Purpose
To develop and validate grading scales for meibomian gland dysfunction (MGD) that allow consistent diagnosis of MGD and are suitable for clinical studies.
Design
Development and validation study of grading scales.
Methods
Lid margin and meibomian gland photographs were taken in the multicenter, prospective cross-sectional study for MGD and control subjects. New grading scales for MGD signs (abnormal lid margin findings of vascularity, plugging of gland orifices, lid margin irregularity, lid margin thickening, partial glands, and gland dropout) in both upper and lower eyelids were developed. Three MGD experts, 3 general ophthalmologists, and 3 non-physicians independently tested the scales by evaluating photographs. The levels of interrater and intrarater agreement for each grading scale were estimated with the use of kappa statistics.
Results
Thirty-eight patients with MGD and 20 control subjects were enrolled and photographed. New grading scales were developed using a total of 226 photographs. The interrater kappa values for MGD experts and for general ophthalmologists and non-physicians with reference to an MGD expert ranged from 0.36 to 0.87 (median of 0.66), 0.41 to 0.73 (0.60), and 0.30 to 0.77 (0.59), respectively. Those for intrarater reliability for 2 MGD experts ranged from 0.49 to 0.93 (0.82).
Conclusions
New grading scales for MGD signs were developed and found to have appropriate inter- and intrarater reliabilities for grading MGD. These grading scales are suitable for MGD diagnosis and application to multicenter trials.
The tear film that covers the ocular surface is protected from evaporation by a thin layer of lipid secreted by the meibomian glands. Meibomian gland dysfunction (MGD) is one of the most common disorders encountered in ophthalmic clinics and is now recognized as a major cause of dry eye syndrome. It can result in tear film instability, damage to the ocular surface epithelium, chronic blepharitis, and contact lens intolerance. MGD is commonly characterized by a chronic, diffuse abnormality of meibomian glands, terminal duct obstruction, and qualitative or quantitative changes in the glandular secretion. The key signs of MGD are meibomian gland dropout, altered meibomian gland secretion, and changes in morphology of the lid margin. The lid margin abnormalities may become detectable with a slit-lamp microscope as the disease progresses. Lid margin findings and meibomian gland morphology are therefore important for diagnosis of MGD. Diagnosis and quantification of MGD thus require assessment of symptoms, altered meibomian gland secretion, changes in lid morphology, and meibomian gland dropout. Evaluation of meibomian gland expressibility as a dynamic process is also important. Assessment of the efficacy of treatment for MGD requires precise evaluation of changes in lid morphology, meibomian gland dropout, and meibomian gland expressibility. The ability to perform an objective evaluation of MGD based on photographs would be useful as a standardized procedure for multicenter clinical trials.
Grading scales for diagnosis of MGD have been proposed and adopted in clinical practice. These scales are based on assessment of lid margin findings or of meibomian glands, with the latter scales being based on the proportion of meibomian glands showing dropout in only the lower tarsal plate or on the number of whole glands and proportion of partial glands. The application of these existing scales to the clinic is difficult, however, because there are many grading subdivisions for each sign or their targets are limited to the lower eyelids. Moreover, information on grading reliability has been available for only a few scales. There is thus still an unmet need for reliable and widely adoptable grading scales based on evaluation of both upper and lower eyelids for the consistent diagnosis of MGD.
We have now developed new grading scales for MGD that can be used by ophthalmologists without special experience, and we have performed a validation study to confirm the robustness of these scales. We propose that these grading scales are suitable for the diagnosis of MGD or for its evaluation in clinical studies.
Methods
Study Design and Target Population
This study was conducted at The University of Tokyo Hospital, Itoh Clinic (Saitama City, Saitama, Japan), and Maeda Ophthalmic Clinic (Aizuwakamatsu City, Fukushima, Japan). MGD patients and control subjects were randomly enrolled from outpatients who visited the 3 medical facilities from December 4, 2012 to December 7, 2013. The study adhered to the tenets of the Declaration of Helsinki and was prospectively approved by the Institutional Review Board of Tokyo University School of Medicine. All subjects provided written informed consent before entry into the study.
