a major problem during endoscopic frontal sinus surgery. In many cases, bleeding can be reduced with the help of anesthetic techniques. The anesthesiologist should be informed constantly about the actual bleeding situation and should follow surgery on a monitor. Intraoperative interaction between the surgeon and the anesthesiologist is mandatory. If the comorbidities of the patient provide no contraindication, controlled hypotension at a mean arterial pressure of 60 mm Hg and a heart rate of 50 to 60 bpm is recommended. Arterial hypotension will minimize hemodynamic causes for bleeding. The influence of various anesthetics on bleeding is continuously under discussion. A total intravenous technique may have advantages with regard to bleeding on the microcirculatory level. In case of diffuse bleeding, adrenaline-soaked pledgets (adrenaline 1:1000) may be applied intraoperatively.16 We recommend starting the surgery on the right side with the surgeon standing on the same side. The surgical approach is more difficult on the right side than the left, because of the positioning of the surgeon. The EEFSS is performed by using a 45-degree rigid telescope with a suction/irrigation handle. The shaver is very helpful for gentle tissue removal and also for drilling in the frontal sinus. Surgery on the frontal recess is usually preceded at least by an anterior, more often than not by a complete ethmoidectomy. Exceptions are the cases where a complete ethmoidectomy has already been performed. It is important to remove agger nasi cells and to identify the lamina papyracea laterally, the attachment of the middle turbinate medially, and the anterior skull base with the anterior ethmoidal artery superiorly. Type I drainage is established by ethmoidectomy including the cell septa in the region of the frontal recess (Fig. 16.1).17 The inferior part of Killian infundibulum and its mucosa are not touched. Type I drainage is indicated if there is a minor pathology in the frontal sinus and the patient does not suffer from “prognostic risk factors” such as asthma and aspirin hypersensitivity, which are associated with reduced quality of mucosa and possible problems in outcome. In the majority of cases, the frontal sinus heals because of the improved drainage via the ethmoid cavity. Figure 16.1 Schematic view of frontal sinus drainage type I after complete ethmoidectomy and removal of cell septa in the frontal recess. FS, frontal sinus; LP, lamina papyracea; MT, middle turbinate; SSF, interfrontal sinus septum; SN, septum nasi. Extended drainage is achieved after ethmoidectomy by removing the floor of the frontal sinus between the lamina papyracea and the middle turbinate (type IIa) or the nasal septum (type IIb) anterior to the ventral margin of the olfactory fossa (Figs. 16.2 and 16.3). Hosemann et al18,19 showed in a detailed anatomical study that the maximum diameter of a neo-ostium of the frontal sinus (type IIa), which could be gained using a curette or a spoon, was 11 mm with an average of 5.6 mm. Figure 16.2 Schematic view of frontal sinus drainage type IIa with removal of frontal sinus floor from the lamina papyracea to the middle turbinate (A) or to the nasal septum, which results in type IIb drainage (B). FS, frontal sinus; LP, lamina papyracea; MT, middle turbinate; SSF, interfrontal sinus septum; SN, septum nasi.
History of Endonasal Frontal Sinus Surgery
Necessary Technology
Technical Details of Surgery
Type I: Simple Drainage
Type IIa/b: Extended Drainage
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


