12 Endocrine Disorders
Parathyroid Overview
1 | How common is a supernumerary parathyroid gland, and where is the supernumerary gland most likely to be found? ( | The incidence of a supernumerary parathyroid gland is up to 15%. They are most often found in the thymus, thyrothymic tract, and carotid sheath. |
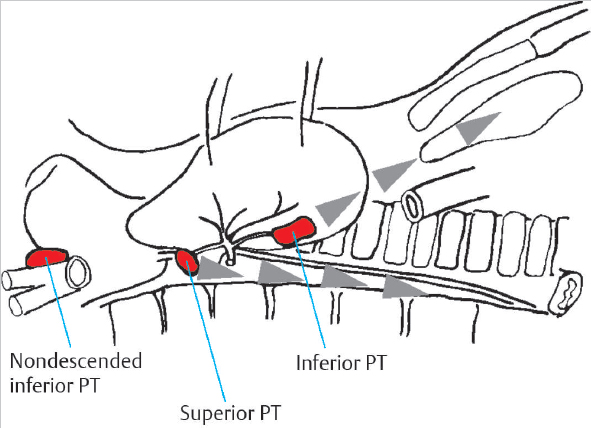
Fig. 12.1 Most common locations of the superior and inferior parathyroid glands and the course of their embryological migration. (Used with permission from Gemsenjaeger E. Atlas of Thyroid Surgery: Principles, Practice, and Clinical Cases. New York, NY: Thieme; 2009.)
2 | Where do the superior and inferior parathyroid glands obtain their blood supply? | Most of the blood supply comes from the inferior thyroid artery, although occasionally the superior glands may get their blood supply from the superior thyroid artery (in 15% of cases). |
3 | What options are available for minimally invasive parathyroidectomy? | Minimally invasive parathyroidectomy is gaining popularity among surgeons. Typically, a technetium-99 sestamibi scan preoperatively determine a single hyperfunctioning parathyroid adenoma, and exploration of that gland alone is done using intravenous (IV) sedation and intraoperative parathyroid hormone assay monitoring. |
4 | When conducting a subtotal parathyroidectomy, what tissue should be left behind? | Approximately three and one-half glands should be excised and the remaining half of a gland left to its blood supply. Most prefer to leave a portion of an inferior parathyroid gland because there would less risk to the recurrent laryngeal nerve. |
5 | How can PTH levels be used intraoperatively to determine the completeness of a parathyroidectomy? | PTH has a half-life of 2–5 minutes, so PTH levels can be drawn from the patient before incision and then 5 to 10 minutes after excision. If there is at least a 50% decrease in the PTH level, into the normal or near normal range, the excised gland was likely the offending gland. |
6 | What structures have been described as landmarks to identify the superior parathyroid gland? | About 80% of superior parathyroid glands are found on the posterior aspect of the thyroid gland within a 1-cm diameter centered 1 cm superior to the intersection of the recurrent laryngeal nerve and inferior thyroid artery. |
What branchial pouch gives rise to the superior and inferior parathyroid glands? ( | The fourth branchial pouch gives rise to the superior parathyroid gland and C cells. The third branchial pouch gives rise to the inferior parathyroid gland and thymus. |
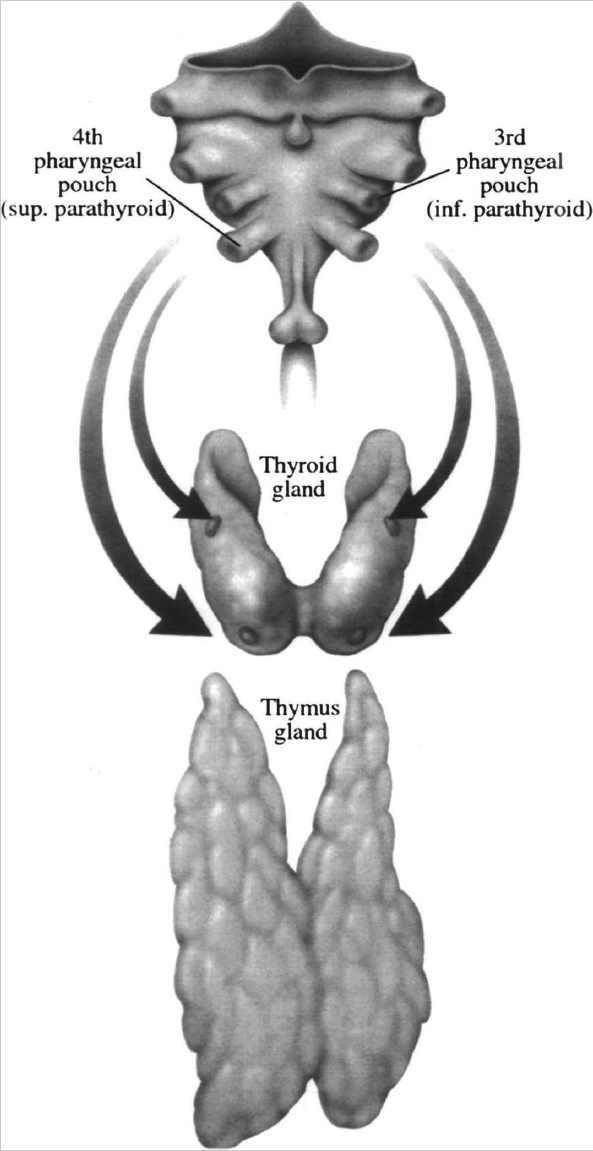
Fig. 12.2 The embryologic origin of the parathyroid glands. (Used with permission from Terris DJ, Gourin CG, eds. Thyroid and Parathyroid Diseases: Medical and Surgical Management. New York, NY: Thieme; 2009.)
How does PTH maintain calcium levels? | PTH increases calcium absorption from the gut, mobilizes calcium from the bones, inhibits calcium excretion from the kidneys, and stimulates renal hydroxylase to maintain activated vitamin D levels. | |
9 | What is the most potent regulator of PTH release? | Serum calcium levels |
