Purpose
To estimate the impact of dry eye disease (DED) on work performance and productivity in office workers using visual display terminals (VDTs).
Design
Cross-sectional study.
Methods
Six hundred seventy-two Japanese young and middle-aged office workers using VDTs completed a questionnaire that was designed to measured at-work performance deficits and productivity losses using the Japanese version of the Work Limitations Questionnaire, completed by e-mail. Using the Japanese dry eye diagnostic criteria, respondents were classified into 3 groups: definite DED, probable DED, and non DED.
Results
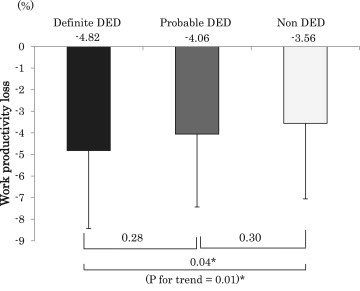
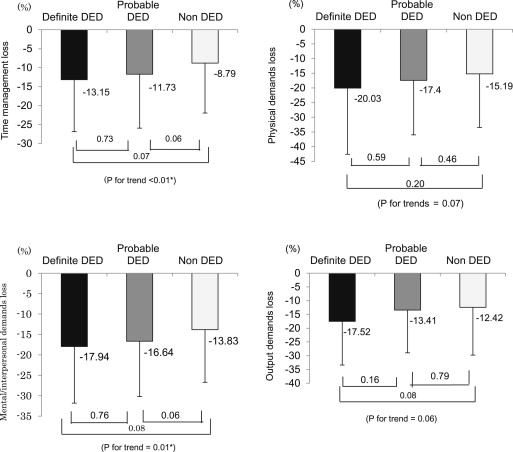
Of the 672 office workers, 553 subjects (82.3%), including 366 men and 187 women, completed the questionnaire and underwent clinical evaluation. As for the total workplace productivity loss, the non DED group demonstrated a loss of 3.56%, those with probable DED demonstrated a loss of 4.06%, and those with definite DED demonstrated a loss of 4.82%, indicating significantly worse performance and productivity ( P = .014, trend test). For the 4 subscales, DED was associated with significantly lower on-the-job time management ( P = .009, trend test) and combined mental performance and interpersonal functioning ( P = .011, trend test). After controlling for age, sex, VDT working hours, and diagnosis of DED, time management, physical demands, and mental and interpersonal functioning showed a significant relationship to DED (each P > .05). Annual DED productivity losses were estimated to be $6160 per employee when measured by total production and $1178 per employee calculated by wage.
Conclusions
This study indicated that there is a significant impact of DED on the total productivity of Japanese VDT users.
According to the International Dry Eye Work Shop, “Dry eye is a multifactorial disease of the tears and ocular surface that results in symptoms of discomfort, visual disturbance, and tear film instability with potential damage to the ocular surface.” Dry eye disease (DED) is one of the most prevalent ocular surface diseases in the world, occurring from 4.4% to as high as 50% of middle-aged and older people. In the United States, estimates from the largest studies suggest that DED affects approximately 5 million people 50 years of age and older. Many studies have demonstrated that patients with DED experience an impact on their daily lives, including poorer general health among patients with moderate to severe DED.
Prior studies also have demonstrated an impact of DED on the ability to work using questionnaires such as the Impact of Dry Eye on Everyday Life questionnaire, which includes a module on work productivity. However, to the extent that this work is based on questionnaires developed for use specifically in the dry eye setting, direct comparisons with other health conditions generally have not been performed. Whether one approach is better or worse has not, to our knowledge, been studied. Nonetheless, such work has aided the recognition that there is an economic burden from DED that can be divided into 2 categories: (1) direct costs such as medical fees and cost of medications and (2) indirect costs such as reduced employment rates, absence from work (absenteeism), and equivalent lost work days resulting from adversely affected performance (presenteeism). Moreover, there have been some studies using questionnaires, such as the Work Productivity and Activity Impairment Questionnaire, developed to assess work productivity across a range of health conditions that have reported a correlation between the severity of dry eye and the duration of both absenteeism and presenteeism, with perhaps a greater impact of DED on presenteeism.
In Japan, Yamada and associates evaluated presenteeism in patients with DED using the Japanese version of the Work Limitations Questionnaire, an established tool for evaluation of presenteeism with high internal reliability. However, that study was carried out as an online survey and did not include a clinical evaluation for DED, which could provide important additional information and may reduce misclassification.
The present study was undertaken to address some of the limitations of prior studies. We evaluated the impact of DED on presenteeism in office workers using the Japanese version of the Work Limitations Questionnaire to allow for direct comparison of the impact of DED versus other health conditions. We conducted clinical evaluation and classification of DED according to the Japanese DED diagnostic criteria to address possible misclassification that could arise from use of self-reported DED.
