Fig. 15.1
(a) Color fundus photograph of the left eye of a diabetic patient with West Nile virus infection shows inactive multifocal chorioretinitis with a linear clustering of chorioretinal lesions. (b) Fluorescein angiogram of the same eye shows central hypofluorescence and peripheral hyperfluorescence of chorioretinal lesions, arranged in linear/curvilinear streaks. There are also features of nonproliferative diabetic retinopathy
Chorioretinal lesions may vary in number and size, involving the midperiphery, with or without associated posterior pole involvement [5]. Linear clustering of chorioretinal lesions is a prominent feature of WNV-associated chorioretinitis. Streaks are oriented radially in the nasal and peripheral fundus and in a curvilinear pattern in the temporal posterior fundus. The linear pattern of chorioretinitis follows the course of retinal nerve fibers, suggesting a contiguous spread of central nervous system disease [27]. Indocyanine green (ICG) angiography reveals well-delineated hypofluorescent choroidal lesions, which are more numerous than those appreciated by FA or clinically [28].
A case of reactivation of WNV infection-related chorioretinitis has been recently reported, with appearance of new active lesions exhibiting a typical pattern almost 1 year after the initial diagnosis was made [29].
Although multifocal chorioretinitis is the most common ocular manifestation of WNV infection, other findings can occur including anterior uveitis, retinal vasculitis, which may be occlusive in nature, retinitis, segmental zones of atrophy and mottling of the retinal pigment epithelium, optic nerve involvement, ocular nerve palsy, nystagmus, and congenital chorioretinal scarring [5, 7–26].
WNV-associated ocular disease usually has a self-limited course, and visual acuity returns to baseline in most patients. However, persistent visual impairment can occur due to a foveal chorioretinal scar, choroidal neovascularization, vitreous hemorrhage secondary to retinal neovascularization, severe ischemic maculopathy, macular edema, optic atrophy, or retrogeniculate damage [5, 14–16, 18–21, 25].
15.2.3 Laboratory Diagnosis
Antibody-capture enzyme-linked immunosorbent assay (MAC-ELISA) for the detection of WNV-specific IgM antibody in serum and/or cerebrospinal fluid is a very sensitive diagnostic method. Almost all patients have detectable IgM antibodies by 7–8 days after the onset of the disease, whereas WNV-specific serum IgG antibodies are detectable only by 3 weeks after the infection. The plaque-reduction neutralization test can help distinguish false-positive results of MAC-ELISA or other assays, and serologic cross-reactions among the flaviviruses. A fourfold or greater increase serum antibody titer in serum samples collected 2–3 weeks apart may be used to confirm the diagnosis of WNV infection, as IgM may persist in the serum for more than a year [30].
Furthermore, detection of viral nucleic acid by real-time reverse transcription polymerase chain reaction (RT-PCR) is highly specific for WNV infection, but it is less sensitive than serology. PCR test is mostly used in the screening of blood products. Viremia often lasts for several days and the virus itself is usually no longer detectable in the serum by the time WNV-specific serum IgM appears [4, 30].
15.2.4 Management
There is currently no effective treatment for WNV infection. In cases of severe systemic disease, intensive supportive therapy is indicated, often involving hospitalization, intravenous fluids, respiratory support, prevention of secondary infections, and good nursing care [6]. Antiviral agents such as ribavirin, interferon α 2b and interferon β, and intravenous immunoglobulins have shown to reduce viral replication in vitro or in animal models [6, 31–34]. However, their efficacy is still to be proven in humans.
Prevention remains the mainstay of WNV infection control. Measures to reduce the number of mosquitoes (draining standing water, larvicides) as well as personal protection (repellents, window screens, protective clothing) are recommended [35]. Widespread vaccination of horses in the USA has led to decreasing the incidence of equine infections [6]. Vaccine for human use is still in the research phase.
Specific ophthalmic treatment may be required including topical steroids for anterior uveitis, peripheral scatter retinal photocoagulation for neovascularization secondary to occlusive retinal vasculitis, pars plana vitrectomy for non-clearing vitreous hemorrhage or tractional retinal detachment, and intravitreal injection of anti-VEGF for choroidal neovascularization or macular edema [16, 36].