10 | Where can one find PTH receptors, and what downstream effects do they have in each location? | PTH binds to PTH receptors in two locations: bone and kidney. In bone, PTH receptors on osteoblasts cause release of receptor activator of nuclear factor-κ ligand, which then activates osteoclasts, which break down bone to increase serum calcium. In the kidney, PTH binds to renal tubule cells and induces reabsorption of calcium and decreases reabsorption of phosphate from the filtrate. It also induces the expression of an enzyme that converts the inactive form of vitamin D (25-hydroxyvitamin D) to the active form (1,25-dihydroxyvitamin D). |
11 | When monitoring total calcium levels in a patient, what factor do you also need to note? | Albumin level. Total calcium can vary with albumin level. In a patient with normal albumin, total calcium can be monitored. In a patient with abnormal albumin levels, the corrected total calcium can be calculated (total serum calcium decreases by 0.8 g/dL for every 1-g/dL decrease in albumin), or the ionized calcium level can be followed. |
12 | What test results support the diagnosis of familial hypocalciuric hypercalcemia? | Hypercalcemia with 24-hour urinary calcium:creatinine clearance ratio below 0.01, as well as one or more first-degree relatives with hypercalcemia |
13 | What are common symptoms of chronic hypercalcemia? | The symptoms of chronic hypercalcemia can be remembered by the mnemonic “bones, stones, abdominal groans, and psychiatric moans,” referring to renal calculi, bone pains, abdominal pain, and depression, anxiety, cognitive dysfunction or other psychiatric problems. |
14 | What testing is necessary to diagnose primary hyperparathyroidism? | Elevated albumin-corrected serum calcium or ionized calcium and elevated PTH. Imaging serves as an adjunct but is not part of the diagnostic criteria of primary hyperparathyroidism. |
15 | Name the most common cause of hypercalcemia in an outpatient clinic setting. | Parathyroid adenoma |
16 | Name the most common cause of hypercalcemia in an inpatient hospital setting. | Underlying malignancy |
17 | A patient has hypercalcemia and low or undetectable PTH levels. What is the likely diagnosis? | Primary hyperparathyroidism is ruled out by the low or undetectable PTH level. This patient likely has a paraneoplastic-induced hypercalcemia mediated by PTH-related protein. |
18 | What is the incidence of primary hyperparathyroidism in Western countries? | 22 cases per 100,000 persons per year The incidence has increased since the 1970s because of increased detection of asymptomatic patients with elevated calcium levels. In postmenopausal women, the most common demographic, the incidence may be as high as 1 per 1,000/year. |
19 | What are the different types of parathyroid hyperplasia? | Parathyroid hyperplasia is predominantly caused by proliferation of the chief cells within the gland. Very rarely, water clear cell hyperplasia, which is a proliferation of vacuolated water clear cells, can be found. The water clear cell variant is clinically more severe and predominantly occurs in females. |
Describe the typical patient population with primary hyperparathyroidism. | Most cases occur in women (74%); incidence peaks in the seventh decade of life. Before age 45, incidence in men and women is similar. | |
