Purpose
To determine the relationship between a ciliochoroidal detachment and intraocular pressure (IOP) after microincision vitrectomy surgery (MIVS).
Design
Prospective, consecutive, observational case series.
Methods
Thirty eyes of 30 patients with an epiretinal membrane that underwent MIVS were prospectively studied. The intraocular pressure (IOP) was measured before 3-port MIVS, and at 1 minute, 1 and 3 hours, and at 1 day postoperatively. All of the 90 sclerotomies were examined by swept source optical coherence tomography to assess the wound and presence of a ciliochoroidal detachment at 3 hours and at 1 day postoperatively. The mean IOP and closure rate of the sclerotomies were compared between eyes with and without a ciliochoroidal detachment. The correlation between the presence of ciliochoroidal detachment and postoperative IOP was determined.
Results
The incidence of ciliochoroidal detachment was 63.3% (19 eyes) during the 1-day observation period. The mean postoperative IOPs were significantly lower than the preoperative IOPs in eyes with a ciliochoroidal detachment ( P < .05). The mean postoperative IOPs were significantly higher in eyes without a ciliochoroidal detachment than in eyes with a ciliochoroidal detachment ( P < .05). The incidence of open sclerotomies was significantly higher in eyes with a ciliochoroidal detachment than in eyes without a ciliochoroidal detachment at 3 hours postoperatively ( P = .03).
Conclusions
A shallow ciliochoroidal detachment develops in 63.3% of eyes after MIVS. Hypotony at the early postoperative period may be a risk factor for a ciliochoroidal detachment.
A ciliochoroidal detachment can develop after pars plana vitrectomy (PPV), and the ciliary body can be easily detached from the sclera. This occurs because the attachment between the longitudinal ciliary muscles and the sclera from the scleral spur to the epichoroidal stars that attach the muscle to the inner surface of the sclera in the pars plana is weak. The mechanism of how PPV leads to a ciliochoroidal detachment has not been completely determined. Hypotony, trauma with subsequent inflammation, vortex vein obstruction, and accidental injection of fluid into the suprachoroidal space have been proposed to be the cause of ciliochoroidal detachment.
Microincision vitrectomy surgery (MIVS) has become more commonly used because there is less postoperative inflammation than that after conventional 20-gauge PPV. However, the incidence of ciliochoroidal detachment may be higher in eyes after MIVS because of the higher risk of postoperative hypotony after MIVS. We have reported that the incidence of ciliochoroidal detachment after MIVS was 45.8%, although none of these eyes was hypotonic.
We hypothesized that a transient hypotony immediately after MIVS is the cause of the ciliochoroidal detachment. To test this hypothesis, we used swept source optical coherence tomography (OCT) to determine whether a ciliochoroidal detachment was present, and then evaluated the relationship between the early postoperative intraocular pressure (IOP) and the presence of a ciliochoroidal detachment.
Methods
We prospectively studied 30 eyes of 30 consecutive patients with an epiretinal membrane (ERM) treated with 25-gauge transconjunctival sutureless vitrectomy at the Yokohama City University Medical Center between August 8, 2010 and December 27, 2010. Patients with glaucoma or those who had undergone PPV were excluded.
Surgical Procedure
All of the patients underwent MIVS using a 25-gauge EDGEPLUS Trocar/Cannula System (Alcon Laboratories Inc, Fort Worth, Texas, USA). For the sclerotomy, the conjunctiva was displaced away from the intended sclerotomy site, and a trocar was inserted into the vitreous at a 30-degree angle to the scleral surface 3.5 to 4.0 mm posterior to the limbus. Three sclerotomies were made in each of the 30 eyes, and all of the surgeries were performed by the same surgeon. At the end of the surgery, the cannulas were removed, and moderate pressure was applied onto the sclerotomy sites with a cotton-tip applicator. After the removal of the infusion cannula, a balanced salt solution was injected into the anterior chamber if the eye was hypotonic. The scleral wounds were inspected for any sign of leakage (ie, a formation of a conjunctival bleb or hypotony confirmed by tactile examination), indicating the need for sutures.
The IOP was measured before surgery and at 1 minute, at 1 and 3 hours, and at 1 day postoperatively with an iCare (iCare Finland Oy, Espoo, Finland) tonometer. Hypotony was defined as an IOP less than 6 mm Hg. The biomicroscopic and funduscopic findings and complications were recorded.
Optical Coherence Tomography
The sclerotomy sites were examined with a swept source OCT (SS-1000 CASIA; Tomey Corporation, Nagoya, Japan) at 3 hours and at 1 day postoperatively. The patients were asked to move their eyes so that the light from the OCT entered the sclerotomy site perpendicularly. A standardized 3-dimensional (3-D) scan by the swept source OCT was used on all 90 sclerotomy sites. The standardized 3-D scan acquires 256 B-scan images with each image containing 512 A-scans across an area of 6 × 6 mm. We used the enhanced depth imaging method to obtain clearer images of the internal lip of the sclerotomies. The OCT instrument was pushed close enough to the eye to create an inverted image, and the inverted image was automatically reinverted to the normal orientation after the measurements.
