Purpose
To evaluate the impact of different scan patterns and scan densities on small full-thickness macular hole (MH) detection.
Design
Retrospective cross-sectional analysis.
Methods
Analysis was performed on 25 eyes from 24 patients with full-thickness MHs imaged with the Heidelberg Spectralis HRA+OCT. Included eyes underwent concurrent imaging with a standard (61-line) raster volume and a 24-line radial pattern. A 6-line radial scan pattern was extrapolated from the higher-density radial pattern. Comparisons of the missed hole rate as well as the proportion of individual B-scans demonstrating a full-thickness defect (termed “full-thickness detection index”) were carried out for the 3 scan patterns. Additionally, qualitative and quantitative hole parameters were evaluated to identify factors associated with “missed” holes.
Results
Full-thickness defects were missed at substantially higher rates using both standard raster volume (20.0%, 90% confidence interval [CI] 8.2%–37.5%) and 6-line radial scanning (12.0%, 90% CI 3.7%–30.4%) when compared to 24-line radial scanning (0% for both comparisons). Full-thickness detection indices were significantly higher for both radial scan patterns when compared to raster scanning ( P < .001 for both comparisons). Missed holes were smaller and commonly associated with prehole flaps.
Conclusion
High-density radial scanning demonstrated superior detection rates of small full-thickness MHs compared to standard raster volume scanning. This finding may be attributable to the greater foveolar scan density attained with radial scan patterns. Failure to utilize radial scanning in the setting of suspected macular holes may lead to a delay in surgical treatment, with attendant worse anatomic and visual outcomes.
With modern vitreoretinal techniques, including internal limiting membrane peeling, reported anatomic closure rates for full-thickness macular holes (MH) are routinely greater than 95%. Regression analyses have identified several factors associated with higher closure rates and better visual outcomes, including lower hole stage, smaller hole diameter, and shorter duration of symptoms. As natural history studies of stage 2 holes have demonstrated high rates of hole enlargement with progression to stage 3-4 without treatment, earlier surgical repair would potentially result in better anatomic and visual outcomes.
Maximizing diagnostic sensitivity thus becomes important as it allows for the detection of smaller/earlier macular holes. Currently, optical coherence tomography (OCT) provides detailed in vivo visualization of foveal integrity and the vitreoretinal interface far superior to that achievable with slit-lamp biomicroscopy, particularly for smaller holes. In theory, OCT-assisted diagnosis of macular holes may thus provide for more timely diagnosis and treatment of smaller/earlier full-thickness MHs with attendant better postoperative outcomes.
Diagnostic sensitivity for macular hole detection may be further improved via the design of OCT scanning protocols with B-scan pattern and density optimized for the detection of foveal pathology. Recent work has focused on the impact of OCT scan density on the detection of qualitative features of neovascular age-related macular degeneration (AMD) as well as on the accuracy of retinal thickness measurements in diabetic macular edema (DME). While these studies did demonstrate numerically inferior results with lower scan densities, the authors were careful to highlight that the sensitivity/accuracy of OCT assessments was clinically acceptable at B-scan densities one-quarter to one-eighth as high as those provided by the standard 128 B-scan/6 mm macular cube (Cirrus HD-OCT, Carl Zeiss Meditec; 3D OCT-1000, Topcon). This would seem to indicate a lesser importance for OCT scan density in optimizing scan protocols for neovascular AMD and DME.
Unlike neovascular AMD and DME, however, the pathologic features in idiopathic macular holes are by definition located at the foveal center. As such, the typical raster-based macular volume scan protocols—designed for evaluation of the more widespread macular pathology seen in neovascular AMD and DME—may be poorly suited for sensitive detection of small full-thickness MHs. Moreover, clinically important characteristics of idiopathic macular holes, such as the presence of a small inner retinal opening, are typically focal and often exceedingly small. B-scan density may thus have a greater impact on the sensitivity of full-thickness MH detection as compared to detection of more macroscopic features (eg, subretinal fluid, pigment epithelial detachments) associated with neovascular AMD.
In this report, we use a retrospective cross-sectional design to examine the effect of different OCT scan patterns (raster vs radial) and scan densities on the detection of full-thickness defects in a cohort of small full-thickness MHs.
Materials and Methods
This was a retrospective, cross-sectional analysis in which clinical data and OCT images were reviewed for patients diagnosed with a macular hole based on receipt of International Classification of Diseases (9th revision) code 362.54 as identified by billing records. This study was prospectively approved by the Duke University Institutional Review Board and adhered to the tenets set forth in the Declaration of Helsinki.
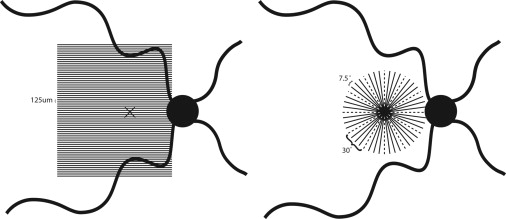
Beginning in March 2012, the Duke University Eye Imaging Center adopted a policy in which patients with suspected small macular holes underwent evaluation with concurrent 24-line radial scanning (24 B-scans with 7.5 degrees interscan spacing) in addition to the Duke Eye Center Imaging Unit standard raster volume scan (61 B-scans with 125 μm interscan spacing) using the Heidelberg Spectralis OCT unit (Heidelberg Engineering, Heidelberg, Germany) ( Figure 1 ). This allowed for the performance of a retrospective cross-sectional analysis comparing the relative rates of full-thickness MH (FTMH) detection using different scan patterns (radial vs raster) and scan densities (24-line radial vs 6-line radial). Of note, the 6-line radial scan pattern was not acquired independently, but rather was extrapolated from the 24-line radial scan based on the standard location of the 6 B-scans comprising this pattern. Ophthalmic photographers were instructed to manually center both scan patterns on the foveola if eccentric fixation was detected during OCT acquisition.
In order to be included in the analysis, patients had to have undergone concurrent raster volume and 24-line radial scanning between March 1, 2012, and October 31, 2012, and have evidence of a full-thickness MH on ≥1 B-scan on either scan pattern. Exclusion criteria included prior vitreoretinal surgery, pathologic myopia, and a history of neovascular AMD, proliferative diabetic retinopathy, solar retinopathy, or significant ocular trauma. The primary outcome was missed hole rate, which is calculated as follows (for comparison of scan pattern A to scan pattern B):
Missed hole rat e A vs B = n without FTMH on scan pattern A n with FTMH on scan pattern A or B × 100
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


