Medical treatment for Meniere’s disease is effective in controlling vertigo for approximately 85% of patients. However, when disabling vertigo continues, surgical therapy is indicated. Several surgical approaches are performed to control the symptoms of peripheral vestibular disorders refractory to medical measures, each procedure having many technical variations. Surgery is usually reserved for patients with disabling vertigo. Here, the authors discuss surgical options for vertigo control in Meniere’s disease and review the literature on outcomes of these management options. The authors discuss endolymphatic sac shunt (ie, endolymphatic mastoid shunt), vestibular nerve section, cochleosacculotomy, and labyrinthectomy. When looking at data based on patient ratings, the authors find that surgery improves vertigo in endolymphatic sac shunt, vestibular nerve section, and labyrinthectomy groups and improves imbalance for the endolymphatic sac shunt and vestibular nerve section groups. Labyrinthectomy and translabyrinthine vestibular nerve section both offer excellent control of intractable vertigo. However, patients undergoing translab yrinthine vestibular nerve section are more likely to show improvement in imbalance and functional disability. This outcome is more likely for diagnoses other than Meniere’s disease. There are potential prognostic factors that can be helpful in the preoperative or postoperative counseling of patients undergoing surgical treatment of vertigo. Patients who rate themselves as more disabled before surgery are less likely to achieve the best outcomes. Several other factors, such as duration of disease, contralateral tinnitus, eye disease, and allergy, may play a role.
Surgery has long been used to control disabling vertigo of Meniere’s disease and other peripheral vestibular disorders refractory to medical measures, with each surgical procedure having many technical variations.
The history of vestibular nerve section (VNS) was recently reviewed. It was first attempted in 1898, with microscopic technique later introduced by William House in 1960. The retrolabyrinthine and retrosigmoid-internal auditory canal (IAC) approaches for VNS were popularized in the 1980s. Transmastoid labyrinthectomy, the gold standard surgical technique for complete removal of all neuroepithelial elements of the ear causing disabling disequilibrium, was described as early as1904. When properly performed, transmastoid labyrinthectomy eliminates all vestibular function in the diseased periphery, but at the expense of any remaining cochlear function. Another common treatment option for patients with intractable Meniere’s disease, endolymphatic sac (ES) surgery, has stood the test of time for 75 years. House described and popularized endolymphatic sac surgery (the shunt procedure) in the early 1960s.
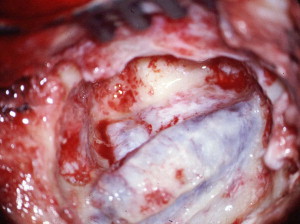
For patients with unilateral disease, the procedures of choice are endolymphatic mastoid shunt ( Figs. 1 and 2 ) and vestibular nerve section (translabyrinthine, retrolabyrinthine, retrosigmoid and middle cranial fossa VNS) ( Fig. 3 ). These procedures are preferred over labyrinthectomy ( Fig. 4 ) because cochlear nerve integrity is preserved, leaving open the possibility of future cochlear implantation should bilateral profound hearing loss develop.


Telischi and Luxford published statistically valid long-term results in endolymphatic sac surgery. This procedure is recommended as the surgical procedure of first choice. Sixty-three percent of patients undergoing sac surgery do not require further surgical procedures and an additional 17% have only revisions of the endolymphatic sac shunt. Thus, 80% never require a destructive procedure and 93% report no further dizziness or mild to no disability 13.5 years later. The sac procedure has only a 2% risk of hearing loss or hearing worsening. Patients who fail sac procedures, or who are severely symptomatic, show a 90% vertigo cure rate to vestibular neurectomy.
Surgical management
Several procedures are available for the surgical treatment of Meniere’s disease. The surgeon should take into consideration severity of disease, hearing status, and presence of unilateral versus bilateral disease when selecting an approach.
Endolymphatic drainage procedures can be divided into external shunts that attempt to drain excessive endolymph from the endolymphatic sac into the mastoid or subarachnoid space (ie, endolymphatic sac shunt) and internal shunts that attempt to drain excessive endolymph into the perilymphatic space (ie, cochleosacculotomy [labyrinthotomy]).
