Categories of Tears and Their Function
Tears play a vital role in visual clarity, ocular health, and emotional expression. Three categories of tears are produced, as discussed below.
Basal Tears
In all mammals, the ocular surface is kept moist by basal tears. These lubricate the cornea and allow the eyelids to sweep across the eye without friction, constantly removing foreign debris from the visual axis.
The avascular cornea depends on the tear film to deliver nutrients and oxygen to the epithelial cells, as well as to remove waste products.10
Immunoglobulins and lysozymes within the basal tears help protect the cornea from invasive pathogens. Lysozyme degrades peptidoglycan in gram positive bacteria membranes (see Chapter 10).11
Visual clarity and refraction of light depends on the smooth surface created by a healthy tear film, swept evenly across the irregular epithelial surface with each blink.
Reflex Tears
Reflex tears are produced in response to an ocular irritant. Causes include eyelid malposition, abnormalities in the basal tear constituents, ocular surface breakdown, foreign material, airborne irritants (smoke, onions, allergens), and bright light or glare. Overly spicy foods, strong odors, and stimulation of the posterior nasal passages may also induce reflex tearing. Eye strain, coughing, and yawning cause tearing in some individuals.12
Reflex tears depend on a sensory afferent pathway from the corneal nerves via the ophthalmic division of the trigeminal nerve (V1) and an efferent parasympathetic pathway carried with the lacrimal nerve following synapse in the sphenopalatine ganglion (see Chapters 1 and 31). Their function is to flush and protect the eye from noxious agents, and they contain higher concentrations of lysozyme and immunoglobulins compared with basal tears.
Emotional (Psychic) Tears
Humans are the only animals known to weep or cry in response to strong emotions (sadness, elation, anger, or pain). Weeping is often accompanied by convulsive breathing, facial congestion, and obvious expressive changes.
Emotional tears have different chemical constituents from those of either basal or reflex tears, with increased levels of two stress-related hormones (prolactin and adrenocorticotropin), as well as leucine enkephalin (an internal pain regulator). Weeping may, therefore, be a means of expelling excessive stress hormones.13
Psychologists have also demonstrated that weeping is a powerful signal to others that indicates genuine emotional strain, often eliciting a comforting response.
Emotional tears are controlled by hormonal signals from the hypothalamus, indirectly stimulating the parasympathetic fibers within the lacrimal nerve, and do not depend on the afferent sensory pathway, unlike reflex tearing.14
The Lacrimal Pathway
The normal lacrimal pathway consists of three stages (Fig. 30.2): (1) tear production (secretion), (2) tear distribution, and (3) elimination (excretion).12 The physiology, pathogenesis, clinical features, investigation, and management for each of these three phases will be described consecutively.

Tear Production (Secretion)
Tear Film Components
The normal tear film is composed of three layers (Fig. 30.3):15
1. A thin (1 µm) mucinous layer produced by conjunctival goblet cells, which smooths the irregular corneal epithelial layer to improve optical clarity and facilitates binding of the aqueous tears onto the hydrophobic epithelial villae.
2. The broad (3–8 µm) middle aqueous layer produced by the lacrimal gland and accessory lacrimal glands (Krause in the conjunctival fornix and Wolfring within the palpebral conjunctiva). The accessory glands are responsible for baseline tear secretion (basal tear layer), whereas the lacrimal gland is innervated by parasympathetic innervation via the lacrimal gland and produces reflex tears in response to ocular surface irritation and emotional tears. If the lacrimal nerve is severed or the lacrimal gland excised, the basal tear secretion remains intact, so the eye remains moist, but no reflex or emotional tears are produced. In cases of anesthesia of the ophthalmic division of the trigeminal nerve, reflex tears are no longer produced (potentially leading to neurotrophic corneal ulcers), but emotional tears can still be released.
3. A thin (0.1–0.2 µm) outer oily layer on the surface of the tear film (meibum) produced primarily by the Meibomian glands on the lid margin, and to a lesser extent by the glands of Zeis associated with the lash follicles. This layer improves tear film cohesiveness and helps reduce evaporation.

