Diabetic Retinopathy
MEDICAL ISSUES
Diabetes is increasing in prevalence in the American population for many reasons (1,2). Diabetics are living longer because of dialysis, kidney and pancreas transplants, improved cardiovascular management, and pharmacologic advances. The availability of high-calorie, high-carbohydrate, high-fat, and high-sugar foods; fast food restaurants; cultural attitudes toward eating; poor role models; large serving sizes; and many other factors contribute to the problem (3). Joslin observed that in 1912, there was no diabetes in the Pima Indian population; the incidence is now almost 70%. Friedman and others have attributed this to the “thrifty gene,” which enabled survival of man with “occasional” eating rather the three-square meals that many believe we should eat. It is of interest that beef, pork, egg, fast food, and dairy business interests support the nutrition community and make very large political donations. If dieticians, teachers, parents, doctors, nurses, ministers, and coaches eat improperly, there are no positive role models. The diabetic, antiatherosclerosis, anticancer, weight-loss, longevity, feel-good, look-good, and fitness diet are virtually the same. If the doctor eats properly, exercises, and educates the family and staff to do the same, a positive model is created for all. Everyone who comes into contact with the patient and family should support better health habits.
IMAGING
Fluorescein angiography was instrumental in understanding the stages in the pathogenesis of diabetic retinopathy and remains a valuable diagnostic tool to determine the extent and location of capillary nonperfusion, presence of neovascularization, and management of diabetic macular edema. The confocal, laser scanning, digital imager provides 15 dB better signal/background (contrast and resolution), eliminates the bright flash that increases patient comfort, and has a faster frame rate when compared to digital or film-based angiography systems. Better image quality is achieved because confocal imaging increases the image to background ratio via rejection of light scattered by the cornea, lens, and vitreous. In addition, lasers are more efficient in stimulating the fluorescein fluorophore than filtered noncoherent light. The use of contact wide-angle angiography lenses permits the diagnosis of preequatorial retinal neovascularization that was previously difficult to diagnose (Fig. 19.1).
Optical coherence tomography has not only allowed more precise diagnosis of diabetic macular edema but also permitted detailed observation of the vitreomacular interface and the presence of traction on the macular area that can be potentially relieved by vitrectomy surgery (Fig. 19.2).
SCREENING
Up to 70% of the known diabetic population in America does not get annual eye exams. Many studies have utilized various methods to screen this population as well as monitor patients with no retinopathy or preclinically significant macular edema (pre-CSME) nonproliferative diabetic retinopathy (NPDR) at their last exam. It appears that color images are somewhat more sensitive than monochrome. Digital cameras have decreased in cost while increasing in quality and have almost replaced standard film and Polaroid images. Nonmydriatic fundus cameras have proven to be very effective for diabetic screening. Screeners, optometrists, general ophthalmologists, and retinal specialists can evaluate the images, if properly trained.
RETINAL THICKNESS MEASUREMENT
Spectral domain ocular coherence tomography (OCT) (Heidelberg Spectralis or equivalent) is used to evaluate macular thickness in patients with NPDR. Although the studies demonstrated excellent sensitivity to macular edema, the real issue is whether it is beneficial to perform focal laser before CSME is present on clinical biomicroscopic examination. This issue will be addressed in the next section.
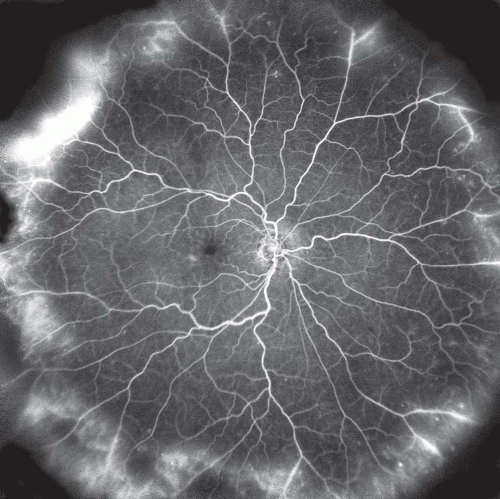 Figure 19.1 ▪ The Staurenghi 230 SLO lens permits angiography of preequatorial neovascularization. |
NONPROLIFERATIVE RETINOPATHY
The Early Treatment Diabetic Retinopathy Study (ETDRS) has contributed greatly to our management of patients with NPDR (4,5). The ETDRS defined CSME as (a) thickening of the retina at or within 500 μm of the center of the macula, (b) hard exudates at or within 500 μm of the center of the macula if associated with thickening of adjacent retina, or (c) an area of retinal thickening one disk diameter or larger, part of which is within one disk diameter of the center of the macula. It should be emphasized that the ETDRS was based on the clinical perception of macular edema. The majority of the physicians, including the authors, do not treat pre-CSME patients. Pre-CSME patients should probably be treated based on upcoming cataract surgery, poor result in the other eye, marked peripheral capillary nonperfusion, upcoming panretinal photocoagulation (PRP), or an estimation that the patient was unlikely to return for follow-up visits. Most surgeons use the Goldmann (flat) contact lens or macular lenses and start with a 60- to 100-μm, 100-milliwatts, and 20-to 30-ms spot. Many surgeons now use lighter treatment compared to the Diabetic Retinopathy Study (DRS) and ETDRS. Some surgeons primarily treat microaneurysms and microangiopathy noted to leak on angiography, others primarily use a light grid in the thickened, leaking area, and most treat both. Preferred lasers include argon green (514 nm), diode or flash tube-pumped diode lasers (532 nm), and krypton yellow (577 nm). Infrared (IR) diode (>800 nm) lasers are not recommended because of absorption in the choroid and pain. The authors prefer a 532-nm, diode-pumped, frequency up-converted continuous wave YAG laser on the PASCAL platform.