21 | What causative factors are associated with primary hyperparathyroidism? | • Head and neck radiation in childhood • Long-term lithium therapy • Genetic predisposition |
22 | What are the guidelines for surgical treatment (parathyroidectomy) in an asymptomatic patient with primary hyperparathyroidism? | Despite being devoid of classic symptoms, some patients should be treated for hyperparathyroidism, including those with serum calcium greater than 1.0 mg/dl above the upper limit of the normal reference range, those with a calculated creatinine clearance less than 60 ml/minute, those with bone mineral density T score less than –2.5 at any site or previous fragility fracture. Patients younger than 50 years should also be considered to prevent long-term damage from elevated calcium. |
23 | What are the typical laboratory values of calcium, PTH, and phosphate in secondary hyperparathyroidism? | In secondary hyperparathyroidism, one would expect low-normal calcium and elevated PTH. Phosphate levels vary based on the etiology (high in renal insufficiency, low in vitamin D deficiency). |
24 | What are some possible causes of secondary hyperparathyroidism? | Secondary hyperparathyroidism can occur from renal failure, which causes a decline in the formation of activated 1,25 vitamin D and calcium absorption in the gut. Phosphate excretion is also impaired, which together cause low serum calcium. It can also result from low vitamin D levels in the setting of adequate renal function, such as in cases of dietary insufficiency. In addition, patients with short gut syndrome or a history of gastric bypass surgery are at risk for secondary disease resulting from malabsorption of both calcium and vitamin D. In all cases, low serum calcium triggers secretion of PTH and growth of the parathyroid glands. |
25 | What is the treatment of secondary hyperparathyroidism? | • Correction of the underlying cause, such as renal transplant in patients with renal failure or vitamin D therapy in vitamin D deficiency • Patient symptoms from secondary disease may improve with medications such as cincalcet or bisphosophate therapy. • There is a role for subtotal parathyroidectomy if medical management fails. |
26 | What is tertiary hyperparathyroidism? | Tertiary hyperparathyroidism is a state of excess secretion of PTH after long-standing secondary hyperparathyroidism. Phosphate levels in tertiary hyperparathyroidism are decreased; however, renal dysfunction may lead to hyperphosphatemia despite elevated PTH levels. A classic example is hyperparathyroidism persisting after renal transplantation. |
27 | What is the pathophysiology of tertiary hyperparathyroidism? | The hypertrophied parathyroid glands become autonomous in their function and hypersecrete PTH, leading to hypercalcemia despite withdrawal of calcium and calcitriol. High calcium levels can cause diffuse calcinosis. |
28 | What is the treatment of tertiary hyperparathyroidism? | Total parathyroidectomy with autotransplantation or subtotal parathyroidectomy (3 and ½ gland resection) |
29 | What are the components of hyperparathyroidism-jaw tumor syndrome? | Recurrent parathyroid adenomas, fibroosseous tumors of the mandible, and Wilms tumors |
