Eyelid abnormalities
Ectropion
Entropion
Lagophthalmos
Floppy eyelid syndrome
Conjunctival abnormalities
Pinguecula
Pterygium
Trabeculectomy
Superior limbic keratoconjunctivitis
Conjunctivochalasis
Corneal disorders
Anterior basement membrane disease
Recurrent erosion syndrome
Salzmann nodular degeneration
After external and anatomical considerations, the next step in diagnosing DES is evaluating which part of the tear film is dysfunctional. The tear film is a complex fluid made up of lipids, an aqueous layer, and mucins (Fig. 1.1). Most patients with DES have dysfunction in more than one layer although there is typically one that is most affected. For examples, patients with Sjogren’s syndrome or graft-versus-host disease (GVHD) typically have primarily aqueous tear deficiency (ATD), while patients with rosacea typically have mostly evaporative dry eye (LTD). Several tests are used to evaluate tear function as this information has implications for treatment (Table 1.2). Schirmer’s test with or without anesthesia can be used to assess aqueous production (Fig. 1.2), while tear break-up time and evaluation of meibomian gland parameters can evaluate the composition and function of the lipid layer (Fig. 1.3). Other tests, such as measurement of tear osmolarity, can give a global assessment of tear health as hyperosmolarity is believed to be a key player in the pathophysiology of disease (Fig. 1.4) (DEWS 2007b). It is important, however, to understand that none of the tests are a perfect mirror of tear function and that the results can vary substantially both due to testing methodology and to the dynamic biology of the tear film. With regard to the former, tear break-up times vary substantially by the amount of fluorescein placed in the eye. With regard to the latter, tear osmolarity values can vary substantially when measured in the same individual 3 times in a row, a finding that suggests the presence of ocular surface instability. Despite these limitations, a general “gestalt” of tear function can be obtained by measuring some or all of these parameters. Newer tests are currently being evaluated that may better assess the dynamic state of the tear film including functional visual acuity (FVA) testing (Goto et al. 2006; Ishida et al. 2005) and evaluating tear film stability with consecutive topographic images (Tear film Stability Analysis System) (Gumus et al. 2011). However, these newer tests are not in widespread use in the clinical arena.
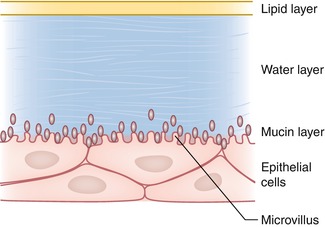
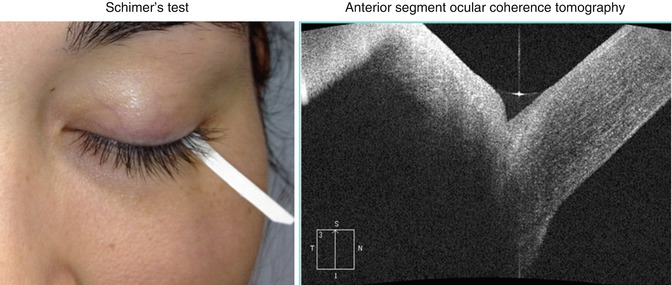
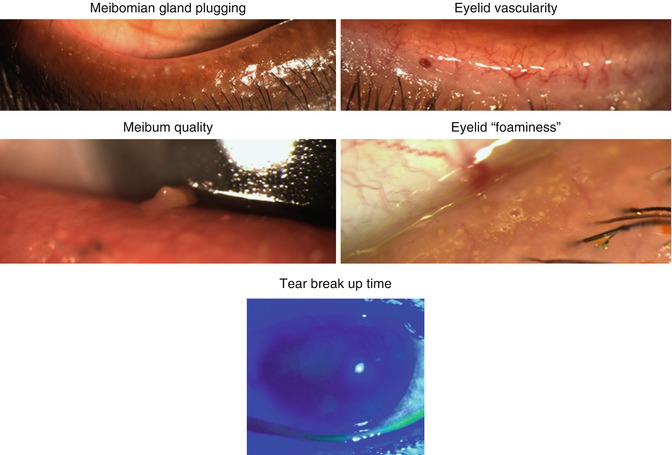
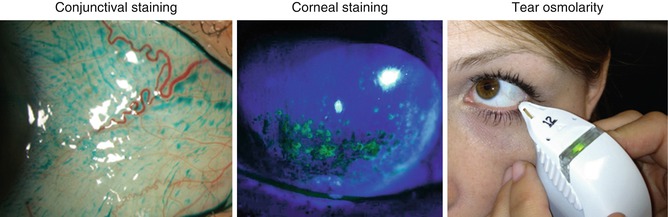
Fig. 1.1
An illustration of the tear film demonstrating its complexity, with a mucin, aqueous, and lipid layer (Used with kind permission from Allergan)
Table 1.2
Common tests used to evaluate tear and ocular surface health
Global assessment of health |
Tear osmolarity (TearLab, San Diego, CA) |
Corneal staining |
Conjunctival staining |
Tear film debris |
Presence of filaments |
Presence of irregular astigmatism by corneal imaging (topography, tomography) |
Elevated level of MMP-9 (InflammaDry, Rapid Pathogen Screening, Sarasota, FL) |
