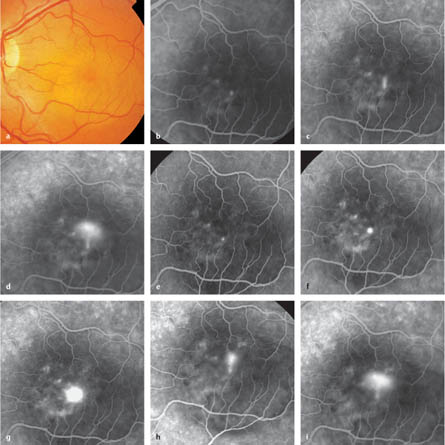
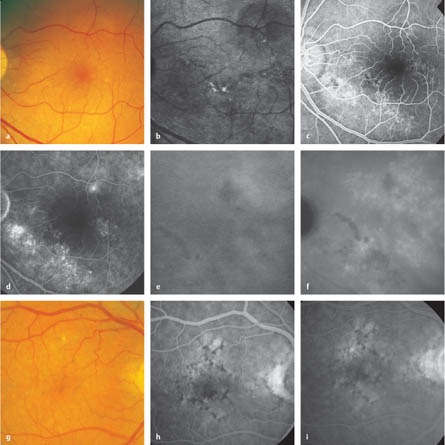
8.1 Central Serous Chorioretinopathy – Classic central serous chorioretinopathy, with one or more areas of focal leakage. – Diffuse pigment epitheliopathy (chronic central serous chorioretinopathy; see section 8.2). Piccolino FC, Borgia L, Zinicola E, Zingirian M. Indocyanine green angiographic findings in central serous chorioretinopathy. Eye 1995; 9:324–32. Robertson DM. Argon laser photocoagulation treatment in central serous chorioretinopathy. Ophthalmology 1986;93:972–4. Yamada K, Hayasaka S, Setogawa T. Fluorescein-angiographic patterns in patients with central serous chorioretinopathy at the initial visit. Ophthalmologica 1992;205:69–76. Fig. 8.1a–i Central serous chorioretinopathy a Color photograph. Acute central serous chorioretinopathy, with a slightly yellow central neurosensory detachment. b Early arteriovenous phase. Blocked fluorescence caused by the exudate inside the detachment; an irregular hyperfluorescent surface with three hyperfluorescent points can be seen inside. c Late arteriovenous phase. One of these leaking points expands upward, creating a smokestack appearance. d Late phase. The leakage continues expanding upward and starts to occupy the hollow space in the neurosensory detachment. e Early arteriovenous phase. The same patient, 3 months later. No significant difference is recognizable in the early arteriovenous phase in comparison with the initial examination. f Late arteriovenous phase. The smokestack is no longer visible, but there is a flat expansion of the hyperfluorescence from the source point (the “expanding pinpoint” appearance). g Late phase. Further radial expansion of the hyperfluorescence, but no umbrella pattern. h Late arteriovenous phase. The same patient, another 3 months later. No significant differences from the angiography carried out at the first visit are evident. i Late phase. The same smokestack appearance as at the first visit, with increasing neurosensory detachment. This patient therefore has different angiographic signs during acute central serous chorioretinopathy. Cohen D, Gaudric A, Coscas G, Quentel G, Binaghi M. [Diffuse retinal epitheliopathy and central serous chorioretinopathy; in French.] J Fr Ophtalmol 1983;6:339–49. Iide T, Yannuzzi LA, Spaide RF, et al. Chronic central serous chorioretinopathy. Retina 2003;23:1–7. Lafaut BA, Salati C, Priem H, De Laey JJ. Indocyanine green angiography is of value for the diagnosis of chronic central serous chorioretinopathy in elderly patients. Graefes Arch Clin Exp Ophthalmol 1998;236:513–21. Levine R, Brucker AJ, Robinson F. Long-term follow-up of idiopathic central serous chorioretinopathy by fluorescein angiography. Ophthalmology 1989;96:854–9. Spaide RF, Campeas L, Haas A, et al. Central serous chorioretinopathy in younger and older adults. Ophthalmology 1996;103:2070–80. Yannuzzi LA, Slakter JS, Kaufman SR, Gupta K. Laser treatment of diffuse retinal pigment epitheliopathy. Eur J Ophthalmol 1992;2: 103–14. Fig. 8.2a–i Chronic central serous chorioretinopathy a Color photograph. Chronic and acute central serous chorioretinopathy, with no foveal reflex and detachment of the neurosensory retina extrafoveal at the 2-o’clock position. b Infrared image. Confocal infrared ophthalmoscopy with the scanning laser ophthalmoscope accentuates a flat detachment of the neurosensory retina along the temporal lower vessel arcade, as well as an acute detachment at the 2-o’clock position, shown as a dark area. c Arteriovenous phase. Detachment of the neurosensory retina at the 2-o’clock position and defects in the retinal pigment epithelium along the temporal lower vessel arcade. d Late phase. There is a point with strong leakage at the 2-o’clock position (acute central serous chorioretinopathy) and diffuse, moderate leakage in the area with retinal pigment epithelium defects at the temporal lower vessel arcade (chronic central serous chorioretinopathy). e Indocyanine green angiography, at 10 min. Hyperfluorescence and initial leakage in the area of the acute and chronic central serous chorioretinopathy can be seen. f Indocyanine green angiography, at 30 min. There is expansion of the Indocyanine green central hyperfluorescence as well as at the 2-o’clock position. g Color photograph in a patient with an occult choroidal neovascularization. A mixed image of atrophies and pigment clumping can be seen. Retinal edema can be confirmed using optical coherence tomography. h Arteriovenous phase. Hypofluorescent and hyperfluorescent areas that match the fundus findings. i Late phase. There is mild diffuse and localized leakage in the temporal area above the fovea.