Methods
Selection of the Study Participants
This cross-sectional study followed the tenets of the Declaration of Helsinki, and the protocol was approved by the Institutional Review Board of Ryogoku Eye Clinic, Tokyo, Japan. All subjects gave written informed consent. Under the supervision of the Japanese Dry Eye Society, the authors arbitrarily selected 2 large companies in the pharmaceutical company listed on the Japanese stock market. We sent a letter to the industrial physician of the health management section of each company to explain the purpose of the study and to request their participation. One company responded to our letter and consented to participate in this study. After an internal review of the protocol and the risks and benefits of the study, permission was granted to conduct the study among employees who were willing to participate. Employees were invited by e-mail to answer the questionnaires and to attend a general ophthalmic check-up. A maximum of 2 e-mail reminders were sent. Subjects who reported a history of any eye surgery were excluded from the study protocol.
Diagnosis of Dry Eye Disease
The diagnosis of DED was established according to the Japanese DED diagnostic criteria. Briefly, 3 criteria were evaluated: (1) presence of dry eye symptoms, (2) presence of qualitative or quantitative disturbance of the tear film in one or both eyes (Schirmer test results ≤5 mm or tear film break-up time ≤5 seconds), and (3) presence of conjunctival and corneal epithelial damage (total staining score, ≥3 points) in one or both eyes. The presence of all 3 criteria was necessary for a definite diagnosis of DED. Subjects showing the presence of 2 of the 3 criteria were diagnosed with probable DED, whereas those with 1 or no positive criteria were diagnosed as having non DED. The methods for administration of Schirmer tests, tear film break-up time analysis, and fluorescein and lissamine staining have been documented previously. Corneal and conjunctival epithelial damage was evaluated by lissamine green and fluorescein staining, after which assessment of tear film break-up time was performed. Finally, the Schirmer test was performed for 5 minutes without topical anesthesia.
Work Limitations Questionnaire
We used the Japanese version of the Work Limitations Questionnaire (Sompo Japan Healthcare Services, Inc, Tokyo, Japan). The questionnaire consists of 25 items and is a validated self-report survey tool for assessing the impact of health problems on at-work performance and productivity. This tool uses data accumulated within a 4-week recall period and calculates scores ranging from 0 to 100 using a specific validated algorithm. A score of 0 indicates no limitations, whereas a score of 100 indicates limitations 100% of the time. In addition to a total score that evaluated overall work performance, we also calculated subscale scores to evaluate 4 domains of work limitations: time management, physical demands, mental or interpersonal functioning, and output demands. The time management scale contains 5 items that address difficulty handling time and scheduling demands. The 6-item physical demands scale covers a person’s ability to perform job tasks that involve bodily strength, movement, endurance, coordination, and flexibility. The mental and interpersonal demands scale has 9 items addressing cognitive job tasks and on-the-job social interactions. The output demands scale contains 5 items concerning diminished work quantity and quality (eg, handling the workload and finishing work on time). Each question was evaluated using a 5-point scale (none of the time to all of the time). The final scale score indicated the percent of time the patient was limited in performing the specific tasks of the job. Past or current history of certain common systemic diseases such as hypertension, diabetes mellitus, depression, and use of systemic medications was determined by asking participants whether they had ever been told that they had these conditions by their physicians or whether they used any systemic medications, including antidepressants.
In addition to work limitation scores, we calculated the economic impact of work productivity losses in 2 ways: (1) based on average annual sales loss per person and (2) based on average annual wages per person. The data on the average annual sales per person as well as the average annual wage were provided by the participating company. Values in Japanese yen were converted to United States dollars using the currency exchange rate concurrent with the August 5, 2011, completion of the Osaka study (1 yen = 0.0126 dollars).
Statistical Analysis
The analysis included all subjects who completed the Japanese version of Work Limitations Questionnaire and the dry eye clinical examination. Statistical comparisons of the total score, as well as the subscale scores, were made among the 3 DED diagnostic groups using the Dunnett test. Trend tests were performed via linear regression analysis to compare the degree of work performance loss as the outcome across the ordered groups indicating dry eye status (non DED, probable DED, definite DED). We then used multiple linear regression analysis to adjust for possible confounders (sex, age, and VDT hours). We categorized prolonged VDT working hours as more than 8 hours, because we previously showed this cut point was associated with DED. A P value of less than .05 was considered to indicate a statistically significant difference. All statistical analyses were performed using the SAS software version 9.2 (SAS, Inc, Cary, North Carolina, USA).
