Purpose
To understand the prognosis of polypoidal choroidal vasculopathy (PCV) by evaluating the responsiveness to intravitreal ranibizumab (IVR) monotherapy according to the presence of a single or multiple polyps.
Design
Retrospective case series.
Methods
We included 48 treatment-naïve eyes of 48 patients who received IVR monotherapy at the Medical Retina Division Clinic, Keio University Hospital between March 2009 and January 2013 and attended the clinic for at least 12 months. All patients received 3 monthly IVR injections followed by pro re nata injections and were divided into single polyp and multiple polyps groups according to indocyanine green angiography and optical coherence tomography (OCT) findings. The outcome measures included changes in best-corrected visual acuity (BCVA) and OCT findings over 2 years after initial IVR.
Results
At baseline, the multiple polyps group exhibited a poorer BCVA, larger greatest linear dimension, and higher prevalence of fibrovascular pigment epithelial detachment compared with the single polyp group. Over 2 years, the multiple polyps group showed no improvement in BCVA, although the central retinal thickness (CRT) decreased in both groups. The multiple polyps group exhibited a significantly greater CRT at 1 year and required more injections in the first year compared with the single polyp group; furthermore, it included a higher number of nonresponders judged either by BCVA or fundus findings at 1 year and fundus findings at 2 years.
Conclusions
We propose that the stratification of PCV lesions according to the presence of single or multiple polyps may be valuable to understand the prognosis.
Recent progress in molecular targeting therapies has improved the overall prognosis of age-related macular degeneration (AMD), a leading cause of blindness worldwide. While most patients receive benefits from treatment with intravitreal anti–vascular endothelial growth factors (anti-VEGFs) such as ranibizumab (IVR) and aflibercept (IVA), treatment response is not always consistent among patients. This can be attributed to differences in the pathogenesis of AMD among individuals.
Generally, AMD is divided into 3 subtypes: typical AMD, polypoidal choroidal vasculopathy (PCV), and retinal angiomatous proliferation (RAP). PCV, which accounts for almost 50% of AMD patients in Asian countries, is characterized by polypoidal lesions with or without a branching vascular network (BVN) detected by indocyanine green angiography (ICGA). Most patients with PCV exhibit unilateral disease, similar to those with typical AMD, and do not frequently develop drusen in the unaffected eye, as opposed to RAP, which carries a poorer prognosis compared with PCV and typical AMD. Because of differences in the clinical course and therapeutic response, it is important to differentiate between PCV and typical AMD, although patients with both PCV and typical AMD in a single eye have also been reported. Moreover, reports of the posttreatment prognosis of PCV patients are inconsistent among clinical studies. For example, a randomized study (the EVEREST study) compared the efficacy of IVR and photodynamic therapy (PDT) for the treatment of PCV and concluded that the latter was more effective in achieving polyp regression. In contrast, another study (the LAPTOP study) showed that IVR monotherapy was superior to PDT. These differences probably occurred because of the lack of detailed classifications for the different variants of PCV that exhibit different responses to treatment. Therefore, classifications that accurately represent the prognosis of each variant are desirable.
We previously reported that nonresponders to IVR among patients with different subtypes of AMD exhibit unique fundus findings at baseline. In the same study, initial fibrovascular pigment epithelial detachment (PED), serous PED, and type 1 choroidal neovascularization were found to be associated with a lack of response to IVR. In the current study, we divided PCV patients into 2 groups on the basis of the presence of a single or multiple polyps and retrospectively analyzed their responsiveness to IVR monotherapy to derive information that will aid in understanding the pathologic course and predicting the prognoses of patients with different variants of PCV treated by IVR monotherapy.
Methods
This retrospective case series was based on a detailed medical chart review, followed the tenets of the Declaration of Helsinki, and was retrospectively approved by the Ethics Committee of Keio University School of Medicine (No. 2010002) and registered with UMIN-CTR (UMIN000007649).
Study Participants
In total, 68 consecutive eyes of 65 patients were diagnosed with PCV. From these, we included 48 eyes of 48 patients with PCV-induced visual loss who received IVR monotherapy at the Medical Retina Division Clinic (AMD Clinic) of the Department of Ophthalmology, Keio University Hospital (Tokyo, Japan) between March 2009 and January 2013. During this period, aflibercept, which was first approved in Japan in November 2012, and another off-label anti-VEGF drug for AMD, bevacizumab, were not used at the hospital. Thus, all PCV patients who needed anti-VEGF therapy were treated with IVR. All patients had attended our clinic for at least 12 months, during which time no medication other than IVR was administered. Patients who had received any other treatment for AMD in the past were excluded; thus, all participants were treatment naïve. All patients who began receiving treatments other than IVR monotherapy after the first year were considered dropouts, and their data before the initiation of another treatment were analyzed. All patients provided informed consent for the use of their data for research purposes.