Epidemiology, Pathophysiology, and Clinical Presentation
 Central serous chorioretinopathy can be described as neurosensory detachment resulting from idiopathic pigment epithelial leakage and can be divided into two basic types:
Central serous chorioretinopathy can be described as neurosensory detachment resulting from idiopathic pigment epithelial leakage and can be divided into two basic types:
 The term most often used for this disease in the German-language literature is “retinitis centralis serosa,” which dates back to the era of Albrecht von Graefe. The disease is more commonly known as “idiopathic central serous chorioretinopathy” (ICSC). The term “central serous retinopathy” (CSR) is also often used.
The term most often used for this disease in the German-language literature is “retinitis centralis serosa,” which dates back to the era of Albrecht von Graefe. The disease is more commonly known as “idiopathic central serous chorioretinopathy” (ICSC). The term “central serous retinopathy” (CSR) is also often used.
 In most cases, the etiology remains unclear; these cases are therefore classified as idiopathic central serous chorioretinopathy. Pathogenetically, a localized permeability dysfunction of the choroid is suspected. Secondary central serous chorioretinopathy can be observed during pregnancy, in patients receiving systemic steroids (including occasional inhalation), after organ transplantation, and in patients with glomerulonephritis, Crohn disease, or choroidal folds.
In most cases, the etiology remains unclear; these cases are therefore classified as idiopathic central serous chorioretinopathy. Pathogenetically, a localized permeability dysfunction of the choroid is suspected. Secondary central serous chorioretinopathy can be observed during pregnancy, in patients receiving systemic steroids (including occasional inhalation), after organ transplantation, and in patients with glomerulonephritis, Crohn disease, or choroidal folds.
 The disease predominantly affects patients between the ages of 20 and 50, and mainly presents unilaterally. The proportion of men to women is 2.7: 1; 60–90% present with acute central serous chorioretinopathy and 5–40% present with chronic central serous retinopathy.
The disease predominantly affects patients between the ages of 20 and 50, and mainly presents unilaterally. The proportion of men to women is 2.7: 1; 60–90% present with acute central serous chorioretinopathy and 5–40% present with chronic central serous retinopathy.
 The most common symptoms of the disease are a deterioration in visual acuity, micropsia, metamorphopsia, reduced dark adaptation, color vision deficiencies, and a brownish spot in the central field of vision.
The most common symptoms of the disease are a deterioration in visual acuity, micropsia, metamorphopsia, reduced dark adaptation, color vision deficiencies, and a brownish spot in the central field of vision.
 Clinically, neurosensory detachments in the foveal area without pigment epithelial detachments can be observed, with multiple leakages in up to 30% of patients. Patients with central pigment epithelial detachment are rare, and those with a bullous form are very rare.
Clinically, neurosensory detachments in the foveal area without pigment epithelial detachments can be observed, with multiple leakages in up to 30% of patients. Patients with central pigment epithelial detachment are rare, and those with a bullous form are very rare.
 Recurrences may develop in about 30% of patients during the course of the disease, and can even occur three or more times in approximately 10% of patients.
Recurrences may develop in about 30% of patients during the course of the disease, and can even occur three or more times in approximately 10% of patients.
