Ectopia Lentis
Rupal H. Trivedi
M. Edward Wilson
Ectopia lentis (EL) refers to the displacement of the lens away from its position in the center of the visual axis (Figs. 37.1, 37.2, 37.3). When the lens is displaced but remains attached to the ciliary processes by some portion of the zonule, it is referred to as being subluxated (Figs. 37.1, 37.2, 37.3). The term subluxated implies a partial or incomplete dislocation and is the preferred term rather than “subluxed.” The term “dislocation” is reserved for situations where there is complete disruption of all zonular attachments and free movement of the lens in the eye. In some patients, the zonule loosens in all quadrants equally, producing high myopia and phacodonesis without the edge of the lens coming into view. This phenomenon is usually also included in the concept of subluxation.
Even without development of cataract, EL often induces large refractive errors and anisometropia. In addition, movement of the dislocated lens can cause an intermittent phakic or aphakic visual axis, leading to marked visual disturbances. Such visual disturbances in a child undergoing visual development can result in amblyopia. Close follow-up is needed when young children have significant EL so that amblyopia can be prevented with glasses correction or amblyopia therapy can be started. Many of these lenses may remain centered long enough to allow the child to develop and maintain normal vision well beyond the amblyogenic years when timing of intervention is less critical.
EL can be hereditary or acquired, and trauma is the most common cause of acquired EL. A Danish national study on nontraumatic EL reported an estimated prevalence rate of 6.4/100,000. In 69% of the cases, nosologic classification was possible; identified etiologies and associations were 68.2% Marfan syndrome (MFS), 21.2% EL et pupillae, 8% simple dominant EL, 1.1% homocystinuria, 0.7% sulfite oxidase deficiency, and 0.7% Weill-Marchesani syndrome (WMS).1
The zonular fibers connect the ciliary process to the equatorial region of the lens and suspend the lens in a centered position behind the iris and pupil. Zonular fibers (all fibers together are referred to as the zonule) are rich in fibrillin, which in turn is rich in cysteine and extensively disulfide bonded. The zonule is hence disrupted in MFS, where abnormalities of fibrillin-1 cause the clinical manifestations of the MFS as well as diseases of sulfate metabolism such as homocystinuria and sulfite oxidase deficiency.2 During aging, zonular fibers become more fragile, and concomitantly, an increased risk for ocular pathologies is observed. The difference between young and old zonules is likely due to modifications in the structure of microfibrils. Older eyes have fewer fibers than do young ones, suggesting slow turnover, and these fibers are also more brittle.3
Management of EL is challenging. In addition to the optical and visual challenges presented by subluxation of the lens, the potential associated systemic conditions are of major concern, the diagnosis of which may be lifesaving.4
NONTRAUMATIC ECTOPIA LENTIS
A. Genetic EL without systemic manifestation
Simple EL: Simple EL occurs either as a congenital disorder or as a spontaneous disorder of late onset. Both are inherited in the majority of cases as autosomal dominant conditions without associated systemic abnormalities. Recessive inheritance is rare, usually occurring in families in which consanguinity has been documented. The ocular anomaly in simple EL is usually manifested as a bilateral, symmetric, upward, and temporal displacement of the lens.5
EL et pupillae: EL et pupillae is an autosomal recessive condition that is not associated with cardiovascular or skeletal features of MFS. This purely ocular disease is characterized by combined anomalies of the lens with pupillary displacement. The condition is usually bilateral, commonly not symmetrical but with the lenses and pupils displaced in opposite directions from each other. The pupils are characteristically oval or slit shaped and ectopic, and they may dilate poorly.
There are usually remnants of the pupillary membrane and subtle signs of anterior segment dysgenesis. In EL et pupillae, the lenses can be displaced in any direction, and zonules are generally stretched but may be disrupted. Glaucoma and retinal detachment (RD) are not uncommon and can occur spontaneously or following lens extraction.
There are usually remnants of the pupillary membrane and subtle signs of anterior segment dysgenesis. In EL et pupillae, the lenses can be displaced in any direction, and zonules are generally stretched but may be disrupted. Glaucoma and retinal detachment (RD) are not uncommon and can occur spontaneously or following lens extraction.
