Disorders of Pupillary Function
The value of observation of pupillary size and motility in the evaluation of patients with neurologic disease cannot be overemphasized. In many patients with visual loss, an abnormal pupillary response is the only objective sign of organic visual dysfunction.
Efferent Abnormalities: Anisocoria
Efferent disturbances of the pupil are usually unilateral and thus produce a difference in the size of the pupils called anisocoria. When assessing the pupils, one should always attempt to determine if anisocoria is present. If anisocoria is present, there is often something wrong with one or both irides or with the innervation of the iris muscles. Accordingly, once anisocoria is found, the examiner should determine not only if anisocoria is more noticeable in dim or bright illumination, but also which pupil has abnormal reactivity and/or dilation. Specific pupil examination techniques are discussed in Chapter 14. Causes of anisocoria are described below and are outlined in Table 15.1.
Physiologic Anisocoria (Simple Anisocoria, Central Anisocoria, Benign Anisocoria)
In dim light, at least 20% of the normal population has an anisocoria of 0.4 mm or more at the moment of the examination. In room light, this number drops to about 10%. This form of anisocoria, called physiologic anisocoria, is rarely more than 0.6 mm, but it may be as much as 1.0 mm (Fig. 15.1). The anisocoria is almost the same in light and in dark, but there is a tendency for it to decrease in light, perhaps because the smaller pupil reaches the zone of mechanical resistance first, giving the larger pupil a chance to catch up. Other terms for physiologic anisocoria are “simple anisocoria,” “central anisocoria,” and “benign anisocoria.”
In a patient with physiologic anisocoria, the amount of pupillary inequality may vary. Physiologic anisocoria may be observed in prior pictures, even back to infancy or early childhood. The anisocoria seldom reverses.
Horner Syndrome
When the sympathetic innervation to the eye is interrupted, the retractor muscles in the eyelids are weakened, allowing the upper lid to droop and the lower lid to rise. The dilator muscle of the iris is weakened, allowing the pupil to become smaller, and vasomotor and sudomotor control of parts of the face may be lost. This combination of ptosis, miosis, and anhidrosis is called Horner syndrome (Fig. 15.2, Video 15.1).
Clinical Features
The affected eye often looks small or sunken in patients with Horner syndrome. The upper eyelid is slightly ptotic because of paralysis of the sympathetically innervated smooth muscle (Müller muscle) that contributes to the position of the opened upper eyelid. This ptosis is sometimes so slight or so variable that it escapes attention. Similar smooth muscle fibers in the lower eyelid also lose their nerve supply in Horner syndrome. Thus, the lower lid is usually slightly elevated, producing an “upside-down
ptosis,” further narrowing of the palpebral fissure, and an apparent enophthalmos.
ptosis,” further narrowing of the palpebral fissure, and an apparent enophthalmos.
Table 15.1 Causes of Anisocoria | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
The palsy of the iris dilator muscle in Horner syndrome allows the iris sphincter to constrict, producing miosis. If the dilator muscle is stimulated (e.g., after an adrenergic eye drop is used), the pupil will dilate widely. Endogenous catecholamines can produce a similar phenomenon if the iris dilator muscle is supersensitive because of denervation. This “paradoxical pupillary dilation” is caused by denervation supersensitivity of the dilator muscle to circulating adrenergic substances.
 Figure 15.1 Physiologic (simple) anisocoria in a teenage male with a history of migraine headache; right pupil is 0.3 mm larger than left. Both pupils reacted normally to light and near stimulus. |
 Figure 15.2 Horner syndrome in two patients. A: Congenital right Horner syndrome. Note associated heterochromia iridis and minimal ptosis. B: Spontaneous left Horner syndrome showing upper eyelid ptosis and lower eyelid elevation. C: Anisocoria better demonstrated with eyelids manually raised. Video 15.1: Infrared pupillography in a patient with left Horner syndrome. Starting in darkness, anisocoria is present but of small magnitude. With light, both pupils show brisk constriction, and anisocoria is accentuated when the light is turned off because of dilation lag in the affected eye (Courtesy of Randy H. Kardon, MD.) |
In Horner syndrome, the weakness of the dilator muscle is most apparent in darkness. The anisocoria is greater in the dark and almost disappears in light. The anisocoria of Horner syndrome is diminished in bright light because the normal action of both sphincters tends to make the two pupils more nearly equal.