Aqueous tear function |
Schirmer’s test |
Inferior meniscus volume (inspection at slit lamp or with ocular coherence tomography) |
Lipid tear function |
Tear break-up time |
Meibum quality |
Meibomian gland inspissation |
Eyelid vascularity |
Eyelid “foaminess” |
Interferometer (LipiView, Tear Science, Morrisville, NC) |
Fig. 1.2
Commonly used tests in dry eye syndrome (DES) to assess the aqueous component of tears
Fig. 1.3
Commonly used tests in dry eye syndrome (DES) to assess the lipid component of tears. For example, morphologic evaluation can include degree of inferior eyelid meibomian orifice plugging (0 none; 1 less than 1/3 lid involvement; 2 between 1/3 and 2/3 involvement; 3 greater than 2/3 lid involvement), degree of eyelid vascularity (0 none; 1 mild engorgement; 2 moderate engorgement; 3 severe engorgement) (Foulks and Bron 2003), and meibum quality (0 = clear; 1 = cloudy; 2 = granular; 3 = toothpaste; 4 = no meibum extracted) (Tomlinson et al. 2011). Expression of meibum can be done with a cotton-tipped applicator or with the Meibomian Gland Evaluator, a device that applies a uniform pressure to the outer skin of the lower eyelid
Fig. 1.4
Commonly used tests in dry eye syndrome (DES) to assess global ocular surface health. For example, a score for corneal staining can be generated by assessing staining in different sections of the cornea (superior, inferior, nasal, temporal, center) or by assigning an overall score for severity (DEWS 2007a). A similar can be used for conjunctival staining
Interferometry is another test that can be performed to evaluate the health of the lipid layer (Tomlinson and Khanal 2005). In this technique, interference fringes are produced by light reflected at the air-lipid and lipid-aqueous interfaces of the tear film. This specular reflection from the tear surface is imaged and recorded digitally. Several researchers have developed grading patterns to interpret the recorded images, most focusing on the uniformity of the fringe pattern. Overall, research has demonstrated that a thicker lipid layer is associated with greater tear film stability and that loss of uniformity indicates tear film instability (Tomlinson and Khanal 2005). LipiView® (Tear Science, Morrisville, NC) is a commercially available interferometer that comes as part of the Tear Science diagnosis and treatment system (described below).
Another adjuvant study that can be used to evaluate for the presence of ocular surface inflammation is the InflammaDry™ assay (Rapid Pathogen Screening, Sarasota, FL). This test detects elevated levels of matrix metalloproteinase-9 (MMP-9) in the tear film. MMP-9 is a nonspecific marker of inflammation and has been found to be elevated in various ocular surface disorders and corneal ulceration (Kaufman 2013). An advantage of the test is its ease and rapidity; the applicator is placed in the lower conjunctivae to sample tears, and the results are available within 10 min. A limitation, however, is that the test result is reported in binary fashion: two lines indicate an elevated MMP-9 level; one line indicates a normal level.