Fluorescein and Indocyanine Green Angiography
 An umbrella or “smokestack” pattern can be seen in approximately a quarter of the cases, starting with a small hyperfluorescent spot in the arteriovenous phase, with leakage that continues upward in the course of the angiography and then spreads downward along the neurosensory detachment borders.
An umbrella or “smokestack” pattern can be seen in approximately a quarter of the cases, starting with a small hyperfluorescent spot in the arteriovenous phase, with leakage that continues upward in the course of the angiography and then spreads downward along the neurosensory detachment borders.
 In approximately 60% of cases, what is known as an “expanding pinpoint” can be identified as a hyper-fluorescent spot in the early phase, which enlarges in all directions simultaneously afterward.
In approximately 60% of cases, what is known as an “expanding pinpoint” can be identified as a hyper-fluorescent spot in the early phase, which enlarges in all directions simultaneously afterward.
 A spot with a minimally increasing hyperfluorescent area can be found in approximately 15% of cases.
A spot with a minimally increasing hyperfluorescent area can be found in approximately 15% of cases.
 One spot is seen in most cases, but two or more hyper-fluorescent spots with leakage can be found in up to approximately 30%.
One spot is seen in most cases, but two or more hyper-fluorescent spots with leakage can be found in up to approximately 30%.
 Indocyanine green angiography reveals hyperfluorescent, expanding areas, which are also usually visible in the unaffected areas and can often be detected in the fellow eye.
Indocyanine green angiography reveals hyperfluorescent, expanding areas, which are also usually visible in the unaffected areas and can often be detected in the fellow eye.
Diagnosis and Treatment
 The diagnosis is based on typical symptoms and ophthalmoscopy, which reveals a nearly round central neurosensory detachment with transparent serous subretinal fluid and no evidence of choroidal neovascularization. The diagnosis is established by fluorescein angiography.
The diagnosis is based on typical symptoms and ophthalmoscopy, which reveals a nearly round central neurosensory detachment with transparent serous subretinal fluid and no evidence of choroidal neovascularization. The diagnosis is established by fluorescein angiography.
 The prognosis is generally good, especially if the initial visual acuity is 0.5 or better (95% of patients achieve visual acuity of more than 0.63). The recovery period averages approximately 4 months. Healing usually leads to defects in the retinal pigment epithelium and can leave persistent metamorphopsia.
The prognosis is generally good, especially if the initial visual acuity is 0.5 or better (95% of patients achieve visual acuity of more than 0.63). The recovery period averages approximately 4 months. Healing usually leads to defects in the retinal pigment epithelium and can leave persistent metamorphopsia.
 Important, and occasionally difficult, differential diagnoses are: idiopathic choroidal neovascularization, neurosensory detachment associated with optic pit, polypoidal choroidal vasculopathy, and retinal telangiectasia. With stereo angiography, telangiectases only show leakages in the retinal layers.
Important, and occasionally difficult, differential diagnoses are: idiopathic choroidal neovascularization, neurosensory detachment associated with optic pit, polypoidal choroidal vasculopathy, and retinal telangiectasia. With stereo angiography, telangiectases only show leakages in the retinal layers.
 The most widely advocated treatment method at present is localized laser coagulation of the original pigment epithelial defect. There have as yet been no controlled prospective studies.
The most widely advocated treatment method at present is localized laser coagulation of the original pigment epithelial defect. There have as yet been no controlled prospective studies.
 The majority of published papers state that laser coagulation reduces the duration of the illness, but it does not improve the final visual acuity in comparison with untreated eyes. The complication rate (with the development of choroidal neovascularization resulting from laser treatment) is 1–5%. As spontaneous resolution takes 3–5 months on average, most authors only recommend laser photocoagulation for patients with persistent leakage and symptoms that have persisted for 6 months or longer.
The majority of published papers state that laser coagulation reduces the duration of the illness, but it does not improve the final visual acuity in comparison with untreated eyes. The complication rate (with the development of choroidal neovascularization resulting from laser treatment) is 1–5%. As spontaneous resolution takes 3–5 months on average, most authors only recommend laser photocoagulation for patients with persistent leakage and symptoms that have persisted for 6 months or longer.
 Some authors state that systemic acetazolamide therapy can shorten the recovery period in acute central serous retinopathy, but this treatment apparently has no influence on the final visual acuity.
Some authors state that systemic acetazolamide therapy can shorten the recovery period in acute central serous retinopathy, but this treatment apparently has no influence on the final visual acuity.
 Systemic corticosteroid therapy is contraindicated.
Systemic corticosteroid therapy is contraindicated.