Paresis of the dilator muscle in Horner syndrome can be detected in several ways. When the lights are turned out, the Horner pupil dilates more slowly than
the normal pupil (dilation lag). A sudden noise will produce an increased sympathetic discharge to the dilator muscle resulting in a transient increase in anisocoria. When looking for dilation lag in a patient with anisocoria that may be caused by Horner syndrome, it is helpful to interject a sudden noise just after the lights go out.
the normal pupil (dilation lag). A sudden noise will produce an increased sympathetic discharge to the dilator muscle resulting in a transient increase in anisocoria. When looking for dilation lag in a patient with anisocoria that may be caused by Horner syndrome, it is helpful to interject a sudden noise just after the lights go out.
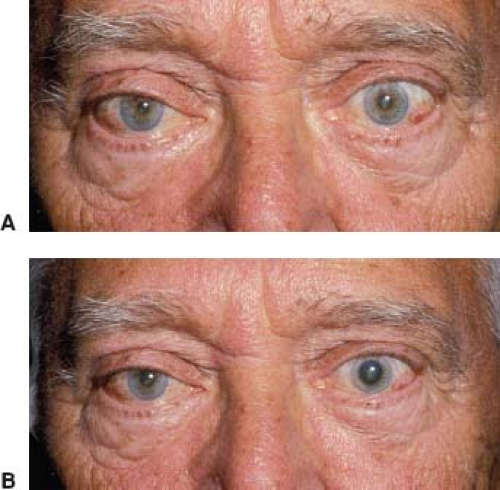 Figure 15.3 Response of Horner pupils to cocaine. A: Right Horner syndrome associated with Raeder paratrigeminal neuralgia in a 65-year-old man. B: Photo taken 45 minutes after conjunctival instillation of two drops of a 10% cocaine solution in each eye. The left pupil is dilated, whereas the right pupil remains unchanged. |
Depigmentation of the ipsilateral iris is not usually seen in patients with an acquired Horner syndrome, but it is a typical feature of congenital Horner syndrome. Nevertheless, it rarely can occur after injury to the sympathetic nervous system in adults.
Characteristic vasomotor and sudomotor changes of the facial skin occur on the affected side in some patients with Horner syndrome. The best known of these is loss of sweating (anhidrosis). In a warm environment, the skin on the affected side will feel dry, whereas the skin on the normal side will be damp. The postganglionic sympathetic sudomotor fibers for the face, after synapsing at the superior cervical ganglion, follow the external carotid artery to the face, whereas the sympathetic fibers to the eye travel via the carotid plexus of the internal carotid artery, carrying only a few sweat fibers for the skin of the forehead. Thus, anhidrosis occurs only in patients with a central or preganglionic Horner syndrome, never with a postganglionic Horner syndrome.
After acute, preganglionic sympathetic denervation, the temperature of the skin rises on the side of the lesion because of loss of vasomotor control and consequent dilation of blood vessels. Acutely, there may be some flushing and some conjunctival hyperemia, epiphora, and nasal stuffiness.
Diagnosis
It is important to differentiate a Horner syndrome from physiologic anisocoria. The diagnosis of Horner syndrome can be made by pharmacologic testing. The cocaine test remains the “gold standard” test and is based on the failure of cocaine to dilate a sympathetically denervated pupil. Cocaine blocks the reuptake of norepinephrine into the sympathetic nerve endings. In a normal eye, a 10% solution of cocaine causes dilation of the pupil, often to 8 mm or more, within about 45 minutes. However, a sufficient quantity of norepinephrine does not accumulate at the receptors of effector cells unless norepinephrine is continually being released by action potentials within the sympathetic nerves to those cells, which do not occur when there is sympathetic denervation of the pupillary dilator muscle (Fig. 15.3).
The first drop of topical cocaine stings briefly until the anesthetic effect occurs. Peak effect is attained in 40 to 60 minutes. There are no apparent psychoactive effects from a 10% solution of cocaine, but metabolites of the drug can be found in the urine in 100% of patients after 24 hours and in 50% at 36 hours.
Cocaine affects only the sympathetic system, not the parasympathetic system. If the patient is observed while seated in a lighted room, the pupils may appear not to have responded to the cocaine because the light tends to produce pupillary constriction. The patient must be brought into the examination room and the lights dimmed, at which time the pharmacologic dilation of one or both pupils can easily be appreciated.