Ophthalmologic Examinations
All patients underwent best-corrected visual acuity (BCVA) measurements using refraction tests, slit-lamp examinations, and binocular indirect ophthalmoscopy after pupil dilation with 0.5% tropicamide throughout the study.
Fluorescein and Indocyanine Green Angiographies
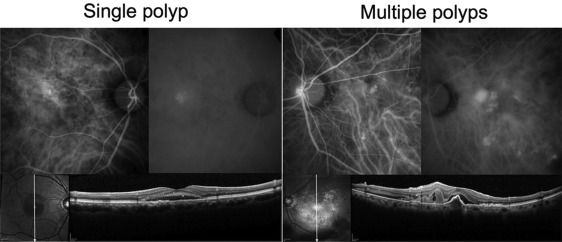
Fluorescein angiography and ICGA were performed for AMD diagnosis and PCV definition using a Topcon TRC 50DX retinal camera (Topcon Corporation, Tokyo, Japan). According to the findings of ICGA and optical coherence tomography (OCT), the patients were divided into the single polyp and multiple polyps groups ( Figure 1 ).
Optical Coherence Tomography
OCT was performed at every follow-up visit using a Heidelberg Spectralis OCT system (Heidelberg Engineering GmbH, Dossenheim, Germany). The OCT images were used to evaluate central retinal thickness (CRT), central choroidal thickness (CCT), and AMD lesions, including PED. CRT was defined as the distance between the internal limiting membrane and the presumed retinal pigment epithelium (RPE) at the fovea. CCT was defined as the distance from the hyperreflective line corresponding to the Bruch membrane beneath the RPE and the inner surface of the sclera at the foveal center, and was manually measured using the caliper function of the OCT device. Measurements were obtained using the scale bars of the OCT system for reference. A dry macula was defined as the resolution of intra- and subretinal fluid detected by OCT with reference to fundus findings, and in particular to an increase or decrease in hemorrhages. Changes in hemorrhages (eg, retinal or subretinal hemorrhage or hemorrhagic PED) were not always detected by OCT, but could respond to AMD activity. Thus, we also checked fundus photography and excluded those who had increased hemorrhagic findings from the patients with dry macula.
Intravitreal Ranibizumab Monotherapy and Follow-up
In the induction phase, ranibizumab (0.5 mg, 0.05 mL) was intravitreally injected via the pars plana under sterile conditions once a month for 3 months. The injections were repeated if follow-up OCT showed evidence of any fluid in the macula, identified as macular edema, subretinal fluid, or PED enlargement. Follow-ups were generally conducted every month after therapy initiation, but in cases where no fluid or hemorrhage was detected for more than 2 months, the interval was extended up to 2 months. Any new intra- or subretinal hemorrhage or unexplained visual loss represented by an increase of >0.2 in logMAR BCVA was treated as appropriate. At each follow-up visit, BCVA was measured and other ophthalmologic examinations, including OCT, were performed.
Definition of Nonresponders to Intravitreal Ranibizumab
Nonresponders were defined on the basis of BCVA or fundus findings, as previously reported. Briefly, patients with an increase of >0.2 in logMAR score at 1 or 2 years after initial IVR therapy were judged as nonresponders on the basis of BCVA. On the basis of fundus findings, nonresponders were judged as patients with aggravated or fresh exudative fundus findings (PED, subretinal fluid, macular edema, or hemorrhage) even after treatment, or those with an increase of >100 μm in CRT between baseline and 1 or 2 years after initial IVR therapy.
Statistical Analyses
Data are expressed as means ± standard deviations (SDs). Commercially available software (SPSS, version 21.0; SPSS Japan, Tokyo, Japan) was used for all statistical analyses. The Mann-Whitney U test, χ 2 test, multiple regression analyses, or Spearman rank correlation coefficient was used for comparisons, and a P value of <.05 was considered statistically significant.
Results
Among the 48 PCV treatment-naïve patients, 29 eyes of 29 patients (22 men and 7 women) exhibited a single polyp and 19 eyes of 19 patients (12 men and 7 women) exhibited multiple polyps on baseline ICGA before IVR treatment. Among the multiple polyps group, 2, 3, 4, 5, 6, 7, and 12 polyps were found in 4, 4, 3, 1, 3, 3, and 1 patient, respectively. There were 5 dropouts in the second year of treatment, including 1 patient in the single polyp group who was lost to follow-up, 1 patient each in both groups who changed their treatments, and 2 patients in the multiple polyps group who underwent vitrectomy for PCV-associated vitreous hemorrhage.