References
8.2 Chronic Central Serous Chorioretinopathy
Epidemiology, Pathophysiology, and Clinical Presentation
 In the English-language literature, chronic central serous chorioretinopathy is also known as diffuse retinal pigment epitheliopathy after its most obvious characteristic. Typically, diffuse areas of atrophy of the retinal pigment epithelium can be seen, with flat neurosensory detachments and pigment epithelial detachments. The course of the disease is chronic, and regular deterioration is common.
In the English-language literature, chronic central serous chorioretinopathy is also known as diffuse retinal pigment epitheliopathy after its most obvious characteristic. Typically, diffuse areas of atrophy of the retinal pigment epithelium can be seen, with flat neurosensory detachments and pigment epithelial detachments. The course of the disease is chronic, and regular deterioration is common.
 Overall, the clinical picture is similar to that in acute central serous retinopathy, but the patients are mostly older (over 50), have distinct areas of atrophy of the retinal pigment epithelium with visual field defects (70%), and often suffer bilateral involvement (90%). In comparison with acute central serous chorioretinopathy, choroidal neovascularizations (CNV) develop in a larger proportion of the patients.
Overall, the clinical picture is similar to that in acute central serous retinopathy, but the patients are mostly older (over 50), have distinct areas of atrophy of the retinal pigment epithelium with visual field defects (70%), and often suffer bilateral involvement (90%). In comparison with acute central serous chorioretinopathy, choroidal neovascularizations (CNV) develop in a larger proportion of the patients.
 The disease can either develop independently, or from recurrences of acute central serous chorioretinopathy.
The disease can either develop independently, or from recurrences of acute central serous chorioretinopathy.
 Retinal edema can sometimes be detected in the affected areas.
Retinal edema can sometimes be detected in the affected areas.
Fluorescein Angiography
 Small pinpoint-like leakages within a pigment epithelial atrophy are typical; they are frequently in a peripapillary location, are chronic and recurrent, and lack the strong leakage that can be seen in leakage areas associated with acute central serous retinopathy.
Small pinpoint-like leakages within a pigment epithelial atrophy are typical; they are frequently in a peripapillary location, are chronic and recurrent, and lack the strong leakage that can be seen in leakage areas associated with acute central serous retinopathy.
 Nonleaking defects in the retinal pigment epithelium almost always form in the area of earlier detachment of the neurosensory retina.
Nonleaking defects in the retinal pigment epithelium almost always form in the area of earlier detachment of the neurosensory retina.
Indocyanine Green Angiography
 Indocyanine green angiography shows areas of diffuse leakage, with dispersion during the 30-minute late phase, which are similar to those in central serous chorioretinopathy but considerably more pronounced.
Indocyanine green angiography shows areas of diffuse leakage, with dispersion during the 30-minute late phase, which are similar to those in central serous chorioretinopathy but considerably more pronounced.
Diagnosis and Treatment
 A long-term disease course, with phases of clinical improvement and deterioration, is typical.
A long-term disease course, with phases of clinical improvement and deterioration, is typical.
 The differential diagnosis from occult CNV in age-related macular degeneration is often difficult. Follow-up is therefore necessary before the diagnosis is conclusively established, with the help of indocyanine green angiography if necessary. Hemorrhages—a classic aspect of CNVs—expansion of the lesion, and retinal edema, argue against the existence of chronic central serous retinopathy alone.
The differential diagnosis from occult CNV in age-related macular degeneration is often difficult. Follow-up is therefore necessary before the diagnosis is conclusively established, with the help of indocyanine green angiography if necessary. Hemorrhages—a classic aspect of CNVs—expansion of the lesion, and retinal edema, argue against the existence of chronic central serous retinopathy alone.
 To prevent further secondary damage as a result of detachment (visual field defects, damage or atrophy of the retinal pigment epithelium, loss of vision), some authors recommend grid laser coagulation in the area of diffuse leakage.
To prevent further secondary damage as a result of detachment (visual field defects, damage or atrophy of the retinal pigment epithelium, loss of vision), some authors recommend grid laser coagulation in the area of diffuse leakage.
References
8.3 Macular Pucker
Epidemiology, Pathophysiology, and Clinical Presentation
 The epiretinal development of gliosis in the macula, with distortion of the retina and resulting dysfunction, is known as idiopathic epiretinal gliosis (when a peripheral retina hole is not detectable) or macular pucker (when gliosis is secondary to formation of a retinal break or retinal detachment). The distinction between these two groups is vague, since in idiopathic epiretinal gliosis, small peripheral holes (which are clinically not always diagnosable) can often be found in postmortem examinations.
