Purpose
To describe a method for staged partial resection of congenital divided eyelid nevus. The rationale, technique, and outcomes for this approach are described.
Design
Retrospective chart review of a case series.
Methods
Clinical records of 12 patients with divided eyelid nevus were reviewed with attention to presenting features, surgical management, histopathology, and follow-up course. Surgical approach involved the use of bipolar and thermal cautery to ablate the eyelid margin component, skin excision for cutaneous lesions, and then repair with advancement flaps or skin grafting.
Results
Eight patients with divided nevus were treated with a staged surgical approach: 5 primarily and 3 as revision cases. Average age was 16.3 years at primary presentation (range, 2-36 years), 16.5 years at initial surgery (range 2-36 years), and 36.0 years at presentation for revision (range, 12-72 years). Primary patients required 1 (n = 3) or 2 (n = 2) surgeries. Revision patients required 2 (n = 1) or 3 (n = 2) procedures in addition to those they had already undergone. Anterior lamellar repair was by granulation (n = 2), local skin flaps (n = 3), or skin grafts (n = 3). Average follow-up was 21.6 months (range, 0-98 months). No adverse effects or malignant transformations were seen.
Conclusions
Patients with divided eyelid nevi often present for surgical management because of cosmetic and functional concerns. Because small-to-medium congenital nevi have a low risk of malignant transformation, total excision may not be necessary. A staged surgical approach with cautery ablation and contouring of the eyelid margin component and surgical resection of the anterior lamellar portion may be a reasonable treatment strategy for these patients.
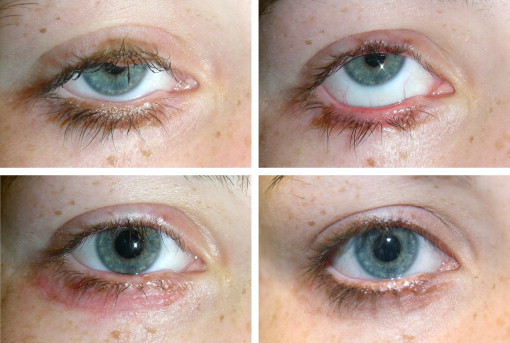
Divided nevus or kissing nevus of the eyelid is a congenital lesion in which nevus tissue is present on corresponding areas of the upper and lower eyelids of 1 eye, such that the eyelid margin components appose or “kiss” when the eyelids are closed. Although rare, divided nevi can have cosmetic, functional, and potentially neoplastic significance. These lesions arise during fetal development when neural crest–derived melanoblasts migrate into the eyelid epidermis (gestational weeks 12-14) while the eyelids are fused (weeks 9-24). The nevus is divided when the epidermis subsequently separates along the eyelid margin.
Congenital nevocellular nevi are present in approximately 1% of newborns, but rarely occur in the form of kissing nevi. Fewer than 80 cases of divided eyelid nevus have been reported in the literature since Fuchs first described the entity in 1919. Malignant transformation has been reported. A review of 55 papers from the dermatology literature concluded that the lifetime risk of congenital nevi transforming to melanoma is size dependent. The reported transformation rates of large nevi (>20 cm diameter) range broadly from 5%-40%, but when data from multiple series are compiled the estimated lifetime risk is closer to 6%-7%. Two cohort studies of medium nevi (1.5-19.9 cm) with over 200 patients each found no transformations during up to 25 years of follow-up. Risk models estimate that less than 1% of small nevi (<1.5 cm) undergo malignant transformation by age 60. Although there are no universal management guidelines, excision is recommended for large nevi while lifetime medical observation is acceptable for small and medium lesions.
Observation may not be an appropriate management strategy for some divided eyelid nevi because of cosmetic or functional concerns (ectropion, ptosis, or epiphora). Surgical management can be particularly challenging in such cases because involvement of the upper and lower eyelids limits reconstruction options. Traditionally, treatment of these lesions may include full-thickness resection with subsequent reconstruction—an approach that often results in deformity of the eyelid margin and loss of the eyelashes. Given the low risk of malignant transformation in small-to-medium congenital nevi, it may be reasonable to address the cosmetic and functional concerns without striving for total excision. The purpose of this retrospective case study is to report the authors’ experience using a combination of eyelid margin cautery and skin excision in the treatment of divided nevus of the eyelid.
Methods
The Washington University Institutional Review Board approved this retrospective review of patient data. The clinic archives were searched for diagnosis-related keywords (eyelid nevus, kissing nevus), then a retrospective chart review was performed on the records of the patients seen between March 2003 and December 2011. The retrospective data collection was performed from February 2012 to April 2012. Age, sex, race, lesion size and location, evolution, management, surgical pathology, and follow-up were collected.
