Purpose
To determine the diagnostic capability of spectral-domain optical coherence tomography in glaucoma patients with visual field defects.
Design
Prospective, cross-sectional study.
Methods
settings: Participants were recruited from a university hospital clinic. study population: One eye of 85 normal subjects and 61 glaucoma patients with average visual field mean deviation of −9.61 ± 8.76 dB was selected randomly for the study. A subgroup of the glaucoma patients with early visual field defects was calculated separately. observation procedures: Spectralis optical coherence tomography (Heidelberg Engineering, Inc) circular scans were performed to obtain peripapillary retinal nerve fiber layer (RNFL) thicknesses. The RNFL diagnostic parameters based on the normative database were used alone or in combination for identifying glaucomatous RNFL thinning. main outcome measures: To evaluate diagnostic performance, calculations included areas under the receiver operating characteristic curve, sensitivity, specificity, positive predictive value, negative predictive value, positive likelihood ratio, and negative likelihood ratio.
Results
Overall RNFL thickness had the highest area under the receiver operating characteristic curve values: 0.952 for all patients and 0.895 for the early glaucoma subgroup. For all patients, the highest sensitivity (98.4%; 95% confidence interval, 96.3% to 100%) was achieved by using 2 criteria: ≥ 1 RNFL sectors being abnormal at the < 5% level and overall classification of borderline or outside normal limits, with specificities of 88.9% (95% confidence interval, 84.0% to 94.0%) and 87.1% (95% confidence interval, 81.6% to 92.5%), respectively, for these 2 criteria.
Conclusions
Statistical parameters for evaluating the diagnostic performance of the Spectralis spectral-domain optical coherence tomography were good for early perimetric glaucoma and were excellent for moderately advanced perimetric glaucoma.
Glaucoma is characterized by irreversible damage to the retinal nerve fiber layer (RNFL) and ganglion cell layer with corresponding typical visual field (VF) changes. In the evaluation of glaucoma, RNFL thickness assessment is relevant, because thinning of the RNFL is correlated directly with loss of ganglion cells, which is assumed to be a primary site of glaucomatous damage. RNFL assessment also is potentially useful for the early detection of glaucoma, because RNFL thinning often occurs before clinically detectable vision loss. For example, histologic evaluation of the RNFL has shown that up to 50% of the RNFL may be lost before the initial appearance of VF loss. In addition, clinical evaluation of the RNFL from red-free photographs has suggested that RNFL thinning can be detected in 60% of photographs up to 6 years before the appearance of a VF defect.
Optical coherence tomography (OCT) is an imaging technology that can image and measure glaucomatous RNFL thinning. OCT, first described by Huang and associates in 1991, allows for in vivo noninvasive quantitative evaluation of RNFL thickness. With the ability to measure RNFL thickness directly with axial resolutions of approximately 10 μm and scan speeds of 400 A-lines per second, time-domain OCT (Stratus OCT; Carl Zeiss Meditec, Inc, Dublin, California, USA) has become a common imaging instrument for glaucoma evaluation. Using best RNFL thickness parameters, time-domain OCT has reported sensitivities and specificities for glaucoma diagnosis of 66% to 90% and 80% to 100%, respectively.
Spectral-domain OCT (SD OCT) is a new technology that affords unprecedented ultra–high-resolution ultra–high-speed RNFL imaging. Using the Cirrus HD-OCT (Carl Zeiss Meditec, Inc) machine, the area under the receiver operating characteristic curves (AUCs) were reported to be 0.837 to 0.963 using best RNFL thickness parameters. Using the RTVue (Optovue, Inc, Fremont, California, USA) SD OCT machine, the best AUC value using RNFL thickness determinations was found to be 0.94 for inferior RNFL thickness.
Spectralis OCT (Heidelberg Engineering, Inc, Heidelberg, Germany) is one of the many commercially available SD OCT instruments. It has a scan speed of 40 000 A-lines per second. In addition, Spectralis OCT has the advantage of eye-tracking technology that enables simultaneous real-time imaging with eye-movement tracking. With faster scan speeds and with the eye-tracking system, Spectralis OCT may reduce RNFL thickness measurement variability secondary to movement artifact and may improve measurement accuracy. The current study evaluated the performance of Spectralis SD OCT RNFL thickness values for diagnosing glaucoma. The following variables were determined: AUC, sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (PLR), and negative likelihood ratio (NLR).