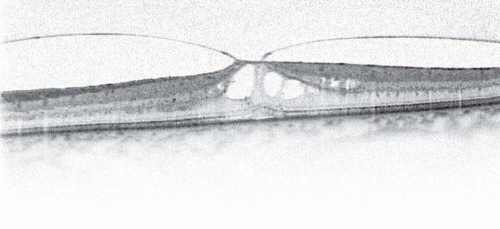 Figure 19.2 ▪ OCT image of vitreomacular traction in a diabetic eye. |
Pharmacotherapy of Diabetic Macular Edema: Corticosteroids
Since the introduction of intravitreal triamcinolone for the treatment of uveitic cystoid macular edema (6), it has become clear that steroids have a direct effect on the retinal vascular endothelium, decreasing leakage and restoring the blood retinal barrier. This discovery has led to the widespread use of intravitreal steroids for macular edema due to multiple causes, including diabetic retinopathy and retinal vein occlusions. Recent reports from the Intravitreal Steroid Injection Studies-Diabetic Macular Edema (7) (ISIS-DME) have shown that intravitreal injections of triamcinolone (Kenalog) result in significant visual improvement (three or more lines) in 38% of patients. Subgroup analysis revealed that 62% of patients with cystoid macular edema improved at least three lines of vision, whereas only 9% of those with noncystoid macular edema had a similar response. The macular edema recurred in approximately 50% of patients 6 months after the injection. Complications noted were steroid glaucoma in approximately a third of patients. Intravitreal steroids have other important complications in addition to steroid glaucoma. Posterior subcapsular cataract formation is a well-recognized complication of steroids and should be considered whenever injections are to be performed in phakic individuals. The authors do not use steroids in the management of diabetic macular edema because of the untenable steroid glaucoma and cataract rates.
The widespread use of intravitreal injections of steroids has been followed by various drug delivery systems that promise to prolong the release of steroids with slowrelease devices implanted in the vitreous. Currently, there are two types of drug delivery steroid implants in clinical trials: biodegradable implants (e.g., Osurdex dexamethasonepolyacticglycolic acid) and nonbiodegradable (e.g., Retisert fluocinolone implant). Both types of implants have potential advantages and disadvantages. Biodegradable implants have the advantage of requiring one implantation (that can be performed in the office with a 22-gauge injection applicator) but may have nonlinear release kinetics, whereas nonbiodegradable implants, although having linear release kinetics, require more complex surgical implantation and subsequent removal unless the implant is left in place. The Retisert clinical
trials reported a 90% incidence of steroid glaucoma and a 34% incidence of glaucoma filtering procedures. The risk/benefit and cost/benefit analyses of these implants in comparison with repeated intravitreal injections of triamcinolone suggest that the implants are too costly, in addition to causing an unacceptably high rate of steroid glaucoma and cataracts.
trials reported a 90% incidence of steroid glaucoma and a 34% incidence of glaucoma filtering procedures. The risk/benefit and cost/benefit analyses of these implants in comparison with repeated intravitreal injections of triamcinolone suggest that the implants are too costly, in addition to causing an unacceptably high rate of steroid glaucoma and cataracts.
Because of steroid glaucoma and steroid-induced cataracts, the authors do not use intravitreal steroids for diabetic macular edema and use a combination of anti-VEGF therapy (Avastin), PASCAL laser, and topical nonsteroidal agents (Nepafenac, Alcon).
