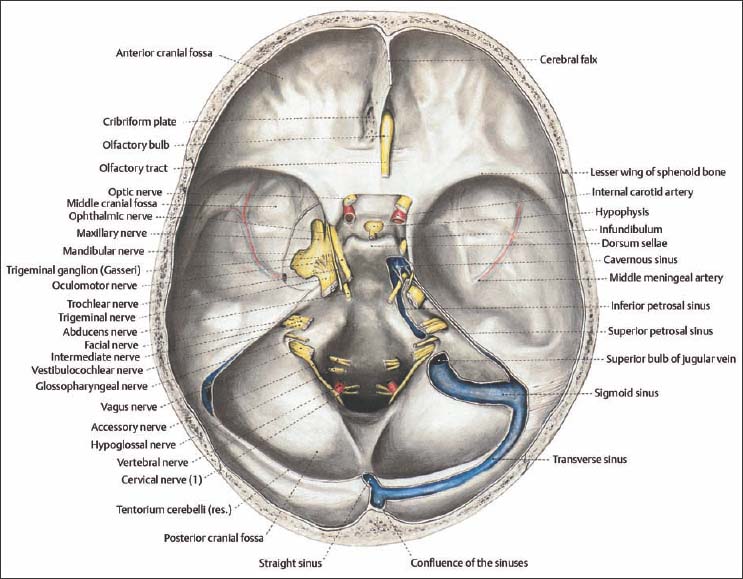
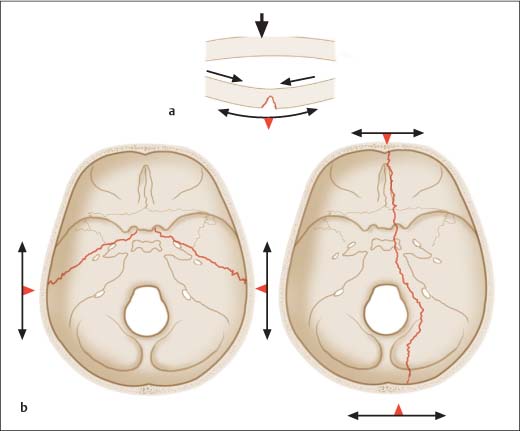
6 Diagnosing Injuries of the Skull Base The bony architecture of the skull base can be divided into three depressions: the anterior, middle, and posterior cranial fossae. The interior surface of the cranial base is comprised of the following (Fig. 6.1): Fig. 6.1 Overview of the anatomic structures of the skull base (from Tillmann 1997). The anterior cranial fossa is made up of two bones: the ethmoid bone and the frontal bone. These form the floor, sides, and anterior wall of the cranial base. The boundary to the middle cranial fossa is formed by the lesser wings of the sphenoid bone. The anterior skull base provides the roof for the pair of orbital cavities and the upper portion of the nasal cavity. At the center of the anterior cranial fossa is the cribriform plate, part of the ethmoid bone. Traversing the cribriform plate through openings in the plate are the fine olfactory nerves, which are covered by a dural sheath and enclosed in the subarachnoid space. There can be considerable differences in height between the ethmoid bone and the cribriform plate. In the center of the cribriform plate is a sagittally positioned bony process, the crista galli, which is sometimes pneumatized. The cerebral falx, which divides the two halves of the brain, is firmly anchored to the crista galli. The middle cranial fossa is also partially formed by the temporal bone, which is made up of petrous (pyramid), squamous, and tympanic portions. The roof of the tympanic cavity (tegmen tympani) and antrum (tegmen antri) thus forms part of the floor of the middle cranial fossa. The optic canal, containing the optic nerve and ophthalmic artery, is located in the middle cranial fossa. Lateral to the apex of the petrous pyramid is the trigeminal ganglion of the trigeminal nerve. The trigeminal ganglion emerges as the mandibular nerve from the foramen ovale and as the maxillary nerve from the foramen rotundum. The foramen spinosum transmits the middle meningeal arteries. The foramen lacerum, transmitting the greater superficial petrosal nerve, is located in front of the carotid canal in which the carotid artery lies. After entering the cranial cavity, the internal carotid artery travels in the carotid canal lateral to the cavernous sinus for a short distance. The middle cranial fossa is divided by the pituitary fossa (sella turcica), which contains the pituitary gland at its center. On the posterior side of the pituitary fossa, the clivus slopes down toward the posterior cranial fossa. The pituitary fossa is formed by the sphenoid body with the lesser and greater wings of sphenoid bone: Between the lesser and greater wings of the sphenoid bone is a gap, the superior orbital fissure, containing the trochlear nerve, abducens nerve, oculomotor nerve, ophthalmic nerve, and superior orbital vein. The posterior cranial fossa is separated from the middle cranial fossa by the edge of the petrous pyramid. At the center of the pyramid is the opening to the internal acoustic meatus, which transmits the vestibulocochlear nerve, facial nerve, and labyrinthine vessels. Directly adjacent to the pyramid is the sigmoid sinus, which flows into the jugular bulb and exits the cranial fossa together with the glossopharyngeal nerve, vagus nerve, and accessory nerve—via the jugular foramen. The foramen magnum is the largest opening in the posterior cranial fossa, allowing entrance of the medulla oblongata and vertebral artery into the cranial cavity. Enclosing the brain is the dura mater, which is made up of an inner and outer layer. The outer layer forms the periosteal covering of the cranial bone. This internal periosteum is firmly attached near the crista galli. At the posterior wall of the frontal sinuses, the periosteum gradually separates from the bone. Injuries of the skull base can be divided into bursting fractures and bending fractures. Bending fractures are caused by direct, focused trauma to the skull. Depression of the bone at the site of impact results, which typically produces comminuted or perforated fractures (Fig. 6.2a). Bursting fractures are caused by objects with a wide surface area and indirect trauma to the cranial bones. The resulting force is transmitted and, in areas where the bone is thin, minimal elasticity results in breakage, i. e., bursting fractures (Fig. 6.2b). Fig. 6.2 Etiology of bending (a) and bursting fractures (b). a Focused trauma leads to primary fissure formation on the opposite surface of the bone, or to complete fracture, given sufficient force. b Impact over a broad area of bone leads to compression, and ultimately a bursting fracture of the skull base. Osseous injury of the skull base can cause a tear in the dura mater, attached to the bone. The firm attachment in the nasal fossa region of the dura mater makes this a site at high risk of injury. The dura mater is a bradytrophic tissue; healing is slow and occurs with connective tissue scar formation. In injuries involving the skull base, resulting swelling of the brain can cause a defect in the cranial base without primary cerebrospinal fluid leak. The arachnoid membrane closes much more quickly than the dura mater, so that cerebrospinal fluid leakage can no longer be detected. Wound closure with arachnoid tissue, however, does not offer sufficient protection against infection arising from the paranasal sinuses. Injuries of the anterior skull base are classified in various ways. Classification by the anatomic region involved (Fig. 6.3) can be made as shown in Table 6.1.