How do the symptoms of acute and chronic hypoparathyroidism differ? | Acute hypoparathyroidism, such as after surgery, can cause dramatic hypocalcemia and associated paresthesias, muscle spasms, tetany, and seizures. The hypocalcemia induced by chronic hypoparathyroidism is gradual in onset and may not present until the patient develops blurry vision from cataracts. | |
31 | What are the most common causes of hypoparathyroidism? | By far, the most common cause of hypoparathyroidism is iatrogenic, by either treatment of hyperparathyroidism or injury during thyroid surgery. The next most common causes are congenital, when the third and fourth branchial arches fail to develop properly. |
Parathyroid Tumors
32 | What is the histologic description of a parathyroid adenoma? | A parathyroid adenoma appears as a hypercellular gland consisting of chief and oncocytic cells with decreased intercellular fat. |
33 | What are some intraoperative techniques used to identify a parathyroid adenoma? | Localization of an adenoma can be assisted by preoperative injection of methylene blue, which stains abnormal parathyroid glands preferentially. Preoperative injection of sestamibi in conjunction with intraoperative gamma probes can also be used to identify a parathyroid gland. |
34 | What is the most sensitive imaging study for identifying the location of a parathyroid adenoma? | Technetium-99 m sestamibi with single-photon emission CT (or SPECT; sensitivity from 70 to 100%). Ultrasound imaging is reported to be successful in localization in 50 to 90% of cases but is highly user dependent. 4D CT scan is an emerging technology, but the localization success rate remains to be determined. |
35 | How frequently is primary hyperparathyroidism caused by a single adenoma versus four-gland hyperplasia? | A single parathyroid adenoma is the cause in 80 to 85% of cases and four-gland hyperplasia in 10 to 15% of cases. Other causes of primary hyperparathyroidism include double adenomas (5%) and parathyroid carcinoma (< 1%). |
36 | What features of a patient with hypercalcemia and elevated PTH are more concerning for a parathyroid carcinoma compared with benign parathyroid adenoma? | Aside from a palpable neck mass, other features worrisome for parathyroid carcinoma include markedly elevated serum calcium levels (> 14), markedly elevated PTH, concomitant renal and bone disease, symptoms consistent with severe hypercalcemia, and evidence of invasion such as recurrent laryngeal nerve palsy. |
37 | What proportion of primary hyperparathyroidism is caused by parathyroid carcinoma? | About 0.1 to 1% of persons with primary hyperparathyroidism have a parathyroid carcinoma. |
38 | What are the incidence and prevalence of parathyroid carcinoma? | Parathyroid carcinoma is one of the rarest of all human cancers, with an incidence of 0.015 per 100,000 population and a prevalence of 0.005% in the United States. |
39 | How does the patient population with parathyroid carcinoma compare with patients with parathyroid adenoma? | There is an even distribution of males and females with parathyroid carcinoma, whereas there is female predominance in parathyroid adenoma. Patients on average are younger with parathyroid carcinoma (average age in 40s) compared with parathyroid adenoma (average age 50 to 60s). |