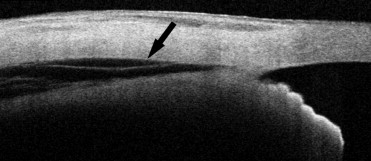
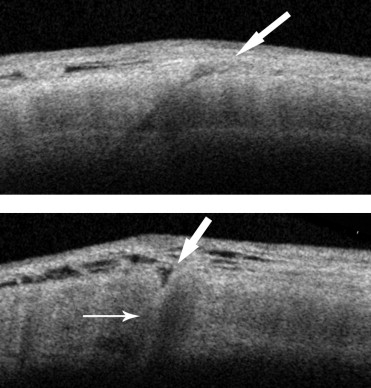
The swept source OCT images were analyzed for the presence of a ciliochoroidal detachment and for wound closure. A ciliochoroidal detachment was considered to be present by the presence of supraciliary effusions ( Figure 1 ) . A wound was considered to be open if a full-thickness scleral gap was detected at the sclerotomy site. A partial wound closure was defined as the presence of a partial, either externally or internally, scleral gap at the sclerotomy site ( Figure 2 ) . All of the sclerotomies were evaluated on the 3-D images by 2 investigators (M.I., A.A.) in a masked manner. When there was a disagreement, a third investigator (S.Y.) was consulted for the final decision.
Statistical Analyses
Statistical analyses were performed using PASW Statistics (version 17.0; SPSS, Inc, Chicago, Illinois, USA). The patients were divided into 2 groups by the presence or absence of a ciliochoroidal detachment at 3 hours and/or 1 day postoperatively. The closure rate of the sclerotomies and the incidence of conjunctival blebs were compared between the 2 groups using the Fisher exact test. The mean IOPs for the 2 groups were compared using the Mann-Whitney U test. The mean preoperative and postoperative IOPs were compared using the Wilcoxon signed rank test. A P value <.05 was taken to be significant.
Results
Thirty eyes of 30 consecutive patients who underwent MIVS for ERM were studied. There were 13 men and 17 women whose mean age ± standard deviation was 66.1 ± 7.9 years, with a range of 52 to 78 years. Surgery was successfully completed with removal of the ERM in all the eyes using the 25-gauge vitrectomy system. Wound suture and fluid-air exchange was not performed on any of the eyes. No intraoperative complications were encountered in any of the eyes.
No significant differences were found in the demographics of the patients between the 2 groups ( Table 1 ).
| Ciliochoroidal Detachment + | Ciliochoroidal Detachment − | P Value | |
|---|---|---|---|
| Number of eyes (patients) | 19 (19) | 11 (11) | |
| Age (mean ± SD, y) | 63.8 ± 7.9 | 68.9 ± 7.1 | .161 a |
| Sex (male/female) | 7/12 | 5/6 | .712 b |
| Operative time (minutes) | 27.8 ± 7.2 | 28.8 ± 14.9 | .281 a |
| Scleral thickness (μm) | 572 ± 31 | 570 ± 26 | .983 a |
Optical Coherence Tomography Image of Sclerotomies
The sclerotomy sites were clearly observed as gaps in the sclera in the swept source OCT images. A shallow peripheral ciliochoroidal detachment was observed in the swept source OCT images in 17 of the 30 eyes (56.7%) at 3 hours and in 18 eyes (60.0%) at 1 day postoperatively. The ciliochoroidal detachment resolved between 3 hours and 1 day postoperatively in 1 eye. On the other hand, 2 cases of ciliochoroidal detachment were detected at 1 day but not at 3 hours postoperatively. Thus, the overall incidence of ciliochoroidal detachment in the 30 eyes was 63.3% (19 eyes) after the MIVS. The closure rate of the sclerotomies was 33.3% (30/90 eyes) at 3 hours and 46.7% (42/90 eyes) at 1 day postoperatively. No significant difference in the wound status was found between the 2 groups at 3 hours ( Table 2 ) and at 1 day postoperatively.
| Ciliochoroidal Detachment + | Ciliochoroidal Detachment − | P Value | |
|---|---|---|---|
| Number of sclerotomies (%) | |||
| Closed | 18 (32) | 13 (39) | |
| Partial closure | 25 (44) | 18 (55) | .09 a |
| Open | 14 (25) | 2 (6) | |
| Total | 57 (100) | 33 (100) | |
| Number of eyes (%) | |||
| Open sclerotomies | 12 (63) | 2 (18) | .03 b |
| Conjunctival bleb | 14 (74) | 2 (18) | .01 b |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


