Purpose
To examine the time burden of managing neovascular age-related macular degeneration (AMD) imposed on physicians, staff, patients, and caregivers.
Design
Mixed-methods, prospective, observational time-and-motion study.
Methods
The multicenter study was conducted from March 2011 through August 2012. Retina specialists administering ≥50 vascular endothelial growth factor (VEGF)–inhibitor injections monthly were surveyed and completed records for ≥5 patients scheduled for office visits within 3 weeks for anti-VEGF injection or monitoring. A survey was administered to 75 neovascular AMD patients aged ≥50 years who received ≥1 anti-VEGF injection in the past 6 months. Telephone interviews were conducted with 13 neovascular AMD patient caregivers.
Results
Fifty-six physicians provided data for 221 patients with neovascular AMD. Patients accounted for 20% of the health care staff’s time per week, with an average of 23 staff members. An average patient visit for neovascular AMD was 90 minutes (range: 13 minutes to >4 hours). Patients reported an average time per visit of almost 12 hours, including preappointment preparation (16 minutes), travel (66 minutes), waiting time (37 minutes), treatment time (43 minutes), and postappointment recovery (9 hours). Patients stated that caregivers took time away from work (22%) and personal activities (28%) to provide transportation to appointments.
Conclusions
Neovascular AMD management imposes a substantial time burden on physicians, staff, patients, and caregivers. There may be a need for additional support and/or reimbursement for services required by patients and caregivers and provided by physicians.
Neovascular age-related macular degeneration (AMD) is a debilitating, progressive disease that has a profound impact on patients’ visual acuity and overall visual function. It is the third-leading cause of blindness worldwide, after cataracts and glaucoma, and the leading cause of blindness in industrialized countries. It is estimated that 1.75 million individuals aged ≥40 years in the United States (US) (prevalence 1.47%; 95% confidence interval [CI] 1.38–1.55) have advanced AMD, and an estimated 1.22 million (prevalence 1.02%; 95% CI 0.93–1.11) patients have neovascular AMD in at least 1 eye; these numbers are expected to increase with the aging population. As visual impairment progresses, independence and overall quality of life decline in parallel. As visual function declines, the negative impact on activities of daily living substantially increases. This has been shown to have a detrimental impact on cognitive functioning, with 1 in 7 patients with AMD showing cognitive decline. Patients with AMD have also shown an increased risk of depression compared with patients without AMD.
As many as one-third of patients with AMD require caregiving services owing to their AMD. As AMD progresses, these indirect costs for caregiver services form a greater proportion of total costs, and caregiver burden can be substantial.
AMD also results in substantial economic impact in terms of direct health care costs. Costs also increase in direct proportion to disease progression. Patients with AMD require more services (eg, rehabilitation, counseling), devices, and supplements (eg, approximately two-thirds of patients took vitamins with lutein) than patients without AMD. Patients with neovascular AMD incurred twice the annual costs per patient compared to individuals without AMD (2011 US$: $34 308 vs $17 473), based on a cohort of 241 patients. Physicians must attempt to continually improve patient outcomes in the face of more stringent budgetary constraints, and health care decision makers (ie, physicians and payers) struggle to balance quality of care with costs of care and reimbursement for time and services provided.
The current mainstay of treatment for neovascular AMD is anti–vascular endothelial growth factor agents (anti-VEGFs), intravitreal therapeutics with demonstrated efficacy in improving visual acuity in patients with neovascular AMD. The management of patients with neovascular AMD is costly and time consuming. The provision of high-quality care requires commitments of significant time and services from physicians, staff, patients, and caregivers.
The objective of this multicenter, mixed-methods, prospective, observational time-and-motion study was to understand the total physician and patient burden of the current standard of care for management of neovascular AMD in the US. This manuscript focuses on the quantitative results from surveys of retina specialists, patients, and associated patient records.
Methods
This multicenter, mixed-methods, prospective, observational time-and-motion study included 3 parts: (1) an ethnographic study, (2) qualitative interviews of patients with a diagnosis of neovascular AMD and their caregivers, and (3) quantitative surveys of retina specialists and patients with a diagnosis of neovascular AMD. There was no institutional review board (IRB) approval for the study, as it was initially conducted (not by RTI Health Solutions) as a market research project and patients were not consented to have their records included in the study. After conferring with the Journal , an exception to IRB approval was permitted in order to have these nonidentifiable data published.
Figure 1 presents an overall summary of the study.
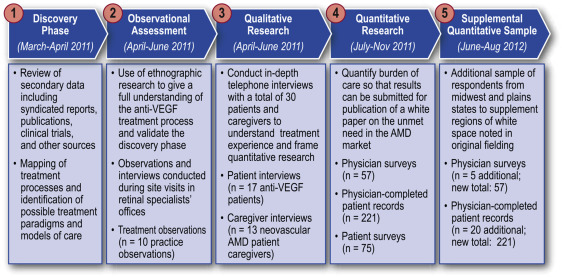
First, an ethnographic study was conducted to gain a full understanding of the intravitreal anti-VEGF treatment process by means of observations and interviews conducted during site visits to 10 retina specialists’ offices in the US. This study consisted of 22 patients (17 established patients receiving a possible reinjection of an anti-VEGF agent, and 5 new patients, receiving their first intravitreal injection of an anti-VEGF agent). Four elements were included in the ethnographic study design:
Patient shadowing: The observer shadowed the patient throughout the entire visit to observe, record, and time the activities that took place and to identify the staff performing each activity. Waiting time that was not directly associated with a particular procedure or test was recorded separately. However, waiting time directly associated with a test was included into the average time for that procedure.