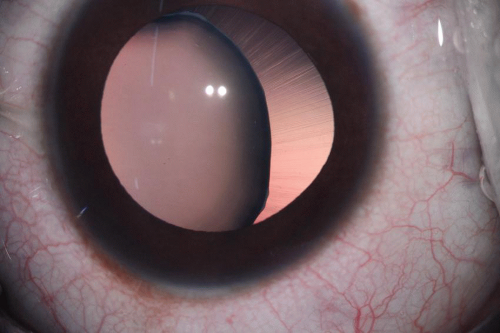 Figure 37.1. Subluxated lens. (Courtesy Dr. Abhay Vasavada, Ahmedabad, India.) |
B. Systemic disorders commonly associated with EL:
Marfan syndrome: MFS occurs in approximately 4 to 6 per 100,000 births.4 It is an autosomal dominant disorder without apparent racial or ethnic predisposition. Mutations of fibrillin gene FBN1 on chromosome 15 have been isolated, producing skeletal, cardiac, and ocular abnormalities.4 The recently revised Ghent criteria for MFS puts more weight on EL as a cardinal clinical feature. In the absence of any family history, the presence of EL and aortic root aneurysm is sufficient for unequivocal diagnosis of MFS.6 The most prominent ocular features of MFS are myopia and EL. However, since myopia is quite a common finding in the general population, the Ghent criteria have given less importance to it in the systemic score of MFS.6
 Figure 37.2. Subluxated lens in a 14-year-old child. |
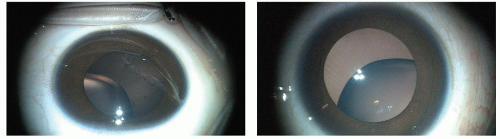 Figure 37.3. Bilateral subluxation in a 5-year-old child with MFS. |
EL occurs in 50% to 80% of patients with MFS. It is almost always bilateral and symmetrical. The amount of dislocation can be stable from early childhood, or it may worsen gradually. Dislocation of the lens in MFS is most typically upward and temporal, but deviation in any direction may occur. Increased globe length and corneal flattening are seen in MFS, but they have unclear specificity.
Weill-Marchesani syndrome: WMS is a connective tissue disorder characterized by abnormalities of the lens of the eye, proportionate short stature, brachydactyly, and joint stiffness. The ocular problems, typically recognized in childhood, include microspherophakia (small spherical lens), myopia secondary to the abnormal shape of the lens, EL, and glaucoma (due to tendency of lens to move into the pupillary space, leading to pupillary block). Although lenticular abnormalities may be absent in MFS, and homocystinuria, the presence of microspherophakia is considered a prerequisite for the diagnosis of WMS. Total dislocation into the anterior chamber is uncommon but may occur.
Homocystinuria: Affecting approximately 1 per 200,000 births, this inborn error of amino acid metabolism is more common in some ethnic groups (e.g., Ireland).6 Untreated, EL develops in 90% of affected individuals, most commonly in later childhood or early adulthood. The disorder is characterized by variable intellectual disability, EL and/or severe myopia, skeletal abnormalities, and a tendency for thromboembolic events. Overlap with MFS can be extensive and includes an asthenic (long and lean) body habitus, pectus deformity, scoliosis, mitral valve prolapse, highly arched palate, hernia, and EL. The appearance of zonular remnants may help differentiate patients with homocystinuria from those with MFS. Unlike simply elongated zonules of MFS, the lens zonules in homocystinuria are markedly abnormal and broken. Subluxation is typically inferiorly or nasally (57%), and complete dislocation into the anterior chamber or vitreous cavity can occur in up to 32% of cases in some series. The lens in homocystinuria is much more mobile than in the MFS. Typical treatment consists of a low-methionine and high-cysteine diet with supplemental pyridoxine (vitamin B6), which may prevent or delay mental retardation and lens subluxation if initiated early in life.4 Patients with homocystinuria have an increased risk of life-threatening thromboembolic events, especially with general anesthesia.
Other disorders: EL has also been described in hyperly-sinemia, sulfite oxidase deficiency, Ehlers-Danlos syndrome, Crouzon syndrome, Refsum syndrome, and scleroderma.5
TRAUMATIC ECTOPIA LENTIS
Traumatic EL can occur following blunt trauma to the head, orbit, or eye. Frequently, a high-energy projectile such as a BB gun, golf ball, or baseball is involved. Associated injuries are common and may include iris trauma, sphincter tears, angle recession, hyphema, vitreous hemorrhage, and choroidal rupture. Lens dislocation from apparently minor trauma should raise the question of possible underlying systemic disorders.
PRESENTATION, EXAMINATION AND MANAGEMENT OF ECTOPIA LENTIS
Presentation
EL may cause marked reduction in visual acuity (VA), which varies with the type and degree of dislocation and presence of other ocular abnormalities.5 The major symptom of EL is decreased VA because the progressive subluxation of the lens can cause frequent refractive changes and highly irregular astigmatism. Intermittent phakic and aphakic visual axes due to movement of the subluxated lens can also occur. Thus, the optical defocus caused by severe astigmatism and frequent aphakic condition can cause amblyopia. Monocular diplopia also can occur. Displacement of the lens into the anterior chamber can induce acute angle-closure glaucoma. Displacement into the vitreous cavity may cause lens protein-induced uveitis, vitreoretinal traction, and RD. At times, a dislocated lens can remain for years without causing any complications.
Examination
Each affected individual should have a complete ophthalmologic evaluation of both eyes and an ophthalmologic evaluation of other family members. The majority of affected persons have congenital EL as a manifestation of a systemic disease. It is therefore essential to evaluate EL patients systemically with a general physical examination, a metabolic screening, and an echocardiography as a minimum, in order to make a nosologic diagnosis and to prevent potentially life-threatening systemic complications.1 Annual ophthalmologic evaluation for the detection of EL, cataract, glaucoma, and RD is essential.