The odds of an anisocoria being caused by an oculosympathetic palsy increase with the amount of anisocoria measured 45 minutes after the instillation of 10% cocaine into both eyes. It is not necessary to compare the before and after measurements; a post-cocaine anisocoria of 0.8 mm is sufficient to diagnose a Horner syndrome.
Testing with apraclonidine, either 0.5% or 1% solution, takes advantage of the denervation hypersensitivity of the affected pupil and results in pupillary dilation and eyelid elevation on the affected side. Unlike phenylephrine, which should dilate both pupils but may have a greater effect on the Horner syndrome eye, apraclonidine affects only the abnormal eye. Apraclonidine is a weak alpha-1 adrenergic agonist with its primary action being on alpha-2 receptors. In normal eyes, apraclonidine either has no effect on the pupil or causes slight miosis by alpha-2 stimulation and inhibition of norepinephrine release. However, both because the Horner syndrome pupil is supersensitive to alpha-1 stimulation and norepinephrine release already is minimal, the alpha-1 activity predominates and the Horner
pupil dilates. Similarly, the upper eyelid elevates slightly relative to the fellow eye (Fig. 15.4). Both anisocoria and ptosis may reverse (with the normal eye now showing miosis and a “droopy” upper eyelid) at 30 to 45 minutes after drop instillation, although in some cases observation at 60 minutes is needed to confirm the findings.
pupil dilates. Similarly, the upper eyelid elevates slightly relative to the fellow eye (Fig. 15.4). Both anisocoria and ptosis may reverse (with the normal eye now showing miosis and a “droopy” upper eyelid) at 30 to 45 minutes after drop instillation, although in some cases observation at 60 minutes is needed to confirm the findings.
 Figure 15.4 Response of Horner pupils to apraclonidine. A: Right Horner syndrome after neck trauma in a 52-year-old woman. B: Photo taken 40 minutes after topical application of 0.5% apraclonidine solution in both eyes. Note the reversal of both ptosis and anisocoria. |
Because apraclonidine is a standard ophthalmic solution and is much easier to obtain in most outpatient settings than medical cocaine, it has supplanted cocaine testing in most clinical situations. The time after onset to the appearance of supersensitivity must be taken into account when interpreting the apraclonidine test. Positive tests have been described as soon as 36 hours after a known event causing the Horner syndrome, but supersensitivity may not develop at the same rate in all patients. A negative apraclonidine test, when clinical suspicion for Horner syndrome is high, should be repeated several days later; cocaine testing 1 to 2 days later also may be considered.
Localization
Regardless of the site of the lesion in the long sympathetic pathway, all patients with Horner syndrome have a similar ptosis and miosis. It is, however, clinically important to separate the pathway into three major divisions: the central (first-order), the preganglionic (second-order), and the postganglionic (third-order) neurons.
Central Horner Syndromes. The central (first-order) neuron begins in the ipsilateral hypothalamus and extends to the ciliospinal center of Budge and Waller in the intermediolateral gray column of the spinal cord at C8–T1 (Fig. 15.5). The path may actually be polysynaptic, but it seems to stay lateral in the brainstem and cervical cord. Thus, Horner syndrome caused by damage to the central neuron is almost always unilateral. There is no pharmacologic test that identifies a central-neuron Horner syndrome; so the clinician must put localizing weight on the associated clinical signs. For example, lesions of the hypothalamus that cause an ipsilateral Horner syndrome are often associated with a contralateral hemiparesis, and some of these patients also have a contralateral hypesthesia.
Another neurologic syndrome characterized in part by a central Horner syndrome is Wallenberg syndrome. This condition, which is caused by damage to the lateral medulla, is also characterized by ipsilateral impairment of pain and temperature sensation over the face, limb ataxia, and a bulbar disturbance causing dysarthria and dysphagia. Contralaterally, pain and temperature sensation are impaired over the trunk and limbs. Lateropulsion, a compelling sensation of being pulled toward the side of the lesion, is often a prominent complaint of patients with Wallenberg syndrome and is also evident in the ocular motor findings.
The occurrence of a unilateral Horner syndrome and a contralateral trochlear nerve paresis indicates involvement either of the trochlear nucleus on the side of the Horner syndrome or of the ipsilateral fascicle before its decussation. However, not all patients with a first-order neuron Horner syndrome have other neurologic manifestations. Patients with cervical spondylosis, for example, may have no symptoms or signs of spinal cord disease. Such patients may present only with a Horner syndrome and perhaps some neck pain.