Pharmacotherapy of Diabetic Macular Edema: Vascular Endothelial Growth Factor Antagonists
Macular edema is caused by vascular endothelial growth factor (VEGF) (8, 9, 10), the same agent that causes retinal neovascularization in diabetes and choroidal neovascularization in age-related macular degeneration. VEGF downregulates the tight junctions of the endothelium of the retinal vessels, causing breakdown of the blood-retinal barrier, and therefore leakage of fluid and macromolecules into the retinal intercellular space. Ischemia leading to VEGF production may be a factor in certain macular edema cases. For this reason, patients with macular edema not responding to direct focal treatment of leaking microaneurysms, or areas of leakage on fluorescein angiography, may respond to treating areas of ischemia. Heavy grid photocoagulation probably has little effect in reducing neovascularization but significantly reduces central visual fields and therefore reading speeds and often causes patients with excellent Snellen acuity to complain that they “cannot see.”
The introduction of anti-VEGF therapy has led to a new mode of therapy for macular edema secondary to NPDR as well as for venous occlusive disorders. Bevacizumab (Avastin) is an anti-VEGF antibody currently approved by the FDA for systemic therapy of cancer. Intravitreal Avastin is widely used for the treatment of choroidal neovascularization in age-related macular degeneration. Avastin is also being used for macular edema secondary to Branch Retinal Vein Occlusion (BRVOs) (11) and Central Retinal Vein Occlusion (CRVOs) as well as for retinal neovascularization in proliferative diabetic retinopathy (PDR). The initial published results as well as the authors’ results demonstrate that anti-VEGF therapy combined with laser should become standard therapy in the management of diabetic macular edema and PDR.
Management of Diabetic Macular Edema
The recent advances in pharmacotherapy and surgical therapy for diabetic macular edema, added to the well-known and time-proven approaches with laser photocoagulation, provide the clinician multiple therapeutic possibilities. Although there are no trials that clearly indicate which combination and sequence of therapies should be employed, the authors present their current perspective of management of diabetic macular edema, with the understanding that this protocol may change in the near future as clinical research is presented. Combination therapy is an appealing concept but is appropriate in some instances and not in others. Combination chemotherapy in oncology is utilized because the agents have narrow windows between effective and toxic drug levels as well as to provide multiple barriers to the evolution of cancer cells. Combination therapy for infectious disease is utilized in severe infections when the infectious agent has not been identified and delayed treatment would produce bad outcomes. Combination therapy for infectious disease creates multiple barriers for evolution of the infectious agent but unfortunately leads to higher incidence of resistance. Focal and/or PRP laser plus anti-VEGF therapy is very effective in diabetic retinopathy and can be broadly defined as combination therapy. Topical nonsteroidal (Nepafenac) therapy in combination with laser and anti-VEGF compounds is effective for diabetic macular edema because of multiple mechanisms, VEGF, and inflammation.
PROLIFERATIVE RETINOPATHY
The DRS randomized, multicenter clinical trial proved that PRP is effective for patients with PDR (12, 13, 14, 15). Many surgeons now treat before the DRS treatment criteria are reached (16), in part because of the subsequent ETDRS study data. The DRS criteria are based on high-risk characteristics as compared to standard photographs. The authors use light treatment with small spot size (100 to 200 μm), using 20- to 30-ms duration to reduce thermal diffusion, with the spots placed one spot size apart. Many surgeons treat using a very large number of intense, large, 100-ms duration spots and see the patient in follow-up in 3 months. Some of this behavior is unfortunately driven by the so-called global period for Medicare reimbursement. It is probably better practice to use a moderate number of spots and reexamine the patients in 1 month. Some surgeons have a protocol mindset with respect to PRP treatment. This approach may result in inappropriate vitrectomy or peripheral cryo when the “protocol has been completed” and active neovascularization is present.
It is better to perform PRP fill-in, combined with anti-VEGF therapy, if there is any neovascularization and the patient is greater than 1-month posttreatment. The authors believe that this combined, incremental approach to therapy reduces treatment-related complications and discomfort. If the patients present with florid neovascularization, it is better to use anti-VEGF therapy at the initial visit combined with PASCAL PRP. PRP with PASCAL using 30-ms, less intense burns does not destroy ischemic inner retina raising questions about efficacy, but studies have shown identical outcomes with less pain. The principal author points out that the destruction of RPE and photoreceptors results in transsynaptic degeneration of the bipolar, horizontal, amacrine, and ultimately ganglion cells similar to what occurs in
retinitis pigmentosa. Combining PASCAL PRP with Avastin combines the benefit of rapid response to Avastin with the durable response of PRP without the disadvantage of complications secondary to longer duration, more intense burns.
retinitis pigmentosa. Combining PASCAL PRP with Avastin combines the benefit of rapid response to Avastin with the durable response of PRP without the disadvantage of complications secondary to longer duration, more intense burns.