Postobservation debrief with health care provider staff to collect information on office logistics and setting, standard operating procedures, decision to administer anti-VEGF therapy, steps in preparation and administration of anti-VEGF therapy, postinjection examination and discharge, delays in processing patients, challenges with current process, and staff education and training.
Postobservation debrief with retina specialists to collect information on delays in processing patients, injection scheduling, consideration of comorbidities and well-being, additional diagnostic procedures, use of as-needed vs monthly injections, consideration of anti-VEGF alternatives, and any limits on number of injections.
Postobservation debrief with office manager or the reimbursement specialists to collect information on the mix of payers involved, costs and reimbursement of diagnostic tests, requirements for prior authorization, how anti-VEGF therapy is obtained (ie, through the manufacturer/distributor or through a specialty pharmacy), cost and reimbursement for anti-VEGF therapy and the injection procedure, other costs and reimbursement associated with the injection, opinions on current process for anti-VEGF treatment, and the impact of caregivers and disabilities on the process.
Qualitative research also was conducted through 1-hour in-depth telephone interviews with 17 patients receiving anti-VEGF treatment and 13 caregivers of patients with neovascular AMD. A professional moderator trained in techniques to build rapport and elicit deeper insights conducted patient interviews. The aims were to assist in quantifying the burden of care for neovascular AMD, identify drivers and barriers to treatment, and understand the patient experience beyond the injection process in terms of the impact on patient/caregiver quality of life and the burden of time and effort involved. The results of this qualitative research helped in guiding the development of a quantitative survey instrument.
Quantitative research followed, consisting of 3 elements. The first was a telephone survey of 75 patients who had a diagnosis of neovascular AMD, aged 50 years or older, treated in the US by an ophthalmologist or retina specialist, and who received at least 2 injections of anti-VEGF treatment in the 6 months prior to the date of the survey.
Secondly, a paper-based survey was issued to 57 retina specialists in the US who had been recruited randomly and then screened for eligibility until the quota was filled. The recruiting, screening, and selection criteria followed guidelines established by the Council of American Survey Research Organizations. Eligibility criteria included the requirement to have administered 50 or more anti-VEGF inhibitor injections per month. The objective of this portion of the research was to capture each step of an office visit (including injection and monitoring) for the management of neovascular AMD among patients who received intravitreal injections of anti-VEGF agents. The specific information captured concerned preparation required prior to patient arrival, time spent while the patient is in the office, and activities undertaken after the patient leaves, such as reimbursement and billing.
The quantitative research section of this study was conducted between July and November 2011; additional sampling of respondents from Midwest and Great Plains states was carried out from June through August 2012, as these regions were underrepresented in the original sample. A total of 20 states were sampled: Arizona, California, Colorado, Connecticut, Florida, Georgia, Hawaii, Illinois, Iowa, Missouri, Nebraska, New Jersey, New Hampshire, New York, North Carolina, Ohio, Pennsylvania, South Dakota, Texas, and Washington.
Finally, the same physicians also completed paper-based forms for up to 5 neovascular AMD patients scheduled for an office visit within the next 3 weeks (either for follow-up evaluation or for treatment with an additional anti-VEGF injection). The patients were required to be aged 50 years and older and to have received at least 1 injection of anti-VEGF therapy during the 6 months prior to the survey. The form included a patient history section for the physician to complete before the visit, and a patient diary in which the physician recorded activities of the patient visit, materials used, time taken for each step, and staff involvement. The physicians were instructed to complete the patient diary on the same day as the patients’ visit.
Results
The physicians were randomly recruited from a US-based list of retina specialists. Every physician who passed screening for qualification agreed to participate. There were 57 retina specialists involved in the survey, 68% (39 of 57) were in a group practice, 14% (8 of 57) practiced in an academic setting, and 18% (10 of 57) were solo practitioners. The average total number of patients treated per month in these 3 settings was 556, and the average number of neovascular AMD patients treated per month was 201. Fifty-six of the 57 retina specialists completed records on upcoming visits, for a total of 221 patients with neovascular AMD.
The results of the retina specialist survey showed that on average, 23 staff members were involved in the management of neovascular AMD patients, including the receptionist, the office manager, the billing manager, technicians, and other physicians or staff ( Table ). The management of patients with neovascular AMD accounted for an average of 20% of the staff’s time per work week: most technicians (68%) spent more than 20% of their time, one-quarter of office managers spent more than 10% of their time, and more than one-third (37%) of billing managers spent more than 20% of their time managing patients with neovascular AMD ( Figure 2 ).
| Staff Type | Average Number of Staff Type Involved in Neovascular AMD (Range) | Average Total % Time in a 40-Hour Work Week Spent in Neovascular AMD Care (Range) | Average Time per Staff Member per Week Spent on Neovascular AMD | Average Hours per Week Spent on Neovascular AMD, All Staff Members |
|---|---|---|---|---|
| Receptionist | 5 (1–18 people) | 20% (1%–75%) | 8 hours | 28 hours |
| Office manager | 2 (0–10 people) | 13% (0%–75%) | 4 hours | 10 hours |
| Billing manager | 2 (0–6 people) | 22% (0%–80%) | 8 hours | 18 hours |
| Technician a | 8 (1–50 people) | 34% (3%–90%) | 14 hours | 112 hours |
| Physicians other than retina specialists b | 2 (0–18 people) | 15% (0%–65%) | 6 hours | 12 hours |
| Other staff members c | 4 (1–12 people) | 25% (5%–70%) | 10 hours | 40 hours |
| Total | 23 people | Average 20% of individual’s work week | Average 10 hours of individual’s work week | Total office time of 225 hours |
a Technician includes photographer, scribe, and lead technician.
b Physicians other than retina specialists include residents, fellows, other ophthalmologists in the practice, or physician assistants.
c Other staff include medical assistants, optometrists, and nurse technicians.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