Methods
Participants and Examinations
All study subjects were recruited from the Glaucoma Service at the Massachusetts Eye and Ear Infirmary between January 2009 and July 2009. All study subjects underwent a complete eye examination by a glaucoma specialist (T.C.C.) that included history, visual acuity testing, refraction, Goldmann applanation tonometry, slit-lamp biomicroscopy, gonioscopy, ultrasonic pachymetry, dilated ophthalmoscopy, stereo disc photography (Visucam Pro NM; Carl Zeiss Meditec, Inc), VF testing (Swedish Interactive Threshold Algorithm 24–2 test of the Humphrey visual field analyzer 750i; Carl Zeiss Meditec, Inc), and peripapillary RNFL thickness measurements using the Spectralis OCT (Spectralis software version 4.0).
Inclusion criteria included patients with a spherical equivalent between −5.0 and 5.0 diopters and with a best-corrected visual acuity of 20/40 or better. The study included only patients with reliable VF testing with less than 33% fixation losses, less than 20% false-positive results, and less than 20% false-negative results. Patients were excluded if they had discernible congenital anomalies of the anterior chamber, corneal scarring or opacities, diabetic proliferative or severe nonproliferative retinopathy, VF loss attributable to a nonglaucoma condition, or a dilated pupil diameter of less than 2 mm.
Glaucoma patients were defined as having characteristic changes of the optic nerve head with corresponding abnormal VF defects. The VF was considered to be abnormal if 3 or more contiguous test locations in the pattern standard deviation plot were depressed significantly at the P < .05 level with at least 1 at the P < .01 level on the same side of the horizontal meridian and if the VF defect corresponded to the optic nerve appearance. Except for traumatic glaucoma, all types of glaucoma were included. VF abnormalities were classified as mild (mean deviation [MD] > −6 decibels [dB]), moderate (−12 dB < MD ≤ −6 dB), or severe (MD ≤ −12 dB). Normal subjects were those without ocular disease, except for mild cataracts, and those with normal VF test results, as defined by pattern standard deviation of more than 5% and glaucoma hemifield test results within normal limits. If both eyes were eligible for the study, 1 eye was selected by the investigator, who was masked to the OCT results at the time selection was made and who used a random number generator statistical table.
Spectralis Optical Coherence Tomography Peripapillary Retinal Nerve Fiber Layer Measurement
All SD OCT imaging was performed after pupillary dilation with the Spectralis OCT (version 4.0), which has an acquisition rate of 40 000 A-lines per second, an axial resolution of 7 μm in tissue, and an 870-nm superluminescent diode source. More details of the SD OCT technique have been described elsewhere. The circular scan pattern was used for peripapillary RNFL thickness measurements. The scan circle was 12 degrees in diameter, and the scan circle diameter in millimeters primarily is dependent on the axial eye length. For a typical eye length, the circle is approximately 3.5 to 3.6 mm in diameter. Images were acquired by different operators but on the same day as the VF examination.
Spectralis OCT provides an automatic real-time function with an eye-tracking system that can increase image quality. With the automatic real-time function activated, multiple frames of the same scanning location are obtained. These data then are averaged for noise reduction, and eye-motion artifacts are reduced. In this study, 16 frames were acquired per eye with the automatic real-time function on. As suggested by the manufacturer, scans with signal strength of less than 15 (range, 0 to 40) were excluded from the analysis. In addition, criteria for determining adequate scan quality were as follows: a clear fundus image with good optic disc and scan circle visibility before and during image acquisition, RNFL visible and without interruptions, and a continuous scan pattern without missing or blank areas.