Newer data suggest that DES may be a manifestation of a corneal neuropathy (Rosenthal et al. 2009; Rosenthal and Borsook 2012) and evaluation of corneal sensation should be considered, especially in patients with extensive corneal staining and minimal disease symptoms. Available technologies include the more qualitative cotton-tip swab which can compare sensation between the eyes and the more quantitative Cochet-Bonnet esthesiometer (Luneau Ophthalmologie, Chartres, France). Belmonte et al. (1999) developed a noncontact gas esthesiometer that can measure corneal threshold to mechanical, thermal, and chemical stimulation. Unfortunately, this esthesiometer is not commercially available and only four modified versions of the instrument are available worldwide.
Another commercially available tool that can be used to study corneal nerves is the confocal microscope (Confoscan 4, Nidek, Fremont, California). In vivo confocal microscopy can be used to image corneal nerves in the sub-basal plexis. Several studies have found abnormal corneal nerve morphology in patients with DES including increased nerve tortuosity, fewer fibers, and higher bead density (Zhang et al. 2011; Villani et al. 2013). This testing, however, is in its infancy, and at this point it is not clear what role nerve imaging will have in the diagnosis and treatment of DES.
1.3 Treating Dry Eye Syndrome
1.3.1 Ocular Surface Protection
The treatment of DES involves a stepladder approach based on the location of the abnormality (Fig. 1.5). The first step in treating ATD is protection of the ocular surface with artificial tears. There are several available products that vary in viscosity, polymer material (methylcellulose, propylene glycol, glycerin, polyvinyl alcohol), and preservative. In addition, some products include additional agents such as lipid replacement (e.g., Soothe (Bausch & Lomb, Rochester NY), Systane balance (Alcon, Fort Worth TX)), while others have properties such as hyposmolarity. A complete list of artificial tear properties and preservatives can be found on the website http://www.dryeyezone.com/encyclopedia/lubricants.html. In general, patients should consider preservative-free options if they require dosing of more than 4 times daily. Patients with more severe symptoms should consider higher-viscosity agents although these tend to cause more visual blurring. Furthermore, gels and ointment are available for nighttime use in those with persistent symptoms.
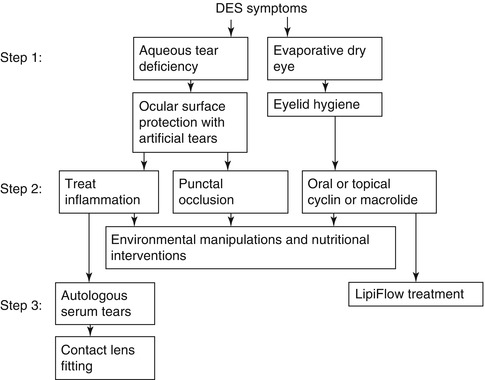
Fig. 1.5
An algorithm for treating dry eye symptoms
1.3.2 Treating Inflammation
The next step in ATD treatment is targeting inflammation. Inflammation has been demonstrated to be a key player in DES. T cells, cellular markers of inflammation (human leukocyte antigen (HLA) DR), inflammatory cytokines (interleukin (IL)-1, IL-6, and tumor necrosis factor (TNF), and chemokines (IL-8 (CXCL8)) have all been found on the ocular surface of dry eye suffers (Stevenson et al. 2012). Targeting inflammation is therefore one important avenue of treatment. While topical corticosteroids are an effective treatment, their side effects of cataract formation and intraocular pressure elevation limit their use in chronic diseases. Cyclosporine 0.05 % (Restasis, Allergan, Irvine CA) is the only Food and Drug Administration (FDA)-approved product for DES in the USA. Several clinical trials demonstrated improvement in symptoms, signs, and inflammatory markers with the use of topical cyclosporine (Stevenson et al. 2000; Sall et al. 2000; Brignole et al. 2001). In patients with immune-mediated ocular inflammation such as those with graft-versus-host disease, one can consider using cyclosporine compounded at a higher concentration (0.5 %, 2 %). Other anti-inflammatory agents are being evaluated in DES but have not yet received FDA approval. Topical tofacitinib, a Janus kinase inhibitor, is one such agent that has been tested in patients with DES in a phase I/II trial. While the agent did not meet its primary endpoint for efficacy, tofacitinib was superior to cyclosporine emulsion with respect to ocular surface symptoms and side effects. However, neither agent was more effective than vehicle in reducing corneal staining (Liew et al. 2012; Huang et al. 2012).