The MGD patients were aged ≥20 years and were diagnosed on the basis of previously described criteria : (1) at least 1 symptom, such as ocular fatigue, discharge, foreign body sensation, dryness, uncomfortable sensation, sticky sensation, pain, epiphora, itching, redness, heavy sensation, glare, excessive blinking, burning sensation, and ocular discomfort on arising; (2) at least 1 abnormal lid margin finding, such as vascular engorgement, anterior or posterior replacement of the mucocutaneous junction, and irregular lid margin; and (3) plugged meibomian gland orifices and poor meibum expressibility in the target eye. The control subjects had never been diagnosed with blepharitis or MGD, were aged ≥20 years, and had no history of contact lens wear or eye surgery. Individuals with severe systemic illness or with squamous cell debris (collarette) around the base of the eyelashes were excluded.
Clinical Assessment and Image Collection
One eye was selected as the target eye in each subject. Complications, history of contact lens wear or eye surgery, the presence of ocular allergy, and concomitant medications were noted as background information. The subjects were assessed for lid margin and meibomian gland findings, as well as for their experience of subjective symptoms.
Lid margin findings were evaluated for the upper and lower eyelids with the use of a slit-lamp microscope. Telangiectasia was assessed on a scale from 0 to 3: 0 = no findings; 1 = mild telangiectasia; 2 = moderate telangiectasia or redness; 3 = severe telangiectasia or redness. Mucocutaneous junction was assessed on a scale from 0 to 3: 0 = Marx line (ML) courses on the skin side of the meibomian orifice (MO) line and does not touch MOs at all; 1 = parts of ML touch MOs; 2 = ML courses through MOs; 3 = ML courses along the eyelid margin side of MOs. Irregularity, plugging, foaming, and thickness were assessed on a scale from 0 to 2: 0 = no findings; 1 = mild findings; 2 = severe findings.
Corneal and conjunctival staining were scored from 0 to 9. The tear film breakup time (BUT) was measured 3 times consecutively after the instillation of fluorescein, and the mean value was adopted. Tear fluid production was evaluated with the Schirmer test without anesthesia.
Meibomian glands were evaluated for the upper and lower lids with the use of a noncontact meibography system attached to a slit-lamp microscope. Partial or complete loss of meibomian glands was scored on a scale from 0 to 3 (meiboscore), as described previously. The extent of meibomian gland dropout was determined on a scale from 0 to 2 based on the number of affected glands: 0 = none; 1 = small number; 2 = large number.
The degree of ease with which meibum could be expressed at the central area of both upper and lower eyelid was evaluated semiquantitatively on a scale from 0 to 3: 0 = clear meibum readily expressed; 1 = cloudy meibum expressed with mild pressure; 2 = cloudy meibum expressed with more than moderate pressure; 3 = meibum could not be expressed even with strong pressure.
Images of lid margins and orifices of meibomian glands at the upper and lower eyelids of 1 eye were obtained with a digital camera and meibography system attached to a slit-lamp microscope (SL-D701 DC4 BG-5; Topcon Japan, Tokyo, Japan). The images of the lid margins and those of meibomian glands were both acquired at 10× magnification for the full length of each eyelid within a single photograph. Four images (2 of each eyelid) were collected for each subject.
New Grading System
We developed grading scales for MGD with the use of printed images. All images were acquired by an ophthalmologist (R.A. or R.S.) with a specialty in MGD. Four signs for lid margin findings detected with a slit-lamp microscope and 2 signs of meibomian glands detected by meibography were selected for development of the grading scales. Three MGD experts (R.A., R.S., and S.F.), each participating at a different institution, developed draft grading scales for MGD with key conceptual components based on morphologic and anatomic criteria described in previous reviews. These draft grading scales were then evaluated with a preliminary validation test in which each of the 3 MGD experts classified the printed images independently according to the draft scales, and the consistency for each scale was determined. The 3 experts then reviewed the results and adjusted the grading scales accordingly. The 3 experts then reviewed the results and adjusted the grading scales accordingly with the advice of another expert. The final versions proceeded to the validation test as the proposed grading scales.
Validation Testing
Validation testing was performed to evaluate the robustness of the proposed grading scales after an interval of >2 weeks since their development. The raters received printed images of the upper and lower eyelids of the original 58 subjects together with printed grading scales and representative images. Each printed image had a randomly assigned number for analysis. Raters individually classified each image according to the grading scales. The test was performed by each rater at a separate site. After the test, the assigned numbers of the classified images for each grading scale were recorded for statistical analysis.