15.3 Dengue Fever
15.3.1 Introduction
Dengue fever (DF) is caused by any of the four immunologically related serotypes of the dengue virus, which belongs to the genus Flavivirus of the family Flaviviridae. It is transmitted through the bite of an infected female Aedes aegypti/albopictus mosquito. Aedes albopictus vector seems to produce a slow-moving outbreak by contrast to the sharp epidemics associated with Aedes aegypti [37].
DF is considered to be one of the most important arthropod-borne disease in the tropical and subtropical regions, being endemic in more than 100 countries, including America, Southeast Asia, Western pacific, Africa, and the Eastern Mediterranean [38]. The spectrum of systemic disease may range from mild flulike illness to life-threatening clinical presentations. Ocular involvement was found to occur in 10 % of patients hospitalized for serologically confirmed DF [39–43].
15.3.2 Clinical Symptoms and Signs
15.3.2.1 Systemic Disease
The incubation period for DF varies from 3 to 14 days. The initial infection may be asymptomatic, may result in a nonspecific febrile illness, or may produce features of classic DF including sudden onset of high fever, severe headache, myalgias, arthralgias, nausea, vomiting, and a maculopapular rash. The majority of DF cases are self-limiting. A small proportion of affected patients may develop life-threatening dengue hemorrhagic fever syndrome, which is characterized by increased capillary permeability and hemostatic disturbances, or dengue shock syndrome, which is characterized by severe systemic hypotension. DF is often associated with a bleeding tendency secondary to thrombocytopenia [37, 44].
15.3.2.2 Ocular Disease
The ocular involvement usually occurs within 1 month after the onset of symptoms of DF and is often bilateral. The patients may present with a sudden decrease in vision, a central scotoma, or floaters [45]. A subconjunctival hemorrhage, petechial in type and associated with a platelet count of less than 50.000/μl, was the most common ocular manifestation in an East Indian population with DF [46]. Numerous posterior segment changes have been associated with DF including retinal hemorrhages, retinal vasculitis, yellow subretinal dots, retinal pigment epithelium mottling, and foveolitis, seen clinically as a round yellowish lesion at the fovea with corresponding focal outer neurosensory retina – retinal pigment epithelium thickening on OCT (Fig. 15.2). Other findings include macular edema, serous retinal detachment, retinal vascular occlusion, choroidal changes, optic disk swelling, optic neuritis, and neuroretinitis [1–3, 41, 42, 44, 45, 47–56].
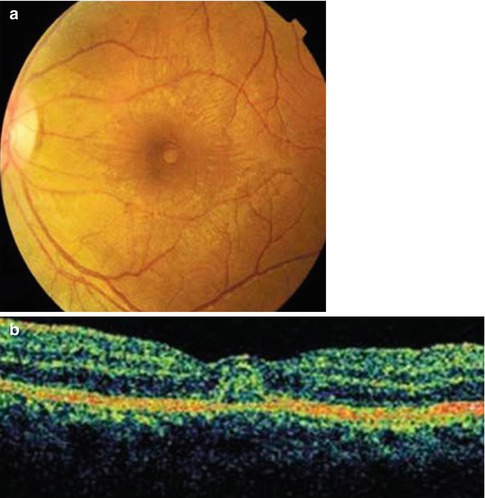
Fig. 15.2
(a) Color fundus photograph of the left eye of a patient with dengue fever shows a round yellowish lesion at the foveal center. (b) OCT of the same eye reveals a corresponding focal thickening of outer neurosensory retina – retinal pigment epithelium. These findings are consistent with foveolitis (Courtesy, Soon Phaik Chee)
15.3.3 Laboratory Diagnosis
Within the first 2 days of fever, diagnosis is possible only by detecting virion, RNA, or dengue proteins, such as nonstructural protein 1 (NS1). In fact, NS1 antigen is usually detected in blood, from day 1 to day 9 of infection [37, 58].
Detection of newly formed antibodies (IgM) usually is not possible until after viremia ends or after fever subsides. MAC-ELISA has become a widely used assay, but it seems to have a high rate of false-positive results [59]. Other tests including immunochromatographic assay, complement fixation, neutralization test, hemagglutination inhibition, and IgG enzyme-linked immunosorbent assay (ELISA) are also helpful to confirm the diagnosis of DF [58].