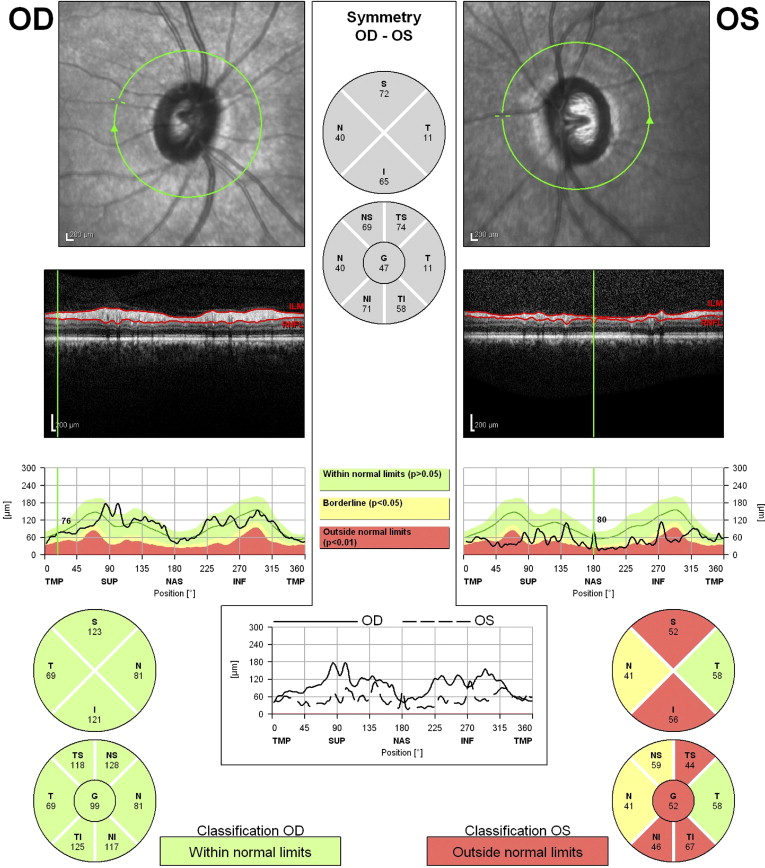
The Spectralis OCT software calculates the average RNFL thickness for the overall globe (360 degrees), for quadrants (ie, superior [S], inferior [I], nasal [N], and temporal , each 90 degrees), and additionally for 4 sectors (ie, superior-temporal [TS], superior-nasal [NS], inferior-nasal [NI], and inferior-temporal [TI]; Figure ). In the Spectralis OCT RNFL printouts, not only are the RNFL thickness values for the above areas shown, but also the classifications are displayed in 3 different colors ( Figure ). The green, yellow, and red areas are determined by comparing the patient’s RNFL thickness values with those of a normative database, with green representing the 95% normal range, yellow (borderline classification) representing values outside the 95% confidence interval but within the 99% confidence interval of the normal distribution (.01 < P < .05), and red (outside normal limits) representing values outside the 99% confidence interval of the normal distribution. The colored bar at the bottom of the printout indicates the overall classification. The bar is red (outside normal limits) if the RNFL thickness of 1 or more sectors (TS, NS, NI, TI), T quadrant or N quadrant, or overall global average is outside normal limits. The bar is yellow (borderline) if the RNFL thickness of 1 or more sectors (TS, NS, NI, TI), temporal or nasal quadrant, or overall global average is classified as borderline, but none is outside normal limits. If all sectors, temporal and nasal quadrant, and overall global average RNFL thickness are classified as within normal limits, the bar will appear green (within normal limits).
Statistical Analysis
Demographic characteristics of the normal and glaucoma groups were compared using chi-square tests and nonpaired 2-tailed Student’s t tests for categorical and continuous variables, respectively. Receiver operating characteristic curves and AUCs were calculated for the RNFL thickness parameters of the overall globe, 4 quadrants, and 4 sectors. A statistical tool (MedCalc version 11.5.1; MedCalc Software bvba, Mariakerke, Belgium) was used when comparing AUCs.
Using RNFL thickness parameters, sensitivity, specificity, PPV, NPV, PLR, and NLR of 6 criteria were tested: (1) average overall globe RNFL thickness abnormal at the < 5% level; (2) average overall globe RNFL thickness abnormal at the < 1% level; (3) ≥ 1 quadrants abnormal at the < 5% level; (4) ≥ 1 quadrants abnormal at the < 1% level; (5) ≥ 1 sectors (TS, TI, NS, and NI) abnormal at the < 5% level; and (6) ≥ 1 sectors (TS, TI, NS, and NI) abnormal at the < 1% level.