Interrater and intrarater reliability
Three MGD experts (R.A., R.S., and S.F.) performed the validation test, and consistency among their results for each grading scale was evaluated.
Two of the MGD experts who participated in the determination of interrater reliability (R.A. and S.F.) performed the test a second time after an interval of >2 weeks. Consistency between the results of the first and second tests for each grading scale was evaluated.
Effect of clinical experience
Three general ophthalmologists (non–MGD experts) who had been certified for 3, 5, or 8 years, as well as 3 non-physicians, also performed the validation test. An introduction and explanation of the grading scales were given before the test by an MGD expert (R.A.). Consistency between the results for each group of raters and those for an MGD expert (first test performance by R.A.) was evaluated as interrater reliability.
Additional validation
For confirmation of the intrarater and interrater reliability of the grading scales, 2 MGD experts (N.M. and Tohru Sakimoto [Nihon University]) who did not contribute to their development performed the validation test as described above but with images of the upper and lower eyelids of 18 additional MGD patients that were not used for scale development. Those images of additional MGD patients were obtained at Itoh Clinic.
Diagnostic Ability of the Proposed Grading Scales
For evaluation of the diagnostic ability of the proposed grading scales, the MGD patients and control subjects were classified on the basis of the validation test results for an MGD expert (first test performance by R.A.). The total score of the upper and lower eyelids was used for the calculation. Receiver operating characteristic (ROC) curves and the area under the curve (AUC) were calculated for each grading scale.
Statistical Analysis
Data were collected into an Excel 2010 worksheet and were analyzed with the use of SAS version 9.2 software (SAS Institute, Cary, North Carolina, USA). Weighted kappa values and 95% confidence intervals (CIs) for each grading scale were calculated to evaluate consistency in test performance. Median values were used to summarize the results for weighted kappa values for each test.
Results
Thirty-eight MGD patients (13 men and 25 women; mean age ± SD, 66.9 ± 15.0 years) and 20 control subjects (8 men and 12 women; 64.5 ± 6.7 years) were eventually enrolled. All subjects underwent clinical assessment and image collection, and their clinical characteristics are shown in Table 1 .
| Characteristic | Controls (N = 20) | Initial MGD Patients (N = 38) | Additional MGD Patients (N = 18) |
|---|---|---|---|
| Sex (male/female) | 8/12 | 13/25 | 8/10 |
| Age (y) | 64.5 ± 6.7 | 66.9 ± 15.0 | 69.1 ± 13.2 |
| BUT (s) | 6.5 ± 1.6 | 3.4 ± 2.1 | 2.7 ± 1.1 |
| Schirmer test value (mm) | 16.4 ± 9.9 | 10.6 ± 7.2 | 7.9 ± 3.7 |
| Corneal staining score a | 0.0 ± 0.0 | 0.5 ± 0.6 | 0.8 ± 0.4 |
| Conjunctival staining score b | 0.0 ± 0.0 | 0.3 ± 0.6 | 0.4 ± 0.5 |
| Telangiectasia c | |||
| Upper | 0.1 ± 0.3 | 1.7 ± 0.9 | 1.8 ± 0.9 |
| Lower | 0.1 ± 0.2 | 1.3 ± 0.8 | 1.3 ± 0.6 |
| Plugging d | |||
| Upper | 0.1 ± 0.2 | 1.3 ± 0.7 | 1.5 ± 0.5 |
| Lower | 0.0 ± 0.0 | 1.0 ± 0.7 | 1.1 ± 0.4 |
| Meiboscore e | |||
| Upper | 0.4 ± 0.5 | 1.9 ± 0.8 | 2.0 ± 0.8 |
| Lower | 0.2 ± 0.4 | 1.9 ± 0.9 | 1.6 ± 0.8 |
| Meibum grade f | |||
| Upper | 0.1 ± 0.4 | 1.5 ± 0.9 | 1.6 ± 0.5 |
| Lower | 0.2 ± 0.5 | 1.6 ± 0.7 | 1.4 ± 0.6 |
| Gland dropout g | |||
| Upper | 0.1 ± 0.3 | 1.1 ± 0.8 | 2.0 ± 0.8 |
| Lower | 0.0 ± 0.0 | 1.1 ± 0.8 | 1.7 ± 0.8 |
a Corneal staining was scored 0-3 for the entire cornea.
b Conjunctival staining was scored 0-3 for each of the nasal and temporal conjunctiva and then summed.
c Telangiectasia was assessed on a scale of 0-3.
d Plugging was assessed on a scale of 0-2.
e Partial or complete loss of meibomian glands was scored 0-3 (meiboscore).
f Meibum grade was scored 0-3.