Preganglionic Horner Syndromes. The preganglionic (second-order) neuron exits from the ciliospinal center of Budge and passes across the pulmonary apex (see Fig. 15.5). It then turns upward, passes through the stellate ganglion and goes up the carotid sheath to the superior cervical ganglion, near the bifurcation of the common carotid artery.
The ptosis and miosis of a preganglionic Horner syndrome are nonspecific, but the distribution of anhidrosis is characteristic. The entire side of the head, the face, and the neck down to the clavicle are usually involved.
Malignancy is a common cause of a preganglionic Horner syndrome. The most common tumors, not surprisingly, are lung and breast cancer, but Horner syndrome is usually not an early sign of these tumors. Tumors that spread behind the carotid sheath at the C6 level may produce a preganglionic Horner syndrome associated with paralysis of the phrenic, vagus, and recurrent laryngeal nerves: the “Rowland Payne
syndrome.” Benign tumors in this region, such as schwannoma of the sympathetic chain, as well as thyroid gland enlargement as in goiter, can also produce a preganglionic Horner syndrome.
syndrome.” Benign tumors in this region, such as schwannoma of the sympathetic chain, as well as thyroid gland enlargement as in goiter, can also produce a preganglionic Horner syndrome.
 Figure 15.5 The oculosympathetic pathway. Note location of central (first-order), preganglionic (second-order), and postganglionic (third-order) neurons. (Reprinted with permission from Glaser JS. Neuro-Ophthalmology. 1st ed. Hagerstown, MD: Harper & Row; 1978:173.) |
A preganglionic Horner syndrome can be caused by accidental or surgical injury (e.g., disc herniation at C8 or T1, trauma to the brachial plexus, pneumothorax, coronary artery bypass surgery, or insertion of a pacemaker). The preganglionic neuron can also be transiently blocked by an epidural anesthetic that flows the wrong way or by an interpleural anesthetic that soaks through the pleura at the pulmonary apex to reach the stellate ganglion. Chest tubes, vascular catheters, and stray bullets can directly injure the preganglionic sympathetic nerves.
Postganglionic Horner Syndromes. The postganglionic (third-order) neuron of the sympathetic pathway to the iris dilator muscle extends from the superior cervical ganglion behind the angle of the mandible and up along the internal carotid artery, where it is called the “carotid plexus” or the “carotid nerve.” Within the cavernous sinus, the sympathetic fibers leave the internal carotid artery, join briefly with the abducens nerve, and then leave it to join the ophthalmic division of the trigeminal nerve, entering the orbit with its nasociliary branch. The sympathetic fibers in the nasociliary nerve divide into the two long ciliary nerves that travel with the lateral and medial suprachoroidal vascular bundles to reach the anterior segment of the eye and innervate the iris dilator muscle. The fibers pass through but do not synapse within the ciliary ganglion.
Lesions that affect the postganglionic third-order sympathetic neuron may be extracranial or intracranial. Extracranial lesions damage the cervical sympathetics in the neck, whereas intracranial lesions damage the sympathetic chain at the base of the skull,
in the carotid canal and middle ear, or in the region of the cavernous sinus. It is very unusual for an orbital lesion to produce an isolated Horner syndrome.
in the carotid canal and middle ear, or in the region of the cavernous sinus. It is very unusual for an orbital lesion to produce an isolated Horner syndrome.
Lesions of or along the internal carotid artery are a common cause of a postganglionic Horner syndrome. Both traumatic and spontaneous dissections of the internal carotid artery can produce sudden ipsilateral face and neck pain associated with a postganglionic Horner syndrome. Raeder paratrigeminal neuralgia, the name given to a headache syndrome characterized by persistent trigeminal pain associated with a postganglionic Horner syndrome, likely represents unrecognized carotid dissection in many patients.
A postganglionic Horner syndrome may be caused by tumors, inflammatory lesions, and other masses in the neck. Any neoplasm that extends or metastasizes to the cervical lymph nodes may also damage the cervical sympathetic chain. A postganglionic Horner syndrome, paralysis of the tongue, anesthesia of the pharynx, and dysphagia, all on the same side, may indicate a tumor of the nasopharynx or jugular foramen.