Apart from the dengue-specific parameters, platelet count is a simple and available laboratory test that can support the diagnosis of dengue hemorrhagic fever or dengue shock syndrome.
15.3.4 Management
To date, there is no specific treatment available for dengue virus infection. Fever can be treated by antipyretics, but drugs such as acetylsalicylic acid and other nonsteroidal anti-inflammatory drugs should be avoided as they may worsen the bleeding tendency. Any medicine that decreases the platelet level should be avoided [37, 42]. In cases of dengue hemorrhagic fever, hospitalization, prompt treatment with intravenous fluids and close monitoring of vital signs, as well as hematologic parameters are indicated [37].
Preventive measures by avoiding contact with infected mosquitoes are required to decrease the infection incidence. Vaccines targeting all the four serotypes of dengue virus hopefully will be available in the near future [60].
There is no established treatment for ocular manifestations of DF. Topical, periocular, intravitreal, oral, and intravenous steroids, as well as intravenous immunoglobulins, have been advocated for the management of dengue ocular complications, based on the postulated immune-mediated pathogenesis of the disease. Indications for treatment may include dengue-associated uveitis and optic neuritis, visual acuity worse than 20/40, and deterioration of vision [45, 46].
15.4 Chikungunya
15.4.1 Introduction
Chikungunya virus is a single-stranded RNA virus of the genus Alphavirus of the family Togaviridae which is transmitted to humans by the bite of infected Aedes mosquitoes (A. Aegypti and A. albopictus). Since its first isolation in Tanzania in 1953, the virus has been associated with many epidemics in tropical regions of Africa, India, Southeast Asia, and South America. The infection which is endemoepidemic typically consists of an acute illness with fever, severe arthralgia, and skin rash [61]. Ocular involvement is relatively uncommon. The main ocular manifestations associated with Chikungunya virus infection are anterior uveitis and retinitis.
15.4.2 Clinical Symptoms and Signs
15.4.2.1 Systemic Disease
The incubation period ranges from 1 day to 12 days, with an average of 2–4 days. Onset of the disease is abrupt and is characterized by high fever, severe arthralgia and myalgia, along with headache and skin rash. Asymptomatic infections are rare (3–25 % of serologically proven infections) [62]. The debilitating polyarthralgia is very characteristic of Chikungunya. Joint pain often disappears in few weeks, but may persist for months or years in some patients [63, 64]. Skin lesions may be seen in almost one half of the patients. A pruriginous maculopapular rash, lasting for 2–3 days, is the most common feature [63–65]. Rarely, severe infection associated with multiorgan failure, central neurological involvement, neonatal infection, and death occurs [63, 64, 66].
15.4.2.2 Ocular Disease
Ocular manifestations associated with Chikungunya may be concomitant of the systemic disease or may follow its resolution [67]. Ocular involvement can be unilateral or bilateral. Ocular symptoms include redness, blurred vision, floaters, pain, irritation, photophobia, and diplopia. Acute anterior uveitis and retinitis are the most common ocular findings in Chikungunya. The anterior uveitis is nongranulomatous or granulomatous and can be associated with increased intraocular pressure. Posterior synechiae are not common [67–69]. The clinical course is typically benign.
Chikungunya retinitis presents in the form of areas of retinal whitening in the posterior pole with surrounding retinal and macular edema and associated mild vitritis (Fig. 15.3) [67]. FA usually shows early hypofluorescence and late hyperfluorescence of retinal lesions, along with focal areas of retinal vascular leakage and capillary non-perfusion [70]. OCT reveals increased reflectivity in the nerve fiber layer zone with after shadowing corresponding to the areas of retinitis. It also helps in the detection and evaluation of associated retinal edema and exudative retinal detachment. Retinitis resolves gradually over a period of several weeks.
