and Mitrofanis Pavlidis2
(1)
Department of Ophthalmology, Uppsala University Hospital, Uppsala, Sweden
(2)
Augencentrum Köln, Cologne, Germany
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-319-20236-5_19) contains supplementary material, which is available to authorized users.
Electronic supplementary material
for this chapter is accessible online at http://extras.springer.com/ by searching via the ISBN.
19.1 General Introduction
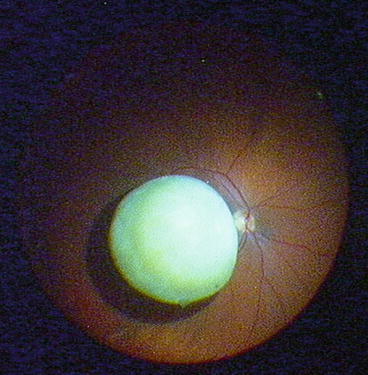
Necessity of surgery: If nuclear fragments drop, we always operate in order to prevent intraocular inflammation and hypertension. In case of dropped soft cortical fragments, it is possible to wait and not to operate if the eye remains quiet (Fig. 19.2).
Fig. 19.1
A hybrid set-up. One 27G infusion trocar and two 25G instrument trocars
Timing of surgery: The surgery is not acute. Normally a dropped nucleus occurs under drop anaesthesia. To proceed with vitrectomy under drop anaesthesia will inflict much unnecessary pain to the patient. It is therefore advisable to stop surgery when a dropped nucleus occurs and to schedule a planned surgery within 1 week. During this time, the eye can be treated against corneal oedema and ocular hypertension.
Surgical Pearls No. 75
The most patients who underwent a complicated cataract surgery do not complain about the complication but about the painful procedure. Why? The cataract surgery was started with drop anaesthesia, and when the complication occurred, the surgery was continued with the same anaesthesia. Our recommendation: If you experience a complication, decide if you continue at once or delay the surgery. If you decide to continue at once, then add a subtenonal or retrobulbar anaesthesia. You will have a happy patient.
Determine preoperatively with a maximally dilated pupil whether the anterior capsule is intact or not. If it is intact, implant a three-piece IOL in the sulcus. If the anterior capsule is defective, implant a scleral-fixated three-piece IOL (suture or Scharioth technique) or an iris-claw IOL.
The most difficult part of this surgery is the removal of the nucleus. There are two methods (Fig. 19.2).
Fig. 19.2
Treatment algorithm for removal of soft or hard dropped nucleus
1.
You can remove the nucleus with a fragmatome inside the vitreous cavity. In case of soft to medium-hard nuclei, I recommend working with the fragmatome. See Sect. 19.2.
2.
You can lift the nucleus with PFCL to the pupillary plane and remove it there with a conventional phaco handpiece or the SICS technique. This technique is very elegant and easy in case of a rock-hard nucleus. For details of SICS technique, see my book Complications During and After Cataract Surgery (Springer). See Sect. 19.4.
19.2 Extraction of a Posteriorly Dislocated Nucleus with Fragmatome
Video 19.1: Extraction of dropped nucleus with fragmatome and sulcus IOL
19.2.1 Introduction
Do you know which tissue you can remove with a vitreous cutter and the fragmatome? This is an important knowledge for this case. With the vitreous cutter, you can remove the cortex, epinucleus, a soft nucleus and iris tissue. You cannot remove a dense nucleus or a thick capsular fibrosis. With the fragmatome you can remove a dense nucleus and a thick capsular fibrosis. A rock-hard nucleus is hard to remove by a fragmatome. The fragmatome is less powerful than a normal phaco handpiece. To remove a rock-hard nucleus, you need to perform phacoemulsification at the pupillary plane or a SICS.
Instruments
1.
23G or 25G 3-port trocar system with chandelier light fibre
2.
120D lens
3.
Fragmatome
4.
1.3 mm V-lance for 20G sclerotomy
Individual Steps
1.
Hybrid 3-port system with chandelier light fibre
2.
Anterior vitrectomy via pars plana
3.
Removal of residual cortex from the lens capsule via paracentesis
4.
Vitrectomy, if necessary PVD
5.
20G sclerotomy at 9 o’clock
6.
Emulsification of the nucleus with fragmatome and flute needle
7.
Closure of 20G sclerotomy
8.
Trimming of vitreous base
9.
Implantation of an intraocular lens
10.
Removal of trocar cannulas