1.3.3 Punctal Occlusion
Another option for the treatment of ATD is temporary or permanent occlusion of the punctae. While this option should be considered in patients with primary and likely irreversible ATD such as those with GVHD, Sjogren’s syndrome, or radiation keratopathy, there is less enthusiasm for the procedure in those with concomitant LTD and/or significant ocular surface inflammation. This is because the punctae are likely one avenue for the elimination of cellular and soluble inflammatory mediators from the ocular surface and their occlusion can exacerbate disease.
1.3.4 Treating Lid Disease
The first-line treatment for LTD is lid hygiene (Fig. 1.5). This process involves heating the eyelids and massaging the meibomian gland openings. There are many different ways to perform this routine including adding baby shampoo to warm water or applying a heated sock filled with rice to the eyelids. The main barrier to treatment response is patient compliance as many patients enthusiastically follow the instructions for a short time prior to discontinuing therapy. It is therefore important to stress that lid hygiene must be incorporated into a patient’s daily routine, with cues such as placing a note on the bathroom mirror as a reminder until the routine has been solidified.
Oral or topical cyclins or macrolides are a second-line therapy for LTD. Doxycycline 20–100 mg once or twice daily or minocycline 50–100 mg once daily can be used for varying lengths of time (typically for at least 1 month). It is important to counsel patients on potential side effects of therapy which include but are not limited to gastrointestinal upset and sensitivity to sunlight. Azithromycin is an alternative medication that can be used topically or orally to treat lipid tear abnormalities (Igami et al. 2011; Luchs 2008; Greene et al. 2014). It is important, however, to remember that a rare but serious side effect of oral azithromycin is heart block (FDA 2013). Topical azithromycin 1 % (Azasite, Merck, Boston MA) can be used twice daily as an off-label treatment for LTD, often for a similar length of time as oral agents (Luchs 2008).
Tetracycline derivatives likely affect lipid deficiency both through their antibacterial and anti-inflammatory properties. Doxycycline has been shown to downregulate the expression of proinflammatory cytokines and chemokines and inhibits the activity of matrix metallopeptidase (MMP) (Stevenson et al. 2012).
A newer option for the treatment of LTD is the LipiFlow® Thermal Pulsation System (Tear Science, Morrisville, NC). This device has two arms, an interferometer (LipiView®) to aid in the diagnosis of concomitant LTD and the treatment arm (LipiFlow). The interferometer illuminates the tear film and measures the interference pattern of the reflected light. This pattern is analyzed by software included with the device and generates a thickness measurement for the lipid layer. The software then advises based on the thickness and pattern of interferometry whether the LipiFlow treatment is advised. LipiFlow uses heat and gentle pulsatile pressure to unblock obstructed meibomian glands during an in-office procedure with the goal of restoring the natural production of lipids. Twenty-one patients with LTD who received one LipiFlow treatment were found to have improved symptoms, meibomian gland secretion scores, and tear break-up times both 1 and 9 months after treatment (Greiner 2012). Its current use, however, is limited mainly by the cost of treatment as patients must usually pay out of pocket for the procedure.
1.3.5 Nutritional Considerations
There is epidemiologic support that nutrition can affect dry eye status with low levels of antioxidants being a risk factor and elevated levels of omega-3 fatty acids (FA) being a protective factor for dry eye (Cejkova et al. 2008; Cermak et al. 2003; Miljanovic et al. 2005). A multicentered, masked, randomized trial of omega-3 and omega-6 FA oral supplementation found a significant decrease in conjunctival inflammation, as measured by the percentage of HLA-DR-positive cells, in the treatment group after 3 months of therapy (Brignole-Baudouin et al. 2011). These findings, taken together, suggest that all patients with symptomatic DES can be counseled on the use of dietary supplementation with antioxidants and omega-3 FA as an adjuvant to their dry eye therapy. Omega-3 FA may improve tear health through several mechanisms including influencing inflammation and modulating meibum quality. With regard to inflammation, omega-3 FAs were found to block the production of proinflammatory eicosanoids and cytokines (IL-1 and TNF) (Stevenson et al. 2012). With regard to meibum quality, one study of women with Sjogren’s syndrome found a difference in polar lipid profiles based on intake of omega-3 (Sullivan et al. 2002).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