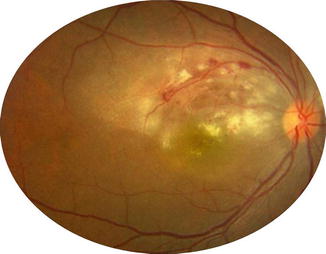
Fig. 15.3
Color fundus photograph of the right eye of a patient with Chikungunya shows confluent areas of retinitis associated with retinal hemorrhages, retinal edema, and foveal hard exudates (Courtesy, Padmamalini Mahendradas)
Other ophthalmic manifestations of Chikungunya have been reported including conjunctivitis, episcleritis, keratitis, panuveitis, multifocal choroiditis, optic neuritis, neuroretinitis, central retinal artery occlusion, panophthalmitis, lagophthalmos, and sixth nerve palsy [67, 68, 71].
Chikungunya-associated ocular disease is usually self-limiting, with most patients recovering good vision. However, permanent visual loss may occur mainly due to optic neuropathy.
Chikungunya virus has been recently detected in the human cornea. It has been suggested that cornea donation may be a route for the disease transmission, especially in endemic areas [72].
15.4.3 Laboratory Diagnosis
Chikungunya infection is suspected on the basis of clinical and epidemiological findings. However, confirmation of the diagnosis is important. In the acute phase of illness, it is based on the detection of viral nucleic acid in serum samples by RT-PCR, isolation of the virus, or detection of an antibody response. After resolution of the acute disease, the diagnosis is confirmed by the presence of an immune response. RT-PCR can detect viral nucleic acid from one day before the onset of symptoms, up to day 7 after the beginning of the disease. Antigen capture ELISA may detect viral antigens as early as day 2 after onset. Indirect immunofluorescence and ELISA are rapid and sensitive techniques for the screening of IgM or IgG immune reaction. IgM antibody and IgG antibody responses have been described to begin both by day 2 after the onset [66].
15.4.4 Management
Nonsteroidal anti-inflammatory drugs are currently recommended for Chikungunya-induced arthralgia. Ribavirin and interferon-α may inhibit viral replication [73, 74], but further studies are needed to assess their efficacy in humans. Another potential treatment for Chikungunya is chloroquine, but results of different studies have been inconclusive [75, 76].
Efforts are to be made to prevent transmission of the virus and to develop efficient and safe vaccines [62].
Topical steroids and cycloplegic agents are used for anterior uveitis. Associated ocular hypertension is managed with topical beta-blockers and oral or topical carbonic anhydrase inhibitors. Systemic steroids may be used to control the inflammation in posterior uveitis, panuveitis, and optic neuritis [67]. The use of acyclovir in association with corticosteroids has been described in some cases of Chikungunya retinitis [67], but its efficacy remains doubtful.
15.5 Rift Valley Fever
15.5.1 Introduction
Rift Valley fever (RVF) is an emerging arthropod-borne zoonotic disease caused by RVF virus, which belongs to the Bunyaviridae family. It is transmitted to humans through the bite of infected mosquitoes or through direct contact with blood, body fluids, or tissues of infected animals. RVF virus was first isolated in Kenya in 1930. It has been responsible of outbreaks in sub-Saharan African countries and in the Arabian Peninsula. Virus replication in the cattle gives high rates of mortality and abortion. RVF virus infection in humans usually causes a self-limiting, acute, and febrile illness, but severe potentially lethal forms may develop [77]. Macular or paramacular retinitis is the most common ocular complication, often resulting in permanent visual impairment.
15.5.2 Clinical Symptoms and Signs
15.5.2.1 Systemic Disease
After an incubation period of 3–6 days, RVF virus is often responsible for influenza like symptoms including fever, headache, arthralgias, myalgias, and gastrointestinal disturbances. The temperature curve usually shows a biphasic pattern, with an initial elevation lasting 2–3 days, followed by a remission and then a second febrile episode. Convalescence is typically rapid. Major life-threatening complications such as hepatic syndromes, hemorrhagic manifestations, or meningoencephalitis may rarely occur [78].