Tumors, aneurysms, infections, and other lesions in the cavernous sinus may produce a postganglionic Horner syndrome. In many of these cases, there is associated ipsilateral ophthalmoplegia as well as pain or dysesthesia of the ipsilateral side of the face caused by involvement of one or more ocular motor nerves and the trigeminal nerve within the sinus. Because the abducens nerve and oculosympathetic nerves are briefly joined in the cavernous sinus, an abducens palsy and a postganglionic Horner syndrome occurring together without other neurologic signs should immediately suggest a cavernous sinus lesion.
Cluster headache manifests as intense, unilateral lancinating or dysesthetic pain, usually lasts 30 to 120 minutes, and often occurs at night. Affected patients often have an associated sympathetic palsy, and there is ipsilateral nasal stuffiness. Typically, the Horner syndrome persists after the headache resolves. Other ischemic conditions, such as giant cell arteritis, can cause a postganglionic Horner syndrome.
A middle fossa mass encroaching on Meckel cave and on the internal carotid artery at the foramen lacerum can also produce a postganglionic Horner syndrome associated with pain. Other lesions at the base of the skull, including a basal skull fracture, can produce a similar clinical picture.
 Figure 15.6 Response of Horner pupils to hydroxyamphetamine. A: Left Horner syndrome in a 55-year-old man with an apical lung tumor. B: At 45 minutes after conjunctival instillation of two drops of 1% hydroxyamphetamine solution in each eye, both pupils are dilated, indicating an intact postganglionic neuron (i.e., a preganglionic Horner syndrome). |
Differentiating Localizations
The hydroxyamphetamine test can be used to differentiate between a postganglionic and a preganglionic or central Horner syndrome (Fig. 15.6). This test should be performed only after a cocaine or apraclonidine test has established the diagnosis of a Horner syndrome or in a setting in which the diagnosis of Horner syndrome is not in doubt. The hydroxyamphetamine test should not be performed for 24 to 48 hours after ether cocaine or apraclonidine testing, to allow the corneas and pupils to recover from the effects of the drug. The hydroxyamphetamine test is performed by placing two drops of hydroxyamphetamine hydrobromide 1% (Paredrine) in the lower cul-de-sac of each eye, and the pupils are assessed in a dim light about 45 minutes later. Hydroxyamphetamine releases stored norepinephrine from the adrenergic nerve ending, producing variable but usually significant mydriasis in normal subjects.
When the lesion causing a Horner syndrome is in the postganglionic neuron, the nerve endings themselves are destroyed, there are no stores of norepinephrine to release, and hydroxyamphetamine thus has no mydriatic effect. If the lesion is in the preganglionic or central neuron, the pupil will dilate fully and may even become larger than the opposite pupil, presumably because of upregulation of the postsynaptic receptors on the dilator muscle. False-negative results may occur within the first week after the Horner syndrome has developed, before the stores of norepinephrine at the presynaptic terminals have been depleted. Thus, a smaller pupil that fails to dilate to cocaine and/or enlarges with apraclonidine and subsequently does not dilate after topical administration of hydroxyamphetamine or a similar substance is likely to be caused by a lesion of the postganglionic sympathetic neuron.
When the lesion causing a Horner syndrome is in the postganglionic neuron, the nerve endings themselves are destroyed, there are no stores of norepinephrine to release, and hydroxyamphetamine thus has no mydriatic effect. If the lesion is in the preganglionic or central neuron, the pupil will dilate fully and may even become larger than the opposite pupil, presumably because of upregulation of the postsynaptic receptors on the dilator muscle. False-negative results may occur within the first week after the Horner syndrome has developed, before the stores of norepinephrine at the presynaptic terminals have been depleted. Thus, a smaller pupil that fails to dilate to cocaine and/or enlarges with apraclonidine and subsequently does not dilate after topical administration of hydroxyamphetamine or a similar substance is likely to be caused by a lesion of the postganglionic sympathetic neuron.
 Figure 15.7 Horner syndrome (top) associated with injury of the right brachial plexus at birth. Note the underdeveloped right arm and forearm (bottom). |
Acquired Horner Syndrome in Children
While an acquired Horner syndrome in childhood is sometimes associated with neoplasia, including spinal cord tumors, embryonal cell carcinoma, neuroblastoma, and rhabdomyosarcoma, this association is quite rare. A Horner syndrome in childhood is usually not associated with a tumor and is often an isolated finding of no significance. Other causes of an acquired Horner syndrome in childhood include traumatic brachial plexus palsy, intrathoracic aneurysm, and thrombosis of the internal carotid artery. If old photographs clearly indicate that a Horner syndrome in a child is acquired, it is recommended to begin further evaluation with CT scanning or MRI of the chest.
