Purpose
To investigate the dynamic changes of tear fluid after cosmetic transcutaneous lower blepharoplasty.
Design
Prospective, observational case series study.
Methods
A total of 60 eyes of 30 patients with transcutaneous lower blepharoplasty were involved in the study. All subjects completed the Ocular Surface Disease Index questionnaire and underwent tear film break-up time measurements and the Schirmer test before surgery and 1 week, 1 month, and 3 months after surgery. Tear meniscus parameters measured by optical coherence tomography were recorded. Lower lid margin reflex distance was also measured. At each time point after surgery, these parameters were compared with the baseline parameters. The incidence of dry eye and chemosis after surgery was assessed.
Results
The Ocular Surface Disease Index score increased significantly 1 week after surgery ( P < .01). The Schirmer test values were significantly decreased 1 week postoperatively ( P < .01), and they returned to baseline by 3 months. There was no significant change in tear film break-up time before and after surgery. The tear meniscus height, depth, and cross section area values were significantly increased at 1 week postoperatively, decreased at 1 month ( P < .01), and returned to baseline at 3 months ( P > .05). The cornea–lower eyelid angle significantly decreased at 1 week postoperatively ( P < .01), increased at 1 month ( P < .01), and returned to baseline by 3 months ( P > .05). The lower lid margin reflex distance was increased 1 week after surgery ( P < .01), and gradually recovered but had not returned to the baseline 3 months after surgery ( P < .01). The increased tear meniscus height had a positive correlation with lower lid margin reflex distance. The incidence of dry eye and chemosis at 1 week postoperatively was 16.7% and 15%, respectively.
Conclusions
Cosmetic transcutaneous lower blepharoplasty affects ocular surface and tear fluid, which leads to dryness, tearful eyes, and chemosis. However, this influence is temporary after surgery, and the symptoms resolve within 3 months. A positive correlation between tear meniscus height and lower lid margin reflex distance was observed. Assessment of the tear meniscus with optical coherence tomography provided a quick, noninvasive, and quantitative method to investigate the dynamic changes of the tear fluid after blepharoplasty.
Cosmetic lower blepharoplasty is one of the most commonly requested and performed aesthetic procedures, especially transcutaneous lower blepharoplasty. A temporary increase in irritative symptoms is seen in most patients undergoing transcutaneous lower blepharoplasty. Uncomfortable feelings including dryness, tearful eyes, and chemosis are common postoperative complaints in these patients, even with successful surgery. The surgery may affect the ocular surface and tear fluid. However, there are limited quantitative indicators to analyze the changes of tear fluid and ocular surface. An understanding of the symptoms through objective examination indices may improve the satisfaction of patients. Although Schirmer test, tear film break-up time (BUT) test, medical photographs, slit-lamp microscopy examinations, ocular surface thermography, and corneal sensitivity measurement have been used in blepharoplasty, these still cannot explain why tearful eyes develop in patients in the early stages after surgery.
Optical coherence tomography (OCT) has been reported to be potentially of high value for the examination and assessment of tear meniscus, especially in the diagnosis of dry eye disease, because it is a rapid, high-resolution tool with the ability to noninvasively provide detailed information about the ocular surface. The tear meniscus measured by OCT has been applied in investigating the changes in the lower tear meniscus pattern in primary acquired nasolacrimal duct obstruction and functional nasolacrimal duct obstruction, as well as in estimating the symptoms of ocular dryness and discomfort in both normal and artificial eyes.
In this study, the tear meniscus measured by OCT was used in association with Schirmer, BUT, and Ocular Surface Disease Index questionnaire to assess the effect of transcutaneous lower blepharoplasty on the ocular surface and tear fluid. The lower lid malposition is the most commonly reported complication after transcutaneous lower eyelid blepharoplasty. So, lower eyelid position was also measured to evaluate its effect on tear fluid.
Methods
This prospective study was approved by the Ethics Committee of Shanghai Ninth People’s Hospital. It was in compliance with the tenets of the Declaration of Helsinki for clinical research. Written informed consent was obtained from all participants after explanation of the purpose and possible consequences of the study. This single-institution prospective observational study began on November 1, 2012 and lasted for 12 months.
Participants and Examinations
A total of 30 consecutive patients referred to the Department of Ophthalmology of Shanghai Ninth People’s Hospital were recruited in this prospective study. All of the cases underwent primary transcutaneous lower blepharoplasty, which was performed by 1 surgeon (H.Z.).