15.5.2.2 Ocular Disease
Ocular involvement has been reported to occur in 1–20 % of RVF infections [1–3, 79], usually 4–15 days after the onset of RVF. Prevalent symptoms at presentation include blurred vision, floaters, and scotomas. Unilateral or bilateral retinitis is the most common finding. It typically presents in the form of a large, single area of necrotizing retinitis, macular, or paramacular in location (Fig. 15.4a). Retinal lesions show early hypofluorescence and late staining on FA. Associated posterior segment changes include severe retinal vasculitis, retinal hemorrhages, vitritis, and optic disk edema [1–3, 79, 80]. Nongranulomatous anterior uveitis has also been described in association with posterior uveitis in patients with RVF. Anterior chamber inflammation disappears spontaneously within 2–3 weeks from the onset of systemic symptoms and is unlikely to result in complications such as glaucoma, posterior synechiae, or cataract. Retinitis usually recovers within 10–12 weeks. Permanent visual loss is common, mainly due to macular or paramacular scarring (Fig. 15.4b), retinal vascular occlusion, or optic atrophy [1–3, 79].
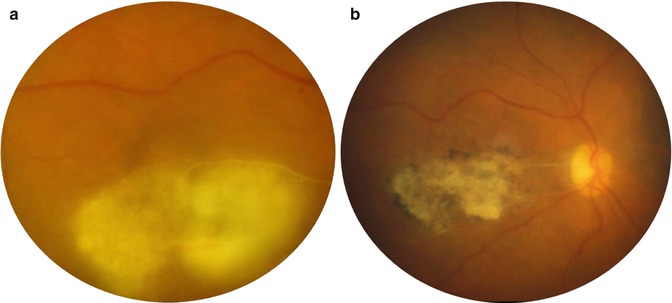
Fig. 15.4
(a) Color fundus photograph of the right eye of a patient with Rift Valley fever shows a large area of macular necrotizing retinitis associated with retinal vascular sheathing. (b) Color fundus photograph of the same eye after healing of the active retinitis shows a large atrophic retinochoroidal scar resulting in permanent severe visual loss (Courtesy, Emad Abboud)
15.5.3 Laboratory Diagnosis
Once an outbreak is recognized and early cases are diagnosed, it becomes easier to suspect further cases of RVF. The most popular method of laboratory diagnosis is based on serologic testing to detect anti-RVF virus IgM antibodies or a rising titer of IgG antibodies in the serum by ELISA technique. Furthermore, laboratory detection of RVF virus antigen by antigen capture ELISA or viral RNA by RT-PCR in serum or other tissue samples confirms the diagnosis of RVF [81].
15.5.4 Management
The current treatment of RVF is only supportive with intravenous fluids and, when indicated, blood transfusion, hemodialysis, or mechanical ventilation. There is no antiviral therapy with proven efficacy in this setting [78]. Preventive measures are recommended including mosquito control and protection against mosquito bites. Vaccination of livestock may be a key element in breaking the chain of human epidemics and could lead to control of this significant public health threat [78, 82].
15.6 Rickettsioses
15.6.1 Introduction
Rickettsioses are worldwide distributed zoonoses due to obligate intracellular small gram-negative bacteria. Most of them are transmitted to humans by the bite of contaminated arthropods, such as ticks. Rickettsial agents are classified into three major categories: the spotted fever group, the typhus group, and the scrub typhus [83, 84]. A rickettsial disease should be suspected, during spring or summer in the presence of the triad of high fever, headache and general malaise, and skin rash in a patient living in or traveling back from a region endemic for rickettsioses. Ocular involvement is common, with retinitis and retinal vascular changes being the most common features [84].
15.6.2 Clinical Symptoms and Signs
15.6.2.1 Systemic Disease
The incubation period for rickettsial disease varies between 2 and 21 days. The initial presentation typically includes high fever with abrupt onset, headache, and myalgia. A maculopapular skin rash usually appears 3–5 days after the onset of fever. The skin rash, involving also the palms of the hands and the soles of the feet, is a hallmark of rickettsial infection. However, its absence should not rule out a possible rickettsial infection, especially during the first week of illness. A local skin lesion, termed tache noire (black spot), at the inoculating site may be seen in several rickettsial infections, including Mediterranean spotted fever, caused by rickettsia conorii infection. Severe systemic complications may occur including interstitial pneumonitis, meningoencephalitic syndrome, acute renal failure, and disseminated intravascular coagulation [83, 84].
15.6.2.2 Ocular Disease
Ocular involvement is common in patients with rickettsiosis, but since it is frequently asymptomatic and self-limited, it may be easily overlooked [1–3, 84–86]. However, patients may present with ocular symptoms such as decreased vision, scotomas, floaters, or redness.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