Pathogenesis and Etiology
Altered production in any of these three components may result in an abnormal or unstable tear chemistry, which can lead to ocular surface disease with visual disturbance, ocular irritation, and reflex lacrimation.15
Reduced Production (Dry Eye Syndrome)
Dry eye syndrome (DES) is a common tear film disorder caused by decreased production of various tear components or increased evaporation. Changes in the tear film composition cause release of proinflammatory mediators by surface epithelial cells, resulting in further injury and destruction of both epithelial and mucin-producing goblet cells.
Reduced aqueous production (keratoconjunctivitis sicca) is caused by:
▪ Age: The accessory lacrimal glands produce fewer tears with advancing age, particularly following menopause. The prevalence of symptomatic keratoconjunctivitis sicca ranges from 8.4% in those younger than 60 years old to 20% in those older than 80 years.16
▪ Medications: Antihistamines, decongestants, hormone replacement therapy, antidepressants, and antiparkinsonian medications.
▪ Inflammation or destruction of the lacrimal and accessory glands: Rheumatoid arthritis, scleroderma, Sjögren syndrome, thyroid disorders, diabetes, radiotherapy, and vitamin A deficiency.17
▪ Conjunctival scarring damaging lacrimal gland ducts and accessory glands: Stevens-Johnson syndrome, cicatricial pemphigoid, alkali burns, surgery.
▪ Damage to corneal nerves (post refractive laser): This is usually temporary.
Reduced mucin production is caused by autoimmune inflammatory disease and chronic dry eyes. Cytokines released by inflamed or metaplastic epithelial cells have been shown to cause reduction in goblet cell populations, both in tissue biopsies and impression cytology, as well as in cell cultures from animal models.18 Lack of mucin results in poor tear film adhesion and further epithelial metaplasia and keratinization.
Reduced sebum production is primarily caused by posterior blepharitis (Meibomian gland disease (MGD)) and less commonly by autoimmune inflammatory conditions. Reduced secretion of meibum into the tear film results in an unstable tear film and easier evaporation.
Increased Production (Hypersecretion, Reflex Tears)
Hypersecretion of tears results from lacrimal gland stimulation, often a response to ocular surface irritants. The etiology includes anterior seborrheic or infective blepharitis (see Chapter 10), eyelid malpositions (entropion, ectropion, retraction, or trichiasis), or ocular contact sensitivities (including topical drops, their preservatives, or airborne irritants).
Paradoxically, the condition “dry eyes” from reduced mucin, basal aqueous, or sebum secretion, as described above, often leads to a compensatory reflex tearing.
In some individuals, simple exposure to bright light, glare, cold, or windy conditions may be sufficient to induce significant reflex tearing.
Gustatory tears are occasionally seen in individuals with previous facial nerve palsy in whom the secretory nerve fibers to the salivary glands are redirected to the lacrimal gland (see Chapter 31).19 These individuals may tear in response to savory smells or while eating. The term “crocodile tears” is sometimes used reflecting the belief that crocodiles tear when eating their prey. This is also the derivation of the term “crocodile tears” referring to insincere sympathy.
Epidemiology
The Dry Eye Workshop (DEWS 2007) estimated the prevalence of keratoconjunctivitis worldwide to be 5% to 30% in those over age 50 years, with the ratio of affected females to males being 2 : 1. Use of contact lenses increases the risk of ocular surface disease, as does the use of the various medications listed above.20
Clinical Features
Dry Eye Symptoms and Signs
Dry eye symptoms and signs usually affect both eyes. They include:
▪ Burning, stinging, or scratchy sensation
▪ Stringy mucus or corneal filaments
▪ Photophobia, with impaired night vision
The ocular surface disease index (OSDI) is a questionnaire that is divided into three subscales: vision-related function, ocular symptoms, and environmental triggers. It is primarily a research instrument to measure the severity of DES, although is also promoted as a screening survey.21
Ocular examination may reveal a decreased tear meniscus from reduced aqueous production, rapid formation of dry spots from lack of mucin production, or Meibomian gland disease with inspissation, inflammation, and atrophy of the posterior lid margin sebaceous glands (Fig. 30.4).