Approaches that transverse the labyrinth, such as labyrinthectomy and translabyrinthine vestibular neurectomy, sacrifice hearing and are useful in patients without useful hearing. Posterior approaches that spare the labyrinth (retrolabyrinthine and retrosigmoid vestibular neurectomy) provide varying degrees of cerebellopontine angle (CPA) exposure with an opportunity for hearing preservation. Superior approaches permit unroofing of the IAC and an opportunity for hearing preservation, such as middle fossa vestibular neurectomy; however, this procedure has fallen out of favor because of increased risk for facial nerve injury or transient palsy, compared with the other approaches.
Endolymphatic Sac Shunt
A postauricular incision is made approximately 2 cm posterior to the sulcus, and the mastoid cortex is cleaned of periosteal soft tissues. A routine mastoidectomy is performed and then extended to include dissection to at least 1 cm posterior to the sigmoid sinus. Additional bone removal is done so that the dura of the posterior fossa is skeletonized from the sigmoid sinus posteriorly to the posterior semicircular canal anteriorly and the endolymphatic sac inferiorly. Exposure of the posterior fossa dura is extended toward the jugular bulb and into the retrofacial air cells, allowing a large decompression of the sac (see Fig. 1 ). The sac is carefully entered with a sharp hook and the lumen identified by its glistening character. The lumen is widely opened with a long, blunt, right-angle hook with specific attention toward the duct. A T-shaped silastic is placed into the lumen (see Fig. 2 ). The wound is closed by use of subcutaneous absorbable sutures followed by skin sutures.
Cochleosacculotomy (Labyrinthotomy)
Cochleosacculotomy is performed under local anesthesia and is the procedure of choice for patients who, for health reasons, are at risk from the stress of postoperative vertigo and who should not have general anesthesia, as well as for elderly patients who often compensate poorly to procedures that ablate vestibular function. It has the advantage of being technically simple to perform, is almost totally free of morbidity, and carries little or no risk of mortality. However, it results in sensorineural hearing loss, and is therefore usually used in patients with preexisting severe-to-profound sensorineural hearing loss.
The cochleosacculotomy operation consists of creating a fracture disruption by impaling the osseous spiral lamina and cochlear duct with a pick introduced through the round window. Usually, the round window niche accommodates a 3-mm right-angle pick without removal of bone. The pick is advanced through the round window membrane, which may or may not be visible. The pick is guided in the direction of the oval window while hugging the lateral wall of the inner ear to ensure that the cochlear duct is traversed. When the pick has been introduced to its full 3-mm length, the end of the pick will be located beneath the footplate of the stapes. Occasionally, the subiculum, which is a ridge of bone lying in the boundary between the round window niche and sinus tympani, interferes with introduction of the pick. It can readily be shaved down with a 2-mm burr. Occasionally, the overhanging bony lip of the round window niche must be removed to accommodate the pick. In this case, a 2-mm (rather than a 3-mm) pick is used to avoid excessively deep penetration into the vestibule and possible injury to the utricular macula. Rarely, a high jugular bulb blocks access to the round window niche, in which case it may be necessary to abort the operation.
The pick is withdrawn and the perforation in the round window membrane is sealed by a tissue graft of perichondrium or adipose tissue. The operation is terminated by returning the tympanomeatal flap to its original position. A piece of Gelfoam is placed in the canal to maintain slight pressure on the skin flap. Cotton is placed in the ear canal.
Labyrinthectomy
An incision is made approximately 1 cm above and behind the postauricular crease and follows the contour of the auricle. A plane is established in the galea aponeurotic layer lateral to the temporalis muscle and the auricle is turned forward. A thick periosteal flap is created by incising this tissue along the linear temporalis just anterior to the incision line and then inferior to the mastoid tip. This flap is elevated off the mastoid cortex and retracted forward with a large self-retaining retractor. The staggered two-layer incision provides better closure to prevent cerebrospinal fluid leaks.