40 | What feature on physical examination is most concerning for parathyroid carcinoma? | A palpable neck mass (reported in 30 to 76% of patients with parathyroid carcinoma), which is rarely associated with a benign adenoma |
41 | What is the gross pathologic description of a parathyroid carcinoma compared with a benign adenoma? | Benign adenomas are generally soft, round, or oval and reddish brown. Parathyroid carcinoma is frequently a large, lobulated, and firm to stony-hard mass, with a grayish white capsule that is frequently adherent or invasive to surrounding tissues. |
What is the American Joint Committee on Cancer (AJCC) staging system for parathyroid carcinoma? | There is no AJCC staging system for parathyroid carcinoma because of its low incidence. | |
43 | What is the most common cause of death in patients with parathyroid carcinoma? | Patients often die from the effects of excessive PTH secretion and uncontrolled hypercalcemia rather than growth from tumor mass. |
44 | What is the best prognostic factor in parathyroid carcinoma? | Early recognition and complete surgical resection at initial operation offer the best prognosis. |
45 | Describe the prognosis for parathyroid carcinoma. | Surgical cure and survival can be achieved in patients undergoing an R0 (complete) resection. Patients with recurrent disease can be palliated with aggressive surgical therapy and calcimimmetic medications such as cincalcet. |
46 | What is the preferred treatment approach to parathyroid carcinoma? | Parathyroid carcinoma should be aggressively treated with en bloc resection of the tumor, ipsilateral central neck components, including thyroid lobectomy, tracheoesophageal soft tissue, and central lymph node dissection. |
47 | What is the most common pattern of malignant spread of disease in parathyroid carcinoma? | Parathyroid carcinoma is generally indolent with local recurrence and involvement of contiguous neck structures representing the most likely pattern of spread. |
48 | What is the rate of recurrence in parathyroid carcinoma? | About 40 to 60% of patients have a postsurgical recurrence, which usually occurs 2 to 5 years after surgery. |
49 | In a patient with recurrent and widely disseminated parathyroid carcinoma, surgical resection is no longer effective. Therapeutic goals should be control of hypercalcemia and decreasing bone resorption. How can this be treated medically? | Aggressive hydration restores fluid volume and increases urinary calcium excretion. Loop diuretics increase calciuresis. Bisphosphonates interfere with osteoclast-mediated bone resorption. |
50 | What is the pattern of metastatic disease in parathyroid carcinoma? | Late metastases occur via both lymphatic and hematogenous spread with the most common site being the lungs. |
Thyroid Overview
51 | From what branchial structures does the thyroid develop? | The thyroid develops from an endodermal diverticulum of the floor of the primitive pharynx. The medial primordia is derived from the first and second pharyngeal pouches. The lateral primordia is derived from the fourth and fifth pharyngeal pouches. |