Results
Participants and Diagnosis of Dry Eye
Of the 672 office workers in this company, 553 (82.3%) participated in this study, including 366 men (66.2%) and 187 women (33.8%) between 22 and 65 years of age. Using the Japanese DED diagnosis criteria, 65 subjects (11.8%) were diagnosed with definite DED, 299 subjects (54.1%) were diagnosed with probable DED, and 189 subjects (34.2%) were in the non DED group. Characteristics of the study population are provided in Table 1 (detailed ophthalmic findings were presented previously). Only 4.7% and 1.1% of all the subjects had hypertension or diabetes mellitus, respectively, with no significant difference among the 3 DED groups ( P = .68 for hypertension and P = .16 for diabetes mellitus). Previous studies showed an association between depression and DED; however, only 2 subjects reported having been diagnosed with depression or to be using antidepressants in the current study.
| Definite DED (n = 65; 11.8%) | Probable DED (n = 299; 54.1%) | Non DED (n = 189; 34.2%) | Total (n = 553) | P Value | |
|---|---|---|---|---|---|
| Age (y) | 40.6 ± 7.3 | 43.5 ± 8.9 | 43.5 ± 8.9 | 43.1 ± 8.8 | .045 a ∗ |
| Male (%) | 46.2 | 63.9 | 76.7 | 66.2 | .000 b ∗ |
| Average VDT hours | 8.2 ± 2.3 | 8.0 ± 2.3 | 7.6 ± 2.1 | 7.9 ± 2.2 | .071 a |
| Hypertension, no. (%) | 2 (3.1) | 13 (4.3) | 11 (5.8) | 26 (4.7) | .678 b |
| Diabetes mellitus, no (%) | 1 (1.5) | 5 (1.7) | 0 (0.0) | 6 (1.1) | .164 b |
Work Limitations
The degree of work limitation according to DED status was 4.82% in the definite DED group and 4.06% in the probable DED group; both showed greater losses than the non DED group (3.56%). There was a significant difference between the definite DED and non DED groups ( P = .041; Figure 1 ). Using the average working hours in Japan (7.75 hours/day, 243 days/year), this difference can be converted to a loss of approximately 23.7 hours, or almost 3.1 working days in a year. The trend test across the 3 DED groups (non DED, probable DED, definite DED) also showed significant worsening from the non DED to the definite DED group ( P = .014). Trend tests across DED diagnostic groups and each subscale score revealed 2 subscales that were significantly lower in the definite DED group ( P = .009 for time management loss and P = .011 for mental and interpersonal functioning loss; Figure 2 ). Subgroup analyses comparing subjects with (n = 343) and without (n = 21) dry eye symptoms showed a significantly greater magnitude of work limitations among those with symptoms (4.33 ± 3.44 vs 2.07 ± 2.07; P = .005).
Using models that evaluated the association between DED and work productivity losses after taking in account the possible influence of other factors (age, sex, VDT hours), we observed a significant association between DED and total productivity loss ( P = .022; Table 2 ). Additional adjustment for cigarette smoking (which was not associated with productivity loss; data not shown) did not affect findings and was not included in the final models. Considering the 4 subscales, 3 of them, time management, physical demands, and mental and interpersonal functioning, showed a significant relationship with DED ( P = .021, P = .023, and P = .025, respectively). For the subscale of output demands, there was a borderline significant association with DED ( P = .068).
| Total Loss | Time Management Loss | Physical Demands Loss | Mental or Interpersonal Loss | Output Demands Loss | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Slope ± SE | P Value | Slope ± SE | P Value | Slope ± SE | P Value | Slope ± SE | P Value | Slope ± SE | P Value | |
| Dry eye | 0.57 ± 0.25 | .022 a | 2.17 ± 0.94 | .021 a | 3.03 ± 1.33 | .023 a | 2.05 ± 0.91 | 025 a | 2.04 ± 1.11 | .068 |
| Age (y) | −0.01 ± 0.02 | .491 | −0.16 ± 0.07 | .026 a | 0.37 ± 0.10 | .001 b | −0.10 ± 0.07 | 144 | −0.07 ± 0.08 | .382 |
| Gender (female) | 0.10 ± 0.34 | .768 | −0.47 ± 1.32 | .722 | −0.42 ± 1.86 | .819 | 0.68 ± 1.28 | 595 | −0.22 ± 1.56 | .889 |
| VDT working hours (>8 hours) | −0.03 ± 0.37 | .937 | 1.68 ± 1.42 | .239 | −2.74 ± 1.97 | .165 | 0.35 ± 1.38 | 799 | −0.15 ± 1.68 | .929 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