The epiretinal development of gliosis in the macula, with distortion of the retina and resulting dysfunction, is known as idiopathic epiretinal gliosis (when a peripheral retina hole is not detectable) or macular pucker (when gliosis is secondary to formation of a retinal break or retinal detachment). The distinction between these two groups is vague, since in idiopathic epiretinal gliosis, small peripheral holes (which are clinically not always diagnosable) can often be found in postmortem examinations.
 In addition to the idiopathic group and classic macular pucker, epimacular membranes can also develop after other vitreoretinal diseases or therapy (branch retinal vein occlusion, uveitis, laser coagulation, and ocular tumor therapy).
In addition to the idiopathic group and classic macular pucker, epimacular membranes can also develop after other vitreoretinal diseases or therapy (branch retinal vein occlusion, uveitis, laser coagulation, and ocular tumor therapy).
 In practice, the term “macular pucker” has emerged as the generic term for these three types of epiretinal gliosis.
In practice, the term “macular pucker” has emerged as the generic term for these three types of epiretinal gliosis.
 Histologically, the membranes consist of collagens, partly from internal limiting membranes, retinal pigment epithelial cells, astrocytes, fibrocytes, and macrophages.
Histologically, the membranes consist of collagens, partly from internal limiting membranes, retinal pigment epithelial cells, astrocytes, fibrocytes, and macrophages.
 The retinal vessels can become irregularly distorted by the epiretinal membrane resulting in edema. The membrane can overgrow the fovea, resulting in increased macular thickness without cysts and without foveal depression, or can create a macular full-thickness hole by tangential traction of the epiretinal membrane.
The retinal vessels can become irregularly distorted by the epiretinal membrane resulting in edema. The membrane can overgrow the fovea, resulting in increased macular thickness without cysts and without foveal depression, or can create a macular full-thickness hole by tangential traction of the epiretinal membrane.
 The prevalence is 6% in patients over the age of 50; the disease is bilateral in 20–30% of cases.
The prevalence is 6% in patients over the age of 50; the disease is bilateral in 20–30% of cases.
 The patient usually notices a decrease in visual acuity with metamorphopsia within a few weeks, followed by a period of relative stability or only a slow deterioration in visual acuity. Only about 1% of patients with macular pucker experience spontaneous separation of the membrane from the macula. Visual acuity deteriorates rapidly if a macular hole develops as a result of the pucker.
The patient usually notices a decrease in visual acuity with metamorphopsia within a few weeks, followed by a period of relative stability or only a slow deterioration in visual acuity. Only about 1% of patients with macular pucker experience spontaneous separation of the membrane from the macula. Visual acuity deteriorates rapidly if a macular hole develops as a result of the pucker.
Fluorescein Angiography
 On angiography, the typical, sometimes corkscrew-shaped vessels are easier to identify as a result of improved contrast. In most cases, only moderately diffuse leakages can be detected in areas of disturbed vessels without the development of retinal cysts.
On angiography, the typical, sometimes corkscrew-shaped vessels are easier to identify as a result of improved contrast. In most cases, only moderately diffuse leakages can be detected in areas of disturbed vessels without the development of retinal cysts.
 Slight blurring above the distorted vessels may also result from thick epiretinal membranes.
Slight blurring above the distorted vessels may also result from thick epiretinal membranes.
 The diagnosis of a macular pucker is usually based on the clinical findings, without the assistance of angiography. However, in case of doubt, angiography is helpful for determining and identifying other causes (choroidal neovascularizations, telangiectasia, branch retinal vein occlusion).
The diagnosis of a macular pucker is usually based on the clinical findings, without the assistance of angiography. However, in case of doubt, angiography is helpful for determining and identifying other causes (choroidal neovascularizations, telangiectasia, branch retinal vein occlusion).
 The extent of the leakage visible on angiography has no prognostic significance in relation to the expected postoperative results.
The extent of the leakage visible on angiography has no prognostic significance in relation to the expected postoperative results.
Diagnosis and Treatment
 The flat, glistening reflection of the gliosis is usually visible on ophthalmoscopy, particularly with the red-free light on the slitlamp. Additional signs include distortions of the vessels, puckering of the internal limiting membrane and absence of the fovea reflex, pseudo-holes, or the development of a macular hole resulting from the puckering.
The flat, glistening reflection of the gliosis is usually visible on ophthalmoscopy, particularly with the red-free light on the slitlamp. Additional signs include distortions of the vessels, puckering of the internal limiting membrane and absence of the fovea reflex, pseudo-holes, or the development of a macular hole resulting from the puckering.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