The authors virtually never use a retrobulbar block for laser treatment. Red and IR lasers cause more pain than 532-nm lasers. Durations greater than 30 ms cause more pain because of thermal diffusion; a duration of 30 ms on PASCAL is a better choice for PRP. Larger spot sizes and higher powers cause more pain, light scattering, and potentially more nuclear sclerosis and occult macular photic damage.
VITRECTOMY
Better medical management and laser photocoagulation should significantly reduce the need for vitrectomy for the complications of PDR. Vitrectomy, when indicated, has an excellent prognosis when appropriate patient selection and techniques are utilized (17).
CASE SELECTION
It is useful to divide blindness from diabetic retinopathy into two subgroups: those cases requiring immediate surgery and those in which surgery is elective. Traction retinal detachment (TRD) involving the macula (MTRD), neovascular glaucoma (NVG), and anterior vitreous cortex fibrovascular proliferation (AVCFVP) are permanently blinding if left untreated. By contrast, the visual potential probably does not change in the treatment of vitreous or preretinal hemorrhage if there is substantial delay before surgery is performed.
Vitreous Hemorrhage
Early experimental work incorrectly concluded that vitreous hemorrhage caused neovascularization via organization of the blood clot. Vitreous hemorrhage is a result of neovascularization rather than the cause. Although long-standing vitreous hemorrhage can deposit iron on many intraocular structures, there is usually no retinal damage from a vitreous hemorrhage. Retinal detachment, macular damage, ischemia, and optic nerve function will determine the ultimate visual outcome when long-standing vitreous hemorrhages are removed, not the hemorrhage per se.
If the other eye has good vision, a unilateral hemorrhage can be followed indefinitely with ultrasound, unless retinal detachment, anterior vitreous cortex (AVC) neovascularization, or iris neovascularization occurs. An eye without prior PRP is at greater risk for the development of neovascular complications and must be watched more closely. B-scan ultrasonography should be repeated at each visit, preferably at 1-month intervals until the blood clears or surgery is performed. Ultrasonic evidence of posterior pole detachment requires immediate vitrectomy. The usual question of duration of a vitreous hemorrhage plays a less important role in the surgical decision-making process than other factors. If it does not appear that near-term clearing will occur, bilateral hemorrhage requires surgery on the eye with the best visual prognosis. Vitreous hemorrhage in a patient with only one eye as well as the better eye of bilateral cases should be operated on to improve visual function. Those patients with shortened lifespan and multisystem disease need immediate visual rehabilitation for emotional and social reasons. Subposterior vitreous detachment and preretinal hemorrhages clear more rapidly than does hemorrhage in the vitreous cortex. For this reason, patients with bilateral or only-eye sub-PVD or preretinal hemorrhage can be followed up for as long as the patient’s emotional and social needs permit. If one eye has macular ischemia and the other, better, eye develops a vitreous hemorrhage, vitrectomy may be indicated to improve the patient’s overall visual function.
Traction Retinal Detachment
TRD can be diagnosed by ophthalmoscopic or ultrasonic examination. If the macula is detached, vitreous surgery should be performed within 3 weeks, unless there are medical contraindications. If there is active neovascularization, it is better to perform PRP before vitrectomy if possible. Because of extensive exudation and fibrous proliferation, panretinal cryopexy should not be utilized. If vitrectomy indications are present, endo-PRP can be combined with vitrectomy. If vitrectomy is postponed until PRP-induced or spontaneous involution of neovascularization occurs, the incidence of postoperative NVG and AVCFVP is dramatically reduced.
Recent studies demonstrate that intravitreal anti-VEGF therapy with bevacizumab can precipitate TRDs in patients with severe neovascularization (18). These patients should be followed closely after anti-VEGF therapy and the surgeon should be ready to proceed to vitrectomy if progression to TRD is evidenced.
Because of the relatively high rate of biologic complications and medical risk factors, vitrectomy is not indicated in extramacular TRD. This is true even if progression toward the macula or a similar condition in the other eye seems to “threaten” the macula. It is safer to operate on actual, rather than predicted, visual loss. The rate of progression of extramacular TRD to include the macula is about 15% per year (19,19a,20). After several years, progression to MTRD stabilizes at a cumulative rate of about 30%, and there are many patients with 5 to 10 years duration extramacular TRDs surrounding the macula with good vision that never required surgery.