 Flowchart Injuries of the Skull Base, Chapter 3, p. 17.
Flowchart Injuries of the Skull Base, Chapter 3, p. 17.
 Treatment of Injuries of the Skull Base, Chapter 17, p. 140.
Treatment of Injuries of the Skull Base, Chapter 17, p. 140.
Surgical Anatomy
 ethmoid bone;
ethmoid bone;
 frontal bone;
frontal bone;
 sphenoid bone;
sphenoid bone;
 temporal bone;
temporal bone;
 occipital bone.
occipital bone.
Anterior Cranial Fossa
Middle Cranial Fossa
 The greater wings of the sphenoid bone (ala major) are two bony plates that descend from either side of the pituitary fossa to create part of the floor of the middle cranial fossa.
The greater wings of the sphenoid bone (ala major) are two bony plates that descend from either side of the pituitary fossa to create part of the floor of the middle cranial fossa.
 The lesser wings of the sphenoid bone (ala minor) travel horizontally toward the lateral cranial fossa.
The lesser wings of the sphenoid bone (ala minor) travel horizontally toward the lateral cranial fossa.
Posterior Cranial Fossa
Pathomechanism and Classification
Pathomechanism
Dural Injury
Classification of Fractures
Region I | Posterior wall of frontal sinuses |
Region II | Anterior cribriform plate of the ethmoid bone |
Region III | Posterior ethmoid |
Region IV | Sphenoid sinus |
Region V | Orbital roof |
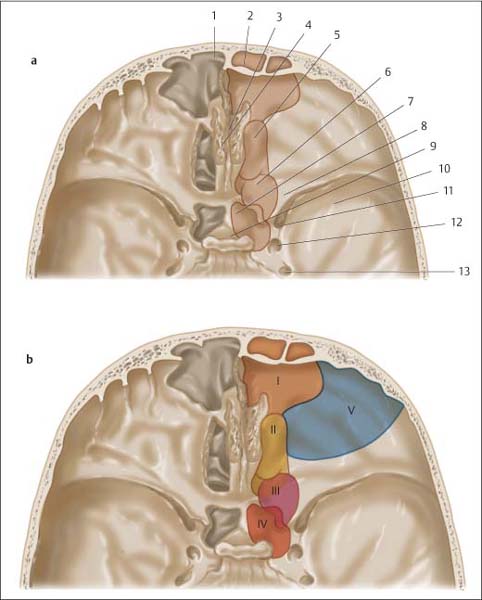
Fig. 6.3 Anterior skull base.
a Anatomy on a view of the paranasal sinuses. 1 Frontal sinus. 2 Posterior wall of the frontal sinus. 3 Crista galli. 4 Cribriform plate. 5 Anterior/middle ethmoid bone. 6 Posterior ethmoid bone. 7 Sphenoid sinus. 8 Lesser wing. 9 Pituitary fossa. 10 Middle cranial fossa (greater wing of sphenoid). 11 Superior orbital fissure. 12 Foramen rotundum. 13 Foramen ovale.
b Classification of anterior skull base fractures based on anatomic region (for regions I–V see Table 6.1, p. 47).
Clinical Signs and Symptoms
Symptoms of injury to the cranial base can be divided into clinically certain and uncertain signs (Table 6.2).
Uncertain Signs of Fracture of the Anterior Skull Base
Eyelid Hematoma, Eyelid Emphysema
Eyelid hematomas can arise from craniofacial injury or from injury of the orbital roof. There is unilateral or bilateral swelling of the upper lids and also blue discoloration in early stages. Swelling can obstruct or impair opening of the eyelid.
Uncertain signs | Certain signs |
Eyelid hematoma, eyelid emphysema | Cerebrospinal rhinorrhea |
Epistaxis | Pneumocephalus |
Seiferth sign | Early meningitis |
Olfactory disturbance | Extruding brain matter |
 Vision must be tested for any injury involving the region around the eye and eyelid. Instruments (eyelid hooks, etc.) should be used if necessary for opening the lids.
Vision must be tested for any injury involving the region around the eye and eyelid. Instruments (eyelid hooks, etc.) should be used if necessary for opening the lids.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