Sensitivity, specificity, PPV, NPV, PLR, and NLR also were evaluated for 10 additional diagnostic criteria that combined the parameters with the best AUC values. These 10 diagnostic criteria were (1) overall classification (provided by Spectralis software) of outside normal limits; (2) overall classification of borderline or outside normal limits; (3) overall, superior, or inferior quadrants with RNFL thickness values abnormal at the < 5% level; (4) overall, superior, or inferior quadrants with RNFL thickness values abnormal at the < 1% level; (5) superior or inferior quadrants with RNFL thickness values abnormal at the < 5% level; (6) superior or inferior quadrants with RNFL thickness values abnormal at the < 1% level; (7) overall, TS, or TI sectors with RNFL thickness values abnormal at the < 5% level; (8) overall, TS, or TI sectors with RNFL thickness values abnormal at the < 1% level; (9) TS or TI sectors with RNFL thickness values abnormal at the < 5% level; (10) and TS or TI sectors with RNFL thickness values abnormal at the < 1% level.
Sensitivity, specificity, PPV, and NPV were calculated using conventional 2 × 2 tables. The use of likelihood ratio tests has been promoted to assist in interpreting diagnostic tests in medicine. PLR and NLR were calculated using the formulae PLR = sensitivity/(1 − specificity) and NLR = (1 − sensitivity)/specificity. A large PLR (for example, a value more than 10) helps to rule in disease, and a small NLR (for example, a value less than 0.1) helps to rule out disease. In the current study, the criteria of PLR > 10 and NLR < 0.1 were used to determine whether Spectralis SD OCT RNFL thickness measurements were good for diagnosing glaucoma. Statistical analyses were performed using SPSS software version 15.0 (SPSS, Inc, Chicago, Illinois, USA). P < .05 was considered to be statistically significant, and P < .001 was considered to be highly statistically significant.
Results
A total of 146 participants (85 normal subjects and 61 glaucoma patients) were studied. The characteristics of the study population are listed in Table 1 . Types of glaucoma included primary open-angle glaucoma (41 of 61 patients; 67.2%), normal-tension glaucoma (6 of 61 patients; 9.8%), pseudoexfoliation glaucoma (6 of 61 patients; 9.8%), chronic angle-closure glaucoma (4 of 61 patients; 6.6%), inflammatory glaucoma (1 of 61 patients; 1.6%), pigmentary glaucoma (1 of 61 patients; 1.6%), juvenile open-angle glaucoma (1 of 61 patients; 1.6%), and iridocorneal endothelial syndrome with glaucoma (1 of 61 patients; 1.6%). Severity of VF defects was distributed equally among mild VF defects (23 of 61 patients; 37.7%), moderate VF defects (17 of 61 patients; 27.9%), and severe VF defects (21 of 61 patients; 34.4%).
| Normal | Glaucoma | All | P Value a | |
|---|---|---|---|---|
| No. of eyes | 85 | 61 | 146 | |
| No. of right eyes (% total) | 60.0 | 62.3 | 61.0 | .779 |
| Mean age (years) | 63.5 ± 14.0 | 69.2 ± 13.0 | 66.4 ± 13.8 | |
| Range | 18 to 90 | 18 to 89 | 18 to 90 | .054 |
| Female (% total) | 52.9 | 59.0 | 55.5 | .466 |
| Race (% total white) | 74.1 | 67.2 | 71.2 | .363 |
| Refractive error (spherical equivalent in diopters) | −0.95 ± 1.94 | −1.33 ± 1.74 | .067 | |
| VF mean deviation (dB) | −1.25 ± 1.74 | −9.61 ± 8.76 | < .001 | |
| VF pattern standard deviation (dB) | 1.82 ± 1.31 | 6.14 ± 3.43 | < .001 |
a When comparing normal and glaucoma groups, chi-square tests were used for categorical variables and nonpaired 2-tailed Student’s t tests were used for continuous variables.