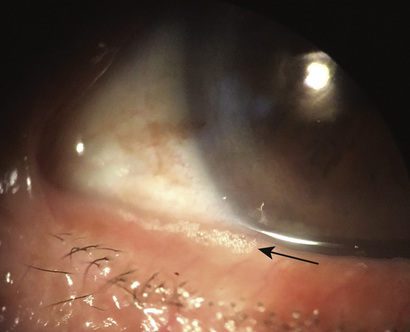
Damage to the corneal epithelium may be evident with punctate erosions or, in severe cases, ulceration. Filamentary keratitis, characterized by mucus tails tethered to the surface epithelium, may be a sign of decreased aqueous. A foamy tear film may suggest soap production by bacterial pathogens within plugged Meibomian glands (Fig. 30.5) (see Chapter 10).
Reflex Tears
The hallmark of reflex tearing is intermittent gushing of tears, often associated with symptoms of ocular surface irritation or burning, depending on the etiology. One or both eyes may be affected. The tearing may be aggravated by certain conditions such as reading, using the computer or watching television (when the blink rate reduces, allowing greater evaporation), use of contact lenses, and exposure to heat or to cold wind. Ocular examination may identify ocular surface disease changes (as listed above), a variable tear meniscus, and obvious lid margin pathology, including anterior blepharitis, trichiasis, or lid malpositions.
Investigations
Tear Volume Tests
The height of the tear meniscus (tear lake) can be estimated by the experienced clinician as being reduced and flattened in DES and elevated in cases of lacrimal outflow obstruction. The height can be measured with the micrometer on the slit lamp beam: a height less than 0.2 mm suggests decreased tear production.22 It may be easier to visualize the tear lake after staining with green, yellow, or blue dye (Fig. 30.6).

Schirmer tests measure the amount of tears soaking a 5 × 35 mm filter paper with tears for 5 minutes; the folded end of the paper is placed over the lid margin at the junction of the lateral and central third to avoid corneal touch. In the basal tear test (Schirmer 1), topical anesthetic is used and blotted dry before the strip is placed. A length of wetting less than 6 to 8 mm after 5 minutes signifies a dry eye. An approximation can also be made by measuring the length of soaking after 1 minute and multiplying by three. The Schirmer 2 test does not use topical anesthetic, and a significant increase in strip wetting compared with the Schirmer 1 test represents the component contributed by reflex tears (Fig. 30.7).23

In the phenol red test, a cotton thread containing phenol red dye is placed over the lid margin. Tears cause the yellow thread to turn red on contact; the amount of wetting is measured after 15 seconds and is considered low if less than 9 mm.24
Tear Stability Tests
In the tear film breakup test, fluorescein placed on the ocular surface is spread across the tear film with each blink (Fig. 30.8). The tear breakup time is the duration from last blink until dark patches appear on the fluorescein-stained tear film when viewed with the bright cobalt blue light on slit lamp biomicroscopy. A rapid breakup time of less than 10 seconds indicates a dry eye with goblet cell depletion (lack of mucin).24

Tear Stain Tests
The fluorescein dye identifies breakdown in corneal epithelial junctions, allowing the dye to stain the underlying basement membrane. The Rose Bengal dye is a more sensitive test, identifying areas of devitalized epithelium even before frank erosions have developed (Fig. 30.9). It is less commonly available now.24

