Ear Trauma
External ear trauma occurs frequently in children because of the ear’s prominent and unprotected position as well as the reflex tendency of head turning to avoid direct facial injury. Blunt trauma may occur during contact sports, most frequently wrestling, or during falls.
5-1 Incisional Evacuation of Hematoma
Introduction
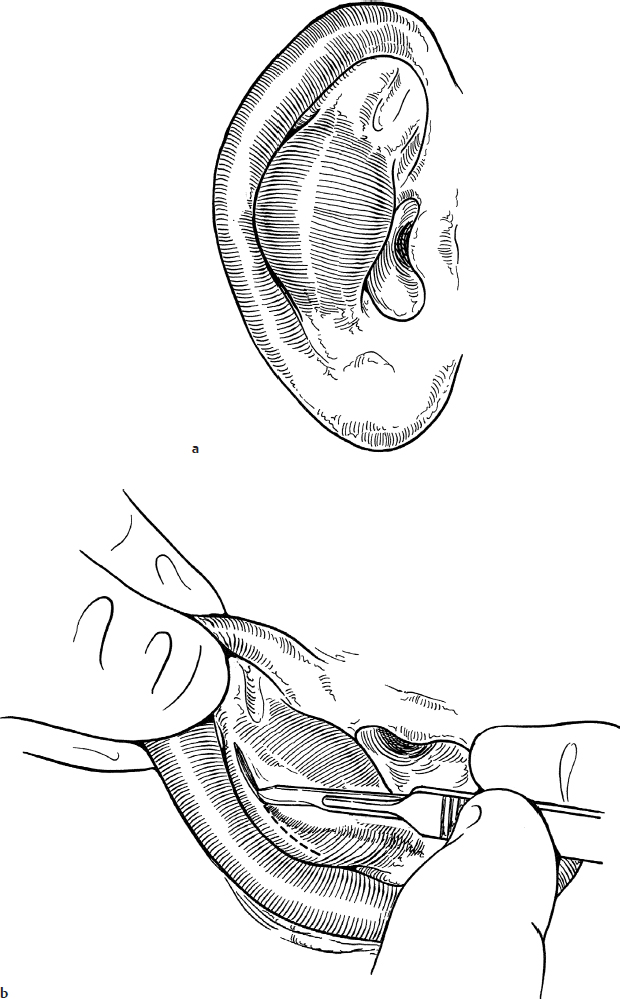
Blunt or shearing trauma may lead to separation of the perichondrium, which, on the lateral surface of the auricle, is tightly adherent to the skin. A hematoma may then form between the two layers. This collection typically forms in either the conchal bowl or the scaphoid fossa (Fig. 5.1a). The consequent devascularization of the underlying cartilage may lead to permanent ear deformity.
Indications
Evacuation of seroma or hematoma is indicated to avoid permanent auricular deformity.
Preoperative Evaluation
Preoperative evaluation consists of noting the presence of a seroma or hematoma. Associated injuries to the inner and middle ear and the rest of the head must be ruled out.
Operative Technique
1. This procedure can often be performed under local anesthesia in older children but may require a general anesthetic in young, uncooperative children.
2. The ear is thoroughly cleansed with an iodine-containing solution. A small amount of local anesthetic can then be instilled at the site of the planned incision.
3. An incision is made along the lateral margin of the hematoma in parallel with the natural curve of either the helical or antihelilcal folds (Fig. 5.1b).
4. The perichondrium and skin are gently separated from the cartilage, and the hematoma is thoroughly evacuated with a suction device (Fig. 5.1c). Gentle curettage with a small sharp mastoid curette can be performed to remove any fibrogranulomatous material that may have formed. The pocket is gently irrigated with sterile saline using an 18-gauge angiocatheter.
5. The incision can then be loosely reapproximated with interrupted 5-0 or 6-0 fast absorbing chromic sutures that do not need to be removed (Fig. 5.1d). Leaving the incision partly open allows a pathway for drainage of any additional fluid.
6. The perichondrial flap is held in position with 4-0 nylon sutures that are tied over dental rolls or petroleum gauze dressings that are precisely contoured to apply pressure, which immobilizes the flap and eliminates all dead space (Fig. 5.1e). This bolster can be removed in 7 to 10 days.
7. Antistaphylococcal antibiotics are prescribed for 10 days to prevent chondritis.
Complications
1. Reaccumulation of hematoma/seroma
2. Chondritis
3. Perichondritis
4. Scar formation, cauliflower ear