Table 2 compares the mean RNFL thickness values for normal versus glaucoma patients. The mean overall RNFL thickness was 94.3 ± 8.8 μm for normal subjects and 65.3 ± 16.5 μm for glaucoma patients.
| RNFL Thickness (μm) | Normal Eyes (n = 85), Mean ± SD | Glaucomatous Eyes (n = 61), Mean ± SD |
|---|---|---|
| Overall global average | 94.3 ± 8.8 | 65.3 ± 16.5 a |
| Superior quadrant | 111.5 ± 14.4 | 73.4 ± 21.9 a |
| Temporal quadrant | 70.3 ± 10.6 | 54.9 ± 13.9 a |
| Inferior quadrant | 119.7 ± 15.9 | 75.3 ± 27.3 a |
| Nasal quadrant | 74.9 ± 11.6 | 57.2 ± 18.0 a |
| TS sector | 124.5 ± 16.4 | 78.0 ± 28.5 a |
| TI sector | 136.0 ± 20.5 | 76.9 ± 29.3 a |
| NS sector | 98.7 ± 19.9 | 68.8 ± 23.0 a |
| NI sector | 103.9 ± 20.8 | 73.8 ± 29.7 a |
a Significantly different ( P < .001) when compared with the normal group (analysis of variance).
Table 3 summarizes AUC data for all RNFL thickness parameters. Table 3 lists the AUC for each parameter generated by the Spectralis OCT peripapillary RNFL scan for 2 groups: (1) all glaucoma patients and (2) early glaucoma patients with mild VF defects. In the group of all the glaucoma patients, the overall RNFL thickness had the highest AUC value (0.952), followed by the TI sector (0.947), superior quadrant (0.925), TS sector (0.911), and inferior quadrant (0.905), and these latter 4 values were not significantly lower than the highest value. The AUC value for overall RNFL thickness was significantly higher than those for the temporal and nasal quadrants, as well as the NS and NI sectors. In the group of glaucoma patients with mild VF defects, overall RNFL thickness had the highest AUC (0.895). Other RNFL parameters with similarly high AUC values were the TI sector (0.888), TS sector (0.873), superior quadrant (0.864), and inferior quadrant (0.861).
| OCT Parameter | All Glaucoma Patients | Glaucoma Patients with Mild VF Loss | ||
|---|---|---|---|---|
| AUC (95% CI) | P Value a | AUC (95% CI) | P Value a | |
| Overall RNFL thickness | 0.952 (0.915 to 0.990) | 0.895 (0.807 to 0.983) | ||
| Superior RNFL thickness | 0.925 (0.881 to 0.969) | .3530 | 0.864 (0.773 to 0.955) | .6300 |
| Temporal RNFL thickness | 0.808 (0.734 to 0.881) | < .001 | 0.718 (0.589 to 0.847) | < .05 |
| Inferior RNFL thickness | 0.905 (0.848 to 0.963) | .1752 | 0.861 (0.755 to 0.967) | .6286 |
| Nasal RNFL thickness | 0.801 (0.726 to 0.877) | < .001 | 0.707 (0.577 to 0.836) | < .05 |
| TS RNFL thickness | 0.911 (0.859 to 0.963) | .2029 | 0.873 (0.774 to 0.972) | .7463 |
| TI RNFL thickness | 0.947 (0.906 to 0.988) | .8599 | 0.888 (0.792 to 0.985) | .9162 |
| NS RNFL thickness | 0.847 (0.781 to 0.914) | < .05 | 0.725 (0.593 to 0.857) | < .05 |
| NI RNFL thickness | 0.819 (0.739 to 0.898) | < .05 | 0.739 (0.605 to 0.873) | .0583 |
Tables 4 and 5 lists the calculated sensitivities, specificities, PPVs, NPVs, PLRs, and NLRs for 6 RNFL thickness criteria. Table 4 lists these diagnostic parameters for all glaucoma patients, and Table 5 lists these diagnostic parameters for early glaucoma patients with mild VF defects. Of the 6 RNFL thickness criteria for the glaucoma group ( Table 4 ), best sensitivity (98.4%) and NPV (98.6%) were achieved when 1 or more of the RNFL thickness sectors was abnormal at the < 5% level. The best specificity (100%) and PPV (100%) were achieved when overall globe RNFL thickness was abnormal at the < 1% level. The only criteria with both PLR of more than 10 and NLR of less than 0.1 was 1 or more RNFL sectors abnormal at the < 1% level. Of the 6 RNFL thickness criteria for the early glaucoma group with mild VF defects ( Table 5 ), similar results were obtained. The only RNFL criteria with both PLR of more than 10 and NLR of less than 0.1 was 1 or more RNFL sectors abnormal at < 1% level.