Hyperosmolarity Tests
High osmolarity related to decreased aqueous production is an important hallmark of DES.20
Controversy: Recently, devices to measure tear osmolarity have become commercially available but are still used more at the research level. Lipid profiles based on tear film distribution have also become available to help diagnose MGD but have not been widely accepted.
Management
Dry Eye Syndrome
Initial diagnosis and management of mild DES can be performed by the family practitioner or optometrist with the use of tear replacement drops.25
▪ Tear replacement: Various tear substitutes are available in over-the-counter preparations. The formulas vary in terms of component electrolytes, viscosity, and preservatives. The ideal substitute for DES should match normal tear attributes: pH 6.5–7.6; osmolarity 302 +/− 6.3 mOsm/L; viscosity 6–12 centiPoise (cps).26 As hyperosmolarity is a common feature of DES and may be partly responsible for symptoms and toxicity, many preparations are hypotonic.
▪ Short-acting agents are based on polyvinyl alcohol or carboxy-methylcellulose, whereas longer-acting substitutes contain aqueous carbomer gels. These wetting agents are limited by short-term benefit. Petrolatum oil ointments (Lacrilube) or aqueous-based gels (Genteal Gel) are useful for overnight therapy primarily. In general, more viscous agents have a longer effect but may blur vision more.
▪ Nonpreserved tear substitutes are packaged in small disposable vials, eliminating the risk of contact sensitivity from preservatives. Some newer preservatives dissipate on contact with the ocular surface, thus reducing the risk of allergies.
▪ Autologous serum drops: These are produced by centrifuging the recipient’s serum. They have similar biochemical and mechanical properties to normal aqueous tears and may be considered in severe cases where epithelial breakdown is evident or in neurotrophic ulcers.27
▪ Mucolytic agents: Acetylcysteine drops help break up mucus filaments in filamentary keratitis.
▪ Punctal occlusion: These procedures are usually performed for more serious DES; they reduce drainage of existing tears or supplementary drops with the hope of reducing the need for tear substitutes. Trial plugs are dissolving intracanalicular rods (often composed of collagen), which help predict the benefit of occlusion. External plugs are capped with a flange flush to the lid margin (Fig. 30.10). Indwelling plugs such as the “smart plug” have largely fallen out of favor because of secondary canalicular scars, canaliculitis, or pyogenic granulomas. The lower punctum is usually plugged first; rarely, in severe cases, the upper punctum is also blocked.28

Controversy: Thermal cautery occlusion is an option but requires a local anesthetic injection; the anesthesia may be harder to reverse, so this method often is reserved for cases in which external plugs fall out repeatedly.
▪ Dilute sodium hyaluronate 0.18% is effective at reducing DES symptomatology but also reverses epithelial damage, restoring ocular surface morphology.29
▪ Topical anti-inflammatories: Topical diclofenac or corticosteroids may be used transiently to settle some inflammatory changes associated with DES until slower-onset therapeutic agents can become effective.
▪ Vitamin A eye drops (0.01% all-trans retinoic acid) may prolong tear breakup times.30
▪ Cyclosporin A 0.05% emulsion (Restasis) has been shown to increase production of tears and reverse goblet cell depletion and restore epithelial cell damage, presumably by reducing the toxic effects of inflammation in more severe cases of DES. It has not shown any benefit in patients using punctal plugs or on other anti-inflammatory drops.31 It is often prescribed with a corticosteroid drop initially to mitigate its burning sensation and, until the therapeutic effect of the drop initiates, often several weeks after first use.
▪ Therapy for MGD: Standard treatment for MGD is described in Chapter 10 and consists of an escalating regimen of eyelid hygiene with soapy scrubs, hot compresses, combined antibiotic and corticosteroid ointments or drops, fish oil supplements, and oral tetracyclines.
▪ Therapy for ocular pemphigoid and Stevens-Johnson syndrome: See Chapter 13.
Reflex Tears
The primary goal in managing reflex tearing is to identify underlying causes based on the clinical examination as outlined in the section on the clinical features of reflex tears.
The most common etiology is DES, and a simple trial of tear supplements may confirm this.
Anterior blepharitis therapy (including identification and treatment of staphylococcal or Demodex infections) is covered in Chapter 10.
Trichiasis and lid malpositions causing ocular surface irritation are identified. Their management is described in Chapter 29.
Hyperreflexive lacrimation in response to environmental factors may be managed by the use of dark glasses for glare or warm teardrops for wind sensitivity.
Nonresponsive cases and gustatory tears may be treated with neurotoxin injection into the palpebral lacrimal gland. The patient looks down and inward, the upper lid is lifted to expose the palpebral lobe, and six units of botulinum toxin type A is injected directly into the gland (Fig. 30.11). This may be very effective for 3 to 4 months. Diffusion of the medicine may occasionally cause a transient upper lid ptosis or abduction weakness, but this typically resolves within 2 weeks.