The exclusion criteria were as follows: the presence of ocular diseases, history of intraocular surgeries including refractive surgeries, Sjögren syndrome, Stevens-Johnson syndrome, severe thyroid eye disease, preoperative dry eye syndrome, nasolacrimal duct obstruction, relative or real proptosis, enophthalmos, scleral show, lagophthalmos, ectropion, periocular trauma causing eyelid malposition, revision blepharoplasty, concomitant upper blepharoplasty, other types of lower blepharoplasty, incomplete medical records, age >60 years, age <45 years, and failure to return for scheduled follow-up examinations for 3 months. Dry eye was diagnosed according to the dry eye diagnostic criteria, as follows: >10.4 score on the Ocular Surface Disease Index questionnaire (OSDI), high tear secretion deficiency in the Schirmer I test ≤5 mm, or BUT ≤5 seconds.
All patients were scheduled for examinations preoperatively and 1 week, 1 month, and 3 months postoperatively. At each scheduled time point, patients were asked to complete a standard OSDI questionnaire to evaluate subjective symptoms, and then the following procedures were performed: a medical digital photograph was taken and patients underwent OCT imaging, BUT testing, and Schirmer I testing. No postoperative medication was instilled into the eyes.
Tear film break-up time and Schirmer I assessments
The standard BUT measurement and Schirmer I test were performed as described by Ibrahim and associates.
Optical coherence tomography examination
Zeiss Cirrus HD-OCT (Carl Zeiss Meditec, Inc, Dublin, California, USA) was applied to perform a vertical 2-mm scan across the lower tear meniscus below the center of the cornea at the 6 o’clock position using anterior segment 5-line raster model. The line length was fixed at 3 mm, and the scan angle was 90 degrees. The images were obtained by 1 examiner (L.L.). Each participant was instructed to fixate on an external fixation target positioned in the primary gaze. The participants were instructed to blink normally to distribute the tear film evenly and to minimize ocular surface dehydration. The image was captured immediately after blinking within 4 seconds to make the examination consistent.
Tear meniscus parameter assessment
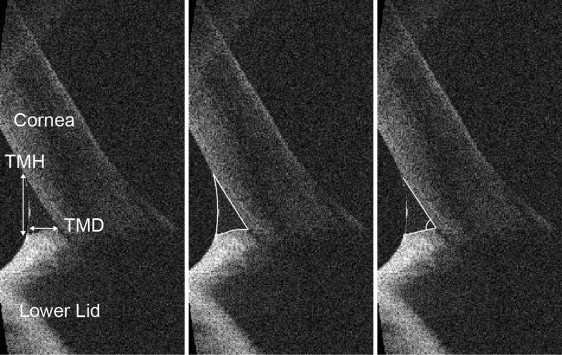
Four parameters of the lower tear meniscus were measured: tear meniscus height (TMH, μm), tear meniscus depth (TMD, μm), tear meniscus cross section area (TMA, μm 2 ), and the cornea–lower eyelid angle (degrees) (CL angle) ( Figure 1 ). Image-Pro Plus (version 6.0, Media Cybernetics, USA) was used to analyze the OCT images.
Surgical Technique
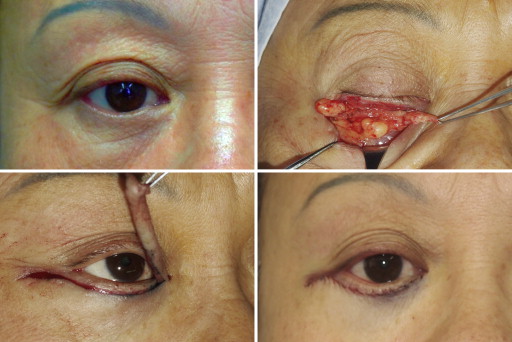
All patients underwent transcutaneous lower blepharoplasty, which was performed using a standard approach ( Figure 2 ). The incision was marked 2 mm below the lid margin in the subciliary crease. At least 3 mm pretarsal muscle was preserved. The septum was incised to expose the lateral, central, and medial fat compartments, and these fats were excised. The patient was asked to look upward and open his or her mouth. The skin-muscle flap that remained above the subciliary incision was safely removed, along with a triangle of tissue lateral to the canthus. The orbicularis muscle suspension was performed by suturing the preseptal orbicularis muscle to the inferior aspect of the periosteum of the lateral orbital rim with a single stitch of 5-0 Vicryl (Ethicon, Johnson & Johnson, Somerville, New Jersey, USA). A tension-free closure was achieved with 7-0 silk suture.