Retinoscopy and Refraction
Retinoscopy in children with EL may reveal a significant refractive error, usually myopia and astigmatism. High myopia may be caused by the higher refractive power of the periphery of the lens or increased curvature of the lens due to the absence of a portion of the zonule. High astigmatism may be due to the periphery of the lens being situated in midpupil, lens tilts, or irregularity of the lens shape because of partial loss of zonular tension. At times, an accurate refraction is difficult because of tilting or dislocation of the lens. If there are both phakic and aphakic parts of the pupil, the aphakic part is usually better for refraction because it is associated with less astigmatism. Careful and repeated phakic or aphakic refractions are necessary to achieve the best possible vision.
Slit-Lamp Examination
The diagnosis of EL usually requires a thorough evaluation with wide dilation of the pupil. However, phacodonesis is more noticeable and dramatic before dilation because dilation often stabilizes the ciliary body and iris, damping any iris or lens movement.7 The lens may be minimally subluxated, markedly subluxated and bisecting the pupil, totally dislocated into the anterior chamber,8 or free floating in the vitreous.5 When the entire zonule is disrupted, as in untreated homocystinuria, the lens becomes globular, its diameter is reduced, and high myopia develops. This is called spherophakia. Spherophakia may also be present in MFS, WMS, or EL et pupillae. The direction of lens subluxation or dislocation and the appearance of the zonular fibers can provide a clue to the systemic diagnosis. In MFS, the lens most often moves superotemporally, and stretched zonular fibers may be visible before or after pupillary dilation. In untreated homocystinuria, the
lenses become dislocated after 4 or 5 years of age; they move initially in an inferior direction behind the iris but may later occlude the pupil or dislocate into the anterior chamber. The latter is almost pathognomonic of homocystinuria. Another differentiating clinical finding is the appearance of the zonular fibers, which are nearly absent in homocystinuria (the equatorial area of the lens has only a fuzz of zonular remnants), as opposed to the elongated and sometimes rarefied zonule of patients with MFS.
lenses become dislocated after 4 or 5 years of age; they move initially in an inferior direction behind the iris but may later occlude the pupil or dislocate into the anterior chamber. The latter is almost pathognomonic of homocystinuria. Another differentiating clinical finding is the appearance of the zonular fibers, which are nearly absent in homocystinuria (the equatorial area of the lens has only a fuzz of zonular remnants), as opposed to the elongated and sometimes rarefied zonule of patients with MFS.
When a patient is evaluated for the presence of lens subluxation to rule out MFS, he or she is asked to look down while positioned at the slit lamp. Using retroillumination, the examiner looks for evidence of posterior and superior displacement of the lens by observing the inferior portion of the lens behind the iris. If the lens is in its physiologic position, there is no separation between the pupillary margin and the lens, and the equator of the lens is not visible. If the equatorial region is seen, the lens is considered subluxated. The mere visualization of the zonule on downgaze is not sufficient to diagnose lens subluxation (can be seen in high myopia).
A proposed grading scheme for subluxation of the lens (assuming that the pupil dilates to at least 7 mm) is2 as follows:
Minimal subluxation (the equator of the lens is seen only in downgaze)
Mild subluxation (the equatorial edge of the lens is visible in primary gaze but only through a dilated pupil)
Moderate subluxation (the equatorial portion of the lens is visible through the undilated pupil)
Dislocation (the lens has lost all zonular attachments and moves freely behind or in front of the iris)
Axial Length Measurements
The first histopathologic report on the eyes of a patient with the MFS demonstrated extreme size of the globe.5 Further pathologic and clinical reports have confirmed this observation. The mean AL measurement for MFS patients without dislocation was 23.39 mm and for those with dislocation, 25.96 mm. The mean AL in patients 12 years and older with an RD was 28.47 mm versus a mean of 24.90 mm for 40 eyes of patients 15 years and older with the MFS but without an RD.9
Keratometry and Pachymetry
MFS is known to be associated with a flattened cornea. These data, known for many years, are included in the Berlin criteria and in the revised diagnostic criteria for MFS as a minor sign. Flat keratometry values may reflect part of the emmetropization process—to compensate for increasing AL, the keratometry value may decrease. Sultan et al. investigated corneal thickness, curvature, and morphology in patients with MFS in a prospective, comparative case series.10 A significant decrease of the mean keratometry measurement appeared in the MFS group compared with the control group. Pachymetry in the MFS groups was also significantly decreased compared with the control group. Heur et al. also noted that Marfan patients had significantly lower keratometry and central corneal thickness value than did controls. A highly significant difference in keratometry values between Marfan and control patients was observed, and values <42 D could be used as a clinical diagnostic criterion for MFS.11