| OCT Parameter | Sensitivity % (95% CI) | Specificity % (95% CI) | PPV % (95% CI) | NPV % (95% CI) | LRP (95% CI) | LRN (95% CI) |
|---|---|---|---|---|---|---|
| Overall global RNFL thickness abnormal at < 5% level | 80.3 (73.9 to 86.85) | 92.9 (88.8 to 97.1) | 89.1 (84.0 to 94.1) | 86.8 (81.3 to 92.3) | 11.38 (6.59 to 29.88) | 0.21 (0.14 to 0.29) |
| Overall global RNFL thickness abnormal at < 1% level | 67.2 (59.6 to 74.8) | 100 | 100 | 81.0 (74.6 to 87.3) | + Infinity | 0.33 (0.25 to 0.40) |
| ≥ 1 quadrants with RNFL thickness abnormal at < 5% level | 96.7 (93.8 to 99.6) | 85.9 (80.2 to 91.5) | 83.1 (77.0 to 89.2) | 97.3 (94.7 to 99.9) | 6.85 (4.75 to 11.76) | 0.04 (0 to 0.08) |
| ≥ 1 quadrants with RNFL thickness abnormal at < 1% level | 88.5 (83.4 to 93.7) | 95.3 (91.9 to 98.7) | 93.1 (89.0 to 97.2) | 92.0 (87.7 to 96.4) | 18.81 (10.24 to 73.73) | 0.12 (0.06 to 0.18) |
| ≥ 1 sectors of TS, TI, NS, NI with RNFL thickness abnormal at < 5% level | 98.4 (96.3 to 100) | 88.9 (84.0 to 94.0) | 87.0 (81.5 to 92.4) | 98.6 (96.7 to 100) | 8.85 (5.94 to 16.70) | 0.02 (0 to 0.04) |
| ≥ 1 sectors of TS, TI, NS, NI with RNFL thickness abnormal at < 1% level | 93.4 (89.4 to 97.5) | 95.3 (91.9 to 98.7) | 93.4 (89.4 to 97.5) | 95.3 (91.9 to 98.7) | 19.86 (10.98 to 76.69) | 0.07 (0.03 to 0.12) |
| OCT Parameter | Sensitivity % (95% CI) | Specificity % (95% CI) | PPV % (95% CI) | NPV % (95% CI) | LRP (95% CI) | LRN (95% CI) |
|---|---|---|---|---|---|---|
| Overall global RNFL thickness abnormal at < 5% level | 65.2 (57.5 to 72.9) | 92.9 (88.8 to 97.1) | 71.4 (64.1 to 78.8) | 90.8 (86.1 to 95.5) | 9.24 (5.13 to 25.12) | 0.37 (0.28 to 0.48) |
| Overall global RNFL thickness abnormal at < 1% level | 47.8 (39.7 to 55.9) | 100 | 100 | 87.6 (82.3 to 93.0) | + Infinity | 0.52 (0.44 to 0.60) |
| ≥ 1 quadrants with RNFL thickness abnormal at < 5% level | 91.3 (86.7 to 95.9) | 85.9 (80.2 to 91.5) | 63.6 (55.8 to 71.4) | 97.3 (94.7 to 99.9) | 6.47 (4.39 to 11.32) | 0.10 (0.05 to 0.17) |
| ≥ 1 quadrants with RNFL thickness abnormal at < 1% level | 78.3 (71.6 to 85.0) | 95.3 (91.9 to 98.7) | 81.8 (75.6 to 88.1) | 94.2 (90.4 to 98.0) | 16.63 (8.79 to 66.85) | 0.23 (0.15 to 0.31) |
| ≥ 1 sectors of TS, TI, NS, NI with RNFL thickness abnormal at < 5% level | 95.2 (91.8 to 98.7) | 88.9 (84.0 to 94.0) | 69.0 (61.5 to 76.5) | 98.6 (96.7 to 100) | 8.57 (5.67 to 16.41) | 0.05 (0.01 to 0.10) |
| ≥ 1 sectors of TS, TI, NS, NI with RNFL thickness abnormal at < 1% level | 91.3 (86.7 to 95.9) | 95.3 (91.9 to 98.7) | 84.0 (78.1 to 89.9) | 97.6 (95.1 to 100) | 19.40 (10.65 to 75.44) | 0.09 (0.04 to 0.14) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