Cataract surgery can result in anterior movement of the vitreous with progression of extramacular TRD to macular involvement. Once again, vitreous surgery should only be performed if the macula actually becomes elevated (21).
MACULAR EDEMA, CYSTS, AND SUBMACULAR EXUDATES
Hilel Lewis et al. first reported vitrectomy with peeling of taut posterior vitreous cortex (PVC) from diffuse macula edema (DME) eyes not responsive to focal laser photocoagulation. SD OCT is very effective at determining the presence of vitreoretinal traction and measuring macular thickness. Many surgeons now believe that vitrectomy in DME cases without vitreomacular traction can reduce macular edema similar to the observations in vitrectomy without branch vein decompression for BRVO and vitrectomy without radial optic neurotomy in CRVO. The principal author has postulated that vitrectomy or separation of the PVC could allow greater egress of VEGF, known to be causative of macular edema. Steffanson and later Holekamp have shown that vitrectomy produces higher oxygenation in the vitreous cavity (22), which may improve macular edema as well. Peeling of the internal limiting membrane can improve diabetic macular edema and should be considered in patients who are resistant to laser and pharmacologic treatment (23). Some surgeons have reported removal of submacular exudates or draining macular cysts, but there is scant evidence of efficacy for either procedure at this time and some concern about retinal damage caused by the procedures.
CONTRAINDICATIONS
The absence of light perception indicates glaucomatous optic atrophy, ischemic optic neuropathy, or extensive retinal vascular occlusive disease and contraindicates vitreous surgery. Corneal opacity; corneal, lid, or conjunctival infection; and the inability to withstand local anesthesia are relative contraindications.
Iris neovascularization can be an indication for surgery in diabetic TRDs (24, 25, 26). Intravitreal bevacizumab has been shown by the authors to cause regression of anterior segment neovascularization and revert the progression toward NVG (27). Anti-VEGF therapy for NVG requires permanent control of VEGF production through retinal reattachment and PRP. Vitrectomy in an aphakic eye with active iris neovascularization will result in rapid progression of postoperative NVG unless intravitreal bevacizumab and PRP are performed preoperatively and intraoperatively.
Cases of several years’ duration may exhibit extensive white vessels and retinal atrophy. If the temporal arcades are not perfusing the macula, there is no need for vitreous surgery because visual improvement will not occur. If the retina is extremely atrophic but PRP has not previously been performed, this is an indication that limited visual improvement will occur from reattachment. There are, however, cases of 3 to 4 years’ duration that have improved to ambulatory vision levels after vitrectomy. Late cases with atrophic retina producing little VEGF have a lesser incidence of NVG and AVCFVP.
SURGICAL SEQUENCE AND TECHNIQUES
Vitreous surgery for hemorrhage or TRD requires a planned sequence of surgical steps, with multiple branches depending on different intraoperative scenarios. As in all vitreous surgery, a full complement of sterile tools and materials must be immediately available.
Anesthesia
The frequency of cardiovascular and renal disease in the diabetic patient requires careful preoperative evaluation by the primary care physician or internist and utilization of cardiologists, endocrinologists, and other consultants as needed. The anesthesiologist should review the preoperative medical evaluation. Diabetic vitrectomies can be performed in the ambulatory surgery center setting if systemic disease is stable, an anesthesiologist is available and the patients systemic specialists (nephrologists, cardiologists) give adequate consent for surgery. Patients that are not controlled systemically and require vitrectomy surgery that cannot be delayed should be operated in a hospital outpatient setting. It is essential to have MD anesthesia function in an immediate availability and supervisory role if CRNA anesthesia is utilized. Proximity to the hospital ensures availability of cardiologists, endocrinologists, pulmonary specialists, and intensive care facilities as well as providing higher facility fees than free-standing ambulatory surgery centers, thereby facilitating access to best technology. An intravenous line, EKG, pulse oximetry, blood pressure monitoring, and oxygen mask with suction hose to prevent hypercapnia must be utilized in all cases. The anesthesiologist or nurse anesthetist should make liberal use of intraoperative serum glucose monitoring. Operating times are always less than 1 hour and usually about 30 minutes, which is compatible with local anesthesia and the associated reduction in nausea, vomiting, and medical complications of general anesthesia. Minimal, if any, sedation is used after the block, which is performed with a 27-gauge, 1.25-inch needle at the outer “corner” of the orbit.