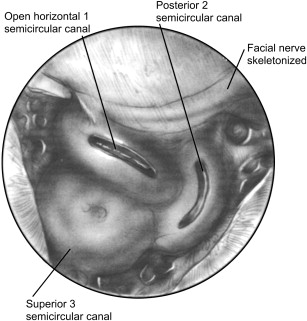
The high-speed drill with a large cutting burr and constant suction irrigation is used to perform a cortical mastoidectomy. The posterior external bony canal wall is thinned, the bone over the tegmen is thinned, and the sigmoid sinus is skeletonized. The bone over the sinus is frequently eggshelled and decompressed by collapsing it with thumb pressure, leaving tiny, fragmented pieces of bone over the highly vulnerable sigmoid sinus to protect it from damage from instruments entering and exiting the wound (see Fig. 3 ). The sinus is easily collapsed and gives needed exposure medially. The sinodural angle is opened as far back on the cortex as possible. Because the vestibule lies under the facial nerve anteriorly, an angulated view via the sinodural angle is necessary to visualize the contents of the vestibule and eventually identify landmarks used to excise the superior vestibular nerve.
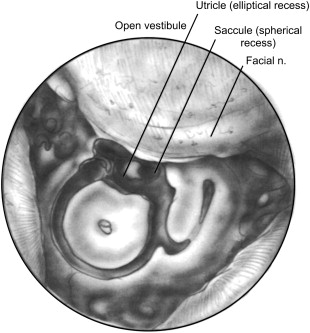
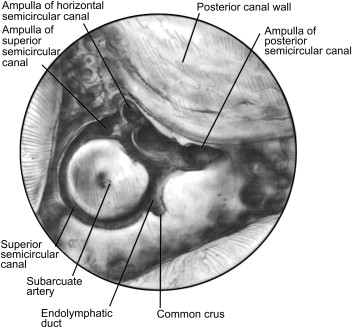
Bone over the posterior fossa dura is thinned out but not removed. The labyrinth is skeletonized and the cells of the mastoid tip are opened. The labyrinthectomy is performed by opening the crown of the lateral (horizontal) semicircular canal on its posterior border and following the half-opened canal posteriorly to the posterior canal. The lateral canal is only half opened to protect the external genu of the facial nerve until careful trimming can be done. The posterior canal, having been opened, can be traced to its confluence with the superior semicircular canal, where the two canals combine to become the common crus (see Fig. 4 ). The common crus may then be followed directly forward to the vestibule ( Fig. 5 ).
The posterior surface of the facial nerve over the external genu is now thinned carefully, and the anterior limb of the posterior canal is followed to its ampulla at the inferior pole of the elliptical recess. The lateral canal is opened anteriorly and medially to its ampullated end, and the ampulla of the superior canal identified next to that of the lateral is opened. The superior canal is opened along the tegmen throughout its course, which curves back to the common crus.
With all the canals and the vestibule opened, all soft-tissue elements of the membranous labyrinth should be removed. This step would be the normal end point of the postauricular, postganglionic labyrinthectomy but only sets the stage to skeletonize the IAC in a translabyrinthine vestibular nerve section and preganglionic denervation ( Fig. 6 ).
Translabyrinthine Vestibular Neurectomy
A mastoidectomy and labyrinthectomy are performed as previously described under labyrinthectomy. A key factor in successful exploration of the IAC is clear identification of the IAC contents. Identification is possible only if the soft-tissue contents are not violated in the removal of bone during IAC skeletonization. Loss of part or all of any of the soft-tissue landmarks places all the other contents at great risk because of the difficulty in differentiating the nerves from one another. The purpose in using the facial nerve-vestibular nerve tissue plane when dissecting the IAC is to enable identification of the facial nerve in its normal position and extend the dissection into the diseased area, where those relationships are sometimes more difficult to ascertain.
A useful technique for IAC skeletonization is blue lining the IAC throughout the area to be opened. The thin bony cover protects the soft-tissue structures within the IAC. Blue lining actually starts at the vestibule because this is where the bone is the thinnest. The nerves of the IAC exit into the bony labyrinth through perforations in the thin bone separating the fundus of the IAC from the vestibule. This naturally blue-lined area can be used as a starting point for skeletonization of the remainder of the canal. Removal of bone should extend to the porus acusticus and should cover 180° of the lateral side of the canal. The general orientation of the IAC is that the fundus is lateral just medial to the vestibule. The superior border is along a line drawn between the superior semicircular canal ampulla and the sinodural angle, and the inferior border is along the line starting at the posterior semicircular canal ampulla drawn posteriorly parallel to the superior border. The IAC angles away from the surgeon in an anterolateral-to-posteromedial direction deep to the sigmoid sinus ( Fig. 7 ).