Congenital Horner Syndrome
Congenital Horner syndrome is an uncommon disorder. In its fully developed form, the syndrome consists of ptosis, miosis, facial anhidrosis, and hypochromia of the affected iris. Injury to the brachial plexus at birth is responsible for many of these cases (Fig. 15.7), but some cases occur in association with congenital tumors, and others occur after viral infections.
Most patients with congenital Horner syndrome can be separated into one of three groups: patients with evidence of obstetric trauma to the internal carotid artery sympathetic plexus, patients without a history of birth trauma but with a lesion that is clinically and pharmacologically localized to the superior cervical ganglion, and those with evidence of surgical or obstetric injury to the preganglionic sympathetic pathway.
The first group of patients tends to have had substantial perinatal head trauma as a result of difficult forceps deliveries. Clinically, such patients have obvious ptosis and miosis with generally intact facial sweating. Pharmacologic testing is consistent with a postganglionic lesion.
In the second group of patients, pharmacologic testing also is consistent with a postganglionic lesion but such patients have facial anhidrosis, indicating a lesion proximal to the separation of the sudomotor fibers with the external carotid artery. The causes of such a lesion could include an embryopathy directly involving the superior cervical ganglion, damage to the vascular supply of the superior cervical ganglion, or transsynaptic dysgenesis of the superior cervical ganglion following a defect located more proximally in the sympathetic pathway.
The third group of patients has suffered trauma to the preganglionic oculosympathetic pathway. Injuries include trauma to the brachial plexus and surgery in the thoracic region. Although patients in this group should have a preganglionic Horner syndrome, some have pharmacologic testing consistent with a postganglionic lesion, presumably indicating transsynaptic degeneration occurring in the postganglionic neuron following preganglionic injury (Fig 15.8A).
 Figure 15.8 Facial coloration changes in Horner syndrome patients. A: Lack of facial flushing and sweating due to transsynaptic degeneration of sympathetic fibers in a patient who underwent extensive resection of a right cavernous sinus tumor. She also had complete ptosis and ophthalmoplegia from damage to cranial nerves 3, 4, and 6. B: Atropinic flushing in a child with a congenital left Horner syndrome. Note that the atropinic flush is present only on the side of the face opposite the Horner syndrome. |
Parents of infants with congenital Horner syndrome sometimes report that the baby develops a hemifacial flush when it is nursing or crying. It is likely that the hemifacial flushing seen in infants is on the side opposite the Horner syndrome and is simply the normal response, which appears more obvious because of the impaired facial vasodilation on the side of a congenital Horner syndrome.
When a child has unilateral ptosis and ipsilateral miosis, and there is doubt as to whether or not a sympathetic defect is present, a cycloplegic refraction can sometimes unexpectedly answer the question by producing an atropinic flush. This reaction only occurs when there is an intact sympathetic innervation to the skin and thus is absent on the side of the Horner syndrome (Fig. 15.8B).
A child with Horner syndrome and very blue eyes will not develop visible iris heterochromia, but most children with Horner syndrome have paler iris on the affected side. This occurs whether the lesion is preganglionic or postganglionic because of anterograde transsynaptic dysgenesis. When the sympathetic pathway is interrupted in the preganglionic neuron, the next distal ganglion—the superior cervical ganglion—does not develop normally. There are fewer cells in the ganglion and less norepinephrine stores to release with hydroxyamphetamine. This results in impaired development of iris melanophores, causing hypochromia of the iris stroma.
Pharmacological testing in children under age 2 should be approached cautiously, as systemic absorption of cocaine may increase blood pressure or heart rate, and apraclonidine crosses the blood–brain barrier in this age group and can produce CNS depression.
Sympathetic Hyperactivity
Sympathetic hyperactivity occurs in a number of settings in which the pupils are affected. In such cases, there may be anisocoria that is more obvious in darkness than in light.
A tadpole pupil is an intermittent and benign phenomenon in which the pupil of one eye becomes distorted for a minute or two. The pupil is pulled in one direction like the tail of a tadpole. It may be caused by repeated bursts of sympathetic innervation, an irritation that eventually causes loss of fibers and a Horner syndrome. This condition is distinct from the episodic unilateral mydriasis that occurs in some young patients during a typical migraine attack, although there is some similarity.