At baseline, the mean BCVA was significantly poorer in the multiple polyps group than in the single polyp group ( Table 1 , P = .017), while the mean greatest linear dimension (GLD) was larger in the multiple polyps group than in the single polyp group ( P = .009). Furthermore, the number of eyes with fibrovascular PED (f-PED), as detected by fluorescein angiography and OCT, was greater in the multiple polyps group than in the single polyp group ( P = .004). All f-PED lesions corresponded to the presence of a BVN in the multiple polyps group. There was no significant difference in age, sex, baseline CRT, baseline CCT, or follow-up duration between the 2 groups.
| Single Polyp | Multiple Polyps | P Value | |
|---|---|---|---|
| Age (y) | 72.1 ± 9.4 | 72.7 ± 7.5 | .72 |
| Sex, male [female] | 22 [7] | 12 [7] | .517 |
| Best-corrected visual acuity (logMAR) | 0.18 ± 0.26 | 0.37 ± 0.30 | .017 a |
| Greatest linear dimension (μm) | 2950.8 ± 3237.3 | 4084.4 ± 1926.4 | .009 b |
| Central retinal thickness (μm) | 394.6 ± 156.8 | 384.1 ± 183.6 | .591 |
| Central choroidal thickness (μm) | 218.9 ± 61.7 | 251.3 ± 85.7 | .117 |
| Fibrovascular retinal pigment epithelial detachment, eyes [%] | 5 [29%] | 11 [57.9%] | .004 b |
| Follow-up period (mo) | 22.5 ± 3.2 | 20.7 ± 4.8 | .116 |
The mean BCVA in the single polyp group showed significant improvement at each point compared with that at baseline ( Figure 2 ), while it remained unchanged in the multiple polyps group. Moreover, the mean BCVA was significantly poorer in the multiple polyps group than in the single polyp group at all time points of assessment ( Figure 3 ; 3 months, P = .04; 1 year, P = .003; 2 years, P = .002), although there was no intergroup difference in mean changes in BCVA at any time point (data not shown).
In total, 21 of 29 eyes (96.6%) in the single polyp group and 14 of 19 eyes (72.2%) in the multiple polyps groups showed maintained or improved BCVA at 1 year after initial IVR therapy ( P = .019), while 21 of 27 eyes (96.4%) and 13 of 16 eyes (81.3%), respectively, showed maintained or improved BCVA at 2 years ( P = .262) ( Figure 3 ).
The mean CRT at 3 months exhibited a decrease relative to that at baseline and remained low throughout 2 years of treatment in both groups ( Figure 4 ). At 1 year, however, the mean CRT was significantly greater in the multiple polyps group (297.5 ± 127.4 μm) than in the single polyp group (226.6 ± 114.4 μm; P = .009), with a significantly smaller mean CRT change in the former (101.2 ± 116.1 μm) than in the latter (168.0 ± 178.6 μm; P = .042).
Interestingly, the numbers of IVR injections in the first and second years were 4.4 ± 2.1 and 1.7 ± 2.0, respectively, in the single polyp group and 6.0 ± 2.5 and 2.3 ± 2.4, respectively, in the multiple polyps group, indicating a significant difference in the first year ( Figure 5 , P = .009).
Intra- and subretinal exudative changes had disappeared after the initial 3 injections in 28 eyes (96.6%) in the single polyp group and 15 eyes (78.9%) in the multiple polyps group ( Table 2 ); the eyes in the latter group showed a greater tendency for residual exudative changes after the induction phase ( P = .051). The mean number of injections required before the first complete disappearance of intra- and subretinal exudative changes and the achievement of a dry macula were 3.4 ± 1.4 and 4.9 ± 3.3 in the single polyp and multiple polyps groups, respectively ( Table 2 ; P = .054). Among eyes in which a dry macula was achieved, the durations between the last injection before observation of a dry macula and the subsequent injection for recurrence were 11.4 ± 7.1 months and 5.9 ± 6.4 months in the single polyp and multiple polyps groups, respectively, with a significant difference between the groups ( Table 2 ; P = .005). Fifteen eyes, including 13 (44.8%) in the single polyp group and 2 (10.5%) in the multiple polyps group ( Table 2 ; P = .003), needed no further injections for more than a year after the first remission.