Complications and Disease Course
DES typically is a chronic condition requiring ongoing therapy for comfort. Severe cases may lead to corneal epithelial breakdown or infection and significantly impact quality of life or ability to function.
Reflex tears are more likely to be controlled if the underlying pathology is identified and treated.
Tear Distribution
Eyelid Anatomy and Tear Flow
The secreted components of the tear film are swept evenly across the surface of the eye and toward the inner canthus with each blink. This requires a healthy lid margin that is well opposed to the ocular surface along the full length of the lids.32 An upward slant at the lateral canthus steers the tears medially and reduces the risk of temporal spillage. The plica semilunaris and caruncle act as a barrier medially to contain the displaced tears within the lacrimal lake before excretion through the outflow channels (Fig. 30.12).

The tear pump is a complex mechanism that plays an important role in lacrimal distribution and excretion (see Chapter 1). The palpebral portion of the orbicularis muscle can be conceptualized as having a pretarsal and preseptal component. The superficial heads of the two muscles form the medial canthal tendon (MCT), anchoring the medial portion of the eyelid into the nasal bone. The deep heads of the pretarsal muscle (Horner muscle) insert into the posterior lacrimal crest, contouring the medial eyelids along the surface of the eye. The deep head of the preseptal muscle (the Jones muscle) inserts into the lacrimal sac fascia, creating negative pressure in the sac with each blink.
As the eyelids close, they squeeze tears toward the lacrimal lake. The puncta are pulled nasally while the lacrimal sac is expanded, drawing fluid into its lumen. As the eyelids open, the puncta are redirected into the lacrimal lake, and the sac collapses and propels the tears through the duct to the nose (Fig. 30.13). The valve of Rosenmuller at the common canaliculus helps prevent retrograde flow of tears back onto the eye as the sac contracts.33

Pathogenesis and Etiology
Eyelid ectropion or horizontal laxity, inferior displacement of the lateral canthus, poor apposition or discontinuity in the eyelid margin, or weakness in orbicularis function all may contribute to poor distribution of tears and functional impairment of lacrimal excretion.
The etiology of facial nerve palsy is described in Chapter 31.
Epidemiology
Poor tear distribution caused by horizontal laxity is more common in older adults and often aggravated by wiping tears from the eye (Fig. 30.14).

Facial palsy caused by idiopathic or congenital causes is most commonly identified in those younger than 20 years. Those associated with acoustic neuromas or vascular infarcts are most commonly seen in those older than 40 years.34
Clinical Features
Disruption in tear distribution may manifest as nonirritative pooling of tears with intermittent visual disturbance and spurting of tears with forced blinking.
Clinical examination may identify abnormal lid contour, horizontal laxity, or facial palsy (Fig. 30.15). A clue to mild facial weakness is aberrant regeneration with facial synkinesis (identified as twitching of the ipsilateral corner of the mouth or platysma muscle with each closure of the eyelid). Facial synkinesis may occasionally be mistaken for hemifacial spasm (see Chapter 32).

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