Some patients who sustain trauma to the low cervical or high thoracic spinal cord experience episodes of unilateral pupillary dilation associated with unilateral sweating; this syndrome was described in the early eighteenth century by the French military surgeon Francois Pourfour du Petit and bears his name. Pharmacologic testing in such patients suggests that the mydriasis is caused by episodic sympathetic irritation.
Pharmacologic Stimulation of the Iris Sphincter
Almost all cases of acute anisocoria in which one pupil is nonreactive are caused by pharmacologic blockade of the iris sphincter muscle. In such cases, the
anisocoria is worse in light than in darkness because the affected pupil cannot constrict. In rare instances, however, a pharmacologic agent, such as an organophosphate used in pesticides, may produce anisocoria by stimulating rather than blocking the parasympathetic system, thus producing a nonreactive, miotic pupil. In such cases and in other cases of pharmacologic stimulation of the ocular parasympathetic pathway, a 1% solution of tropicamide will dilate the larger, reactive pupil but will fail to dilate the small, nonreactive pupil.
anisocoria is worse in light than in darkness because the affected pupil cannot constrict. In rare instances, however, a pharmacologic agent, such as an organophosphate used in pesticides, may produce anisocoria by stimulating rather than blocking the parasympathetic system, thus producing a nonreactive, miotic pupil. In such cases and in other cases of pharmacologic stimulation of the ocular parasympathetic pathway, a 1% solution of tropicamide will dilate the larger, reactive pupil but will fail to dilate the small, nonreactive pupil.
Pharmacologic Stimulation of the Iris Dilator
Topical cocaine placed in the nose for medical or for other reasons can back up the lacrimal duct into the conjunctival sac. Most eye-whitening drops that contain sympathomimetic components are too weak to dilate the pupil, but if the cornea is abraded (e.g., by a contact lens), enough of the oxymetazoline or the phenylephrine may get into the aqueous humor to dilate the pupil. Other adrenergic drugs given in a mist for pulmonary therapy may escape around the edge of the face mask and condense in the conjunctival sac, causing pupillary dilation that is more evident in darkness than in light.
More Anisocoria in Light
Damage to the Parasympathetic Outflow to the Iris Sphincter Muscle
The final common pathway for pupillary reactivity to light and near stimulation begins in the mesencephalon with the visceral oculomotor nuclei, continues via the oculomotor nerve to the ciliary ganglion, and reaches the iris sphincter through the short ciliary nerves. Lesions that affect this parasympathetic pathway can produce absolute paralysis of pupillary constriction. The pupil is then dilated and nonreactive, and all constrictor reflexes are absent. In many cases, all parasympathetic input to the eye is damaged simultaneously so that accommodation is also lost. This combination of iridoplegia and cycloplegia is often called internal ophthalmoplegia to distinguish it from the external ophthalmoplegia that occurs when the extraocular muscles are paralyzed in the setting of normal pupillary responses.
Topical diagnosis of paralysis of the iris sphincter is simplified when signs of an oculomotor nerve palsy are present. In the setting of ptosis and paralysis of the superior, inferior, and medial rectus muscles, as well as the inferior oblique muscle, a nonreactive, dilated pupil is but a part of the classic picture of a lesion of the oculomotor nerve. This chapter provides a brief overview of oculomotor nerve disease causing anisocoria. For additional considerations and details, please see Chapter 18. However, isolated iris paralysis can be a difficult diagnostic problem. One must consider lesions of the mesencephalon, the oculomotor nerve, the ciliary ganglion, the short ciliary nerves, and the eye itself.
Damage to the Edinger–Westphal Nuclei
Lesions of the rostral mesencephalon almost never produce an isolated unilateral, nonreactive, dilated pupil. When there is isolated damage to the Edinger–Westphal nuclei, bilateral pupillary abnormalities are the rule. In addition, most lesions in this region that produce pupillary abnormalities also affect other parts of the oculomotor nucleus, causing ptosis, ophthalmoparesis, or both.
Damage to Pupillomotor Fibers in the Oculomotor Nerve
Because the fibers emerging from the Edinger–Westphal nucleus are among the most rostral in the oculomotor group (Fig. 15.9




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