The surgical management strategy was based on size, extension, lesion characteristics, and patient preferences. In general, the approach involved 2 components: eyelid margin cautery and pretarsal skin excision, as shown in Figures 1 and 2 . These stages were performed in 1 or multiple operative sessions, depending on the extent of the lesion. The same surgeon (author P.L.C.) performed all procedures except 1 (Patient 10, performed by S.M.C.). During the cautery stage, thermal and/or bipolar cautery was applied to the involved portion of the eyelid margin, ablating the nevus tissue and sculpting the remaining underlying eyelid margin to an acceptable contour. In anticipation of superficial tissue necrosis and atrophy, the eyelid margin component of the nevus was not contoured flush, but instead was left minimally elevated compared to the normal remaining eyelid. During the initial cauterization, the posterior eyelid margin was often left untreated to reduce the risk of conjunctival migration onto the margin. Residual deep pigment was left in place if the lesion depth extended beyond the targeted eyelid contour. Redundant rows of lashes were excised if necessary, but an attempt was made to preserve the normal lash line hair follicles.

A second surgical stage was undertaken with the goal of removing the anterior lamellar component of the nevus. The pigmented and/or thickened nevus tissue was resected with minimal margins, often leaving the orbicularis intact. The skin defect was then repaired with reconstructive surgical techniques appropriate to the defect size and location.
Postoperatively, topical erythromycin ophthalmic ointment was applied to cautery sites and incisions. Special care was taken to keep treated eyelid margins moist with frequent ointment applications until spontaneous epithelialization had occurred. Follow-up examinations focused on the progress of healing; eyelid function and cosmesis; scar management, if indicated (eg, steroid injection to hypertrophic grafts); and any evidence of recurrence.
Results
Twelve patients with divided nevus of the eyelid were identified. Of these, 8 had never received treatment (primary group, Table 1 ), and 4 had undergone previous excision elsewhere prior to presentation (secondary group, Table 2 ). The average age in the primary group was 20.5 years (range, 3-36 years), and in the secondary group 30.3 years (range, 12-72 years, with an average of 22.3 years elapsed since prior surgical procedure). Location was evenly distributed (right = 6, left = 6). There were 7 female and 5 male patients. The most common position was central eyelid (58%). In the primary group, average greatest dimension was 1.5 cm (range, 0.5-4.5 cm) for the upper eyelid component and 1.7 cm (range, 0.5-5.5 cm) for the lower eyelid component, with a total vertical extent averaging 1.5 cm (range, 0.6-5.5 cm) when eyelid closure brought the 2 components together.
| Patient | Age (y) | Sex | Location | Maximum Diameter (cm) | Evolution | Management (Numbered by Stage) | Postoperative Complications [Total Follow-up Interval] |
|---|---|---|---|---|---|---|---|
| 1 | 7 | M | Right, lateral | 5.5 | Enlarging |
| Skin graft hypertrophy [26 months] |
| 2 | 16 | F | Right, central | 1.5 | Enlarging since age 11 y |
| Residual margin pigment. Epilated twice for trichiasis. [15 months] |
| 3 | 8 | M | Left, central | ∼1.3 | Enlarging and darkening since age 7 y |
| None [2 months] |
| 4 | 36 | M | Left, lateral | 1.4 | Increased hair |
| Residual marginal lesion. [15 months] |
| 5 | 35 | M | Right, central | 1.0 | Enlarging |
| Residual margin pigment. [6 months] |
| 6 | 3 | F | Right, medial | 1.0 | Enlarging and darkening since age 2 y | None | NA [0 months] |
| 7 | 34 | M | Right, lateral | 1.0 | Enlarging and increased hair | None | NA [0 months] |
| 8 | 25 | F | Left, central | 0.5 | None noted. Incidental finding. | None | NA [40 months] |
| Patient | 1 o Age (y) | 2 o Age (y) | Sex | Location | Prior Procedures | Condition of Eyelids at 2 o Presentation | Evolution | Management (Numbered by Stage) | Postoperative Complications [Total Follow-up Interval] |
|---|---|---|---|---|---|---|---|---|---|
| 9 | 2 | 12 | F | Right, central | LL resected. Revision at age 3 y | UL: Elevated residual pretarsal and marginal lesion. LL: Cheek flap, cicatricial ectropion, 1 mm lag. | Enlarging, darkening, and increased hair |
| Margin thinning. Lash rotation, with 1 episode of trichiasis. Residual margin pigment. Conjunctival overgrowth resolved with LMC. <0.5 mm lag. [26 months] |
| 10 | 22 | 72 | F | Left, central | UL and LL resection | UL and LL: Regrowth of marginal and pretarsal lesions. Intermittent lag. | Enlarging, and increased hair |
| None [2 months] |
| 11 | 4 | 24 | F | Left, medial | UL and LL resected, with FTSG. Canthal revision at age 14 y. Two laser treatments. | UL: FTSG, cicatricial ectropion, margin and brow pigment. LL: Thickened graft with visible crease, cicatricial ectropion, margin pigment, and 2 mm lag. | Decreasing pigmentation since childhood |
| Skin graft hypertrophy. UL hooding after 1st stage, improved by 3rd procedure. 0.5 mm lag. [29 months] |
| 12 | 4 | 13 | F | Left, total UL, medial LL | UL and LL laser ablation at medial canthus. Tissue expander age 10 y (removed because of infection). LL FTSG age 11 y. | UL: Pretarsal nevus 3.5 cm diameter. LL: cicatricial ectropion; thickened graft; residual marginal lesion extending to nasal sidewall. | Enlarging and darkening | None. Patient went elsewhere for pretarsal laser ablation. | NA [98 months] |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