Lower Eyelid Position Measurement
Photographs of participants were taken at the scheduled time point using an Olympus E-PL1 camera (Japan) under identical lighting conditions, with the patient in a sitting position and with the eyes in primary gaze. Image Pro Plus 6.0 was used to measure the distance (pixels) from center of pupil to lower eyelid margin, which was defined as lower lid margin reflex distance (MRD 2 ). We standardized the lower lid margin reflex distance to an arbitrary horizontal corneal diameter of 11 mm by multiplying the ratio of lower lid margin reflex distance to corneal diameter in pixels by 11, as described by Taban and Perry.
Statistical Analysis
Statistical analysis was performed using SPSS software (version 19.0, SPSS Inc, Chicago, Illinois, USA). Descriptive statistics were calculated for all variables and were expressed as the mean ± standard deviation (SD). The Wilcoxon test was used to compare the preoperative and postoperative parameters. The Spearman correlation coefficient (r) was calculated to assess the relationship between tear meniscus height, Schirmer, and OSDI value. Partial correlation was assessed between tear meniscus height, cornea–lower eyelid angle, and lower lid margin reflex distance. P values less than .05 were considered statistically significant.
Results
Baseline Characteristics
In total, 30 patients met the study inclusion criteria. The population examined varied in age from 45 to 60 years, with a mean age of 50.53 ± 4.80 years; 23 patients (76.7%) were female and 7 patients (23.3%) were male. The mean preoperative parameter values are as follows: OSDI 3.82 ± 3.01, BUT 5.78 ± 2.33 seconds, Schirmer 11.63 ± 6.47 mm, tear meniscus height 292.67 ± 98.58 μm, tear meniscus depth 148.30 ± 48.85 μm, tear meniscus cross section area 21 430.00 ± 13 844.33 μm 2 , and cornea–lower eyelid angle 60.41 ± 9.76 degrees. The Table shows the patients’ preoperative and postoperative data.
| OSDI | BUT (s) | Schirmer I (mm) | TMH (μm) | TMD (μm) | TMA (μm 2 ) | CL Angle (Degrees) | MRD 2 (mm) | |
|---|---|---|---|---|---|---|---|---|
| Preop | 3.82 ± 3.01 | 5.78 ± 2.33 | 11.63 ± 6.47 | 292.67 ± 98.58 | 148.30 ± 48.85 | 21 430.00 ± 13 844.33 | 60.41 ± 9.76 | 4.57 ± 0.37 |
| Postop 1 wk | 7.51 ± 6.10 a | 5.47 ± 2.30 | 9.47 ± 6.87 a | 442.33 ± 292.18 a | 238.83 ± 119.53 a | 53 601.67 ± 57 812.64 a | 51.66 ± 9.01 a | 4.89 ± 0.40 a |
| P value | .007 | .322 | .002 | <.001 | <.001 | <.001 | <.001 | <.001 |
| Postop 1 mo | 4.78 ± 6.17 | 5.38 ± 2.14 | 10.08 ± 5.98 | 337.00 ± 114.60 a | 188.33 ± 62.20 a | 31 171.17 ± 20 366.52 a | 55.66 ± 8.77 a | 4.87 ± 0.28 a |
| P value | .75 | .158 | .069 | <.001 | <.001 | <.001 | .007 | <.001 |
| Postop 3 mo | 2.76 ± 3.16 | 5.65 ± 2.07 | 10.10 ± 5.66 | 297.83 ± 74.59 | 153.67 ± 37.95 | 22 114.5 ± 10 383.08 | 59.04 ± 7.63 | 4.72 ± 0.31 a |
| P value | .19 | .700 | .086 | .371 | .354 | .137 | .338 | <.001 |
Comparison of Ocular Surface Parameters at Each Time Point After Surgery With the Baseline Values
The mean OSDI was significantly increased at 1 week postoperatively, returned to baseline by 1 month, and decreased at 3 months, with no significance (1 week, 7.51 ± 6.10, P < .01; 1 month, 4.78 ± 6.17, P > .05; 3 months, 2.76 ± 3.16, P > .05). The mean BUT changed with no significance (1 week, 5.47 ± 2.30 seconds; 1 month, 5.38 ± 2.14 seconds; 3 months, 5.65 ± 2.07 seconds; P > .05). There was a significant decrease in Schirmer test between the preoperative and 1 week postoperative values, and those values returned to baseline at 3 months postoperatively (1 week, 9.47 ± 6.87 mm, P < .01; 1 month, 10.08 ± 5.98 mm, P > .05; 3 months, 10.10 ± 5.66 mm, P > .05) ( Figure 3 , Table ). Dry eye developed in 5 patients (10 of 60 eyes, 16.7%) at 1 week postoperatively; in 3 of them it persisted for 1 month, and in only 1 of them it persisted for 3 months.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