52 | The ultimobranchial bodies develop into what structures? | Ultimobranchial bodies derive from the fourth pharyngeal pouch neural crest cells and give rise to parafollicular cells (C cells) of the thyroid, which release calcitonin. |
53 | What is the relationship of the ultimobranchial bodies to the thyroid gland? | The ultimobranchial bodies fuse with the thyroid gland during its descent, consistently in the middle to upper thirds of thyroid gland. |
54 | What is the most common pattern of descent of the thyroid gland in relation to the hyoid bone? ( | The thyroid gland descends anterior to the hyoid bone during gestational weeks 4 through 7. |
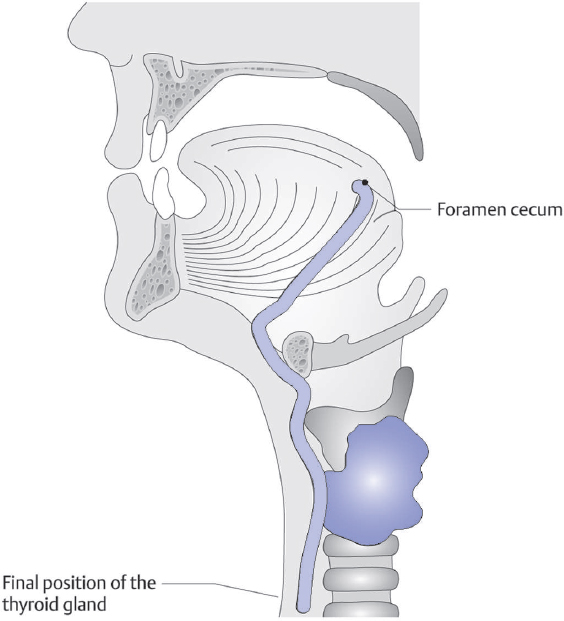
55 | What is the most common location of ectopic thyroid tissue? | As the thyroid forms from an endodermal diverticulum of the pharynx, the most common location of ectopic thyroid tissue is found in the base of tongue (lingual thyroid). |
56 | What does the proximal portion of the thyroglossal duct form? | Foramen cecum of the tongue |
57 | What does the caudal remnant of the thyroglossal duct form? | Pyramidal lobe of the thyroid, which is present in 40 to 55% of patients |
58 | What is the recommended surgical treatment for a thyroglossal duct cyst? | The Sistrunk procedure, which includes complete removal of the thyroglossal duct along with a portion of the central hyoid bone |
59 | What is the most common path of the right and left recurrent laryngeal nerves? | The right recurrent laryngeal nerve wraps around and passes deep to the right subclavian artery. It then travels in a more oblique path to enter the larynx just posterior to the cricothyroid joint. The left recurrent laryngeal nerve wraps around and passes deep to the arch of the aorta. The nerve then travels in a more medial path within the tracheoesophageal groove. |
60 | What does the recurrent laryngeal nerve innervate? ( | The intrinsic muscles of the larynx and sensory innervation of the glottis (shared innervation with internal branch of superior laryngeal nerve) and subglottis |
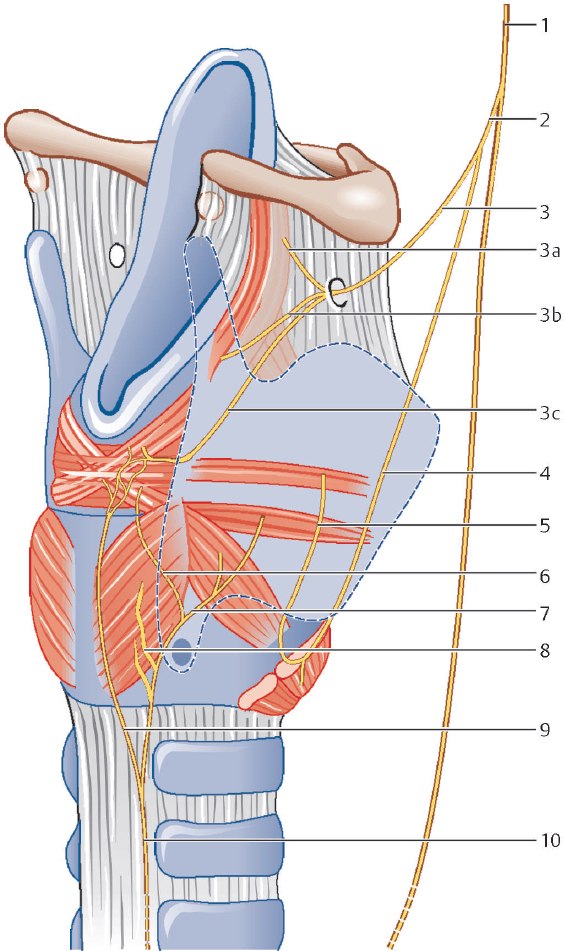
61 | What is the relationship of the recurrent laryngeal nerve and the cricothyroid joint? | The recurrent laryngeal nerve enters the larynx posterior to the cricothyroid joint. |
62 | What does the external branch of the superior laryngeal nerve innervate? | The cricothyroid muscle |
63 | What is the function of the cricothyroid muscle? | The cricothyroid increases tension on vocal cords, inducing a higher pitch when vocalizing, and is innervated by the superior laryngeal nerve. |
64 | What does the internal branch of the superior laryngeal nerve innervate? | The internal branch of the superior laryngeal nerve pierces the thyrohyoid membrane to enter the larynx. The superior laryngeal nerve provides sensation to the supraglottic structures and shares sensation of the glottis with the recurrent laryngeal nerve. |
Where does the superior laryngeal nerve branch off from the vagus? | Immediately below the nodose ganglion (inferior ganglion) of the vagus nerve, which is located just inferior to the jugular foramen | |
66 |