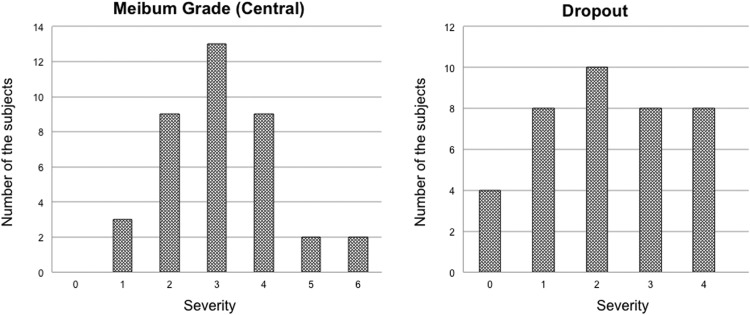
For the MGD patients, lid margin and meibomian gland findings encompassed the range of severity levels and appeared to reflect the distribution of findings encountered in the clinic ( Table 2 , Figure 1 ). For the control subjects, almost all findings were normal ( Table 2 ). With the exception of 6 missing images, 4 images acquired from each subject (total of 226 images) were used to develop the new grading system.
| Parameter | MGD Patients (N = 38) | Controls (N = 20) | ||
|---|---|---|---|---|
| Upper | Lower | Upper | Lower | |
| Telangiectasia | ||||
| 0 | 3 (7.9) | 4 (10.8) | 17 (89.5) | 18 (94.7) |
| 1 | 14 (36.8) | 21 (56.8) | 2 (10.5) | 1 (5.3) |
| 2 | 14 (36.8) | 8 (21.6) | 0 (0) | 0 (0) |
| 3 | 7 (18.4) | 4 (10.8) | 0 (0) | 0 (0) |
| Missing data | 0 | 1 | 1 | 1 |
| Mucocutaneous junction | ||||
| 0 | 3 (8.3) | 4 (11.8) | 18 (94.7) | 18 (94.7) |
| 1 | 12 (33.3) | 12 (35.3) | 1 (5.3) | 1 (5.3) |
| 2 | 11 (30.6) | 12 (35.3) | 0 (0) | 0 (0) |
| 3 | 10 (27.8) | 6 (17.6) | 0 (0) | 0 (0) |
| Missing data | 2 | 4 | 1 | 1 |
| Irregularity | ||||
| 0 | 22 (57.9) | 19 (50.0) | 18 (94.7) | 18 (94.7) |
| 1 | 14 (36.8) | 14 (36.8) | 1 (5.3) | 1 (5.3) |
| 2 | 2 (5.3) | 5 (13.2) | 0 (0) | 0 (0) |
| Missing data | 0 | 0 | 1 | 1 |
| Plugging | ||||
| 0 | 5 (13.2) | 9 (23.7) | 18 (94.7) | 19 (100) |
| 1 | 18 (47.4) | 21 (55.3) | 1 (5.3) | 0 (0) |
| 2 | 15 (39.5) | 8 (21.1) | 0 (0) | 0 (0) |
| Missing data | 0 | 0 | 1 | 1 |
| Foaming | ||||
| 0 | 37 (97.4) | 34 (91.9) | 19 (100) | 19 (100) |
| 1 | 1 (2.6) | 2 (5.4) | 0 (0) | 0 (0) |
| 2 | 0 (0) | 1 (2.7) | 0 (0) | 0 (0) |
| Missing data | 0 | 1 | 1 | 1 |
| Thickness | ||||
| 0 | 29 (76.3) | 30 (78.9) | 19 (100) | 19 (100) |
| 1 | 7 (18.4) | 7 (18.4) | 0 (0) | 0 (0) |
| 2 | 2 (5.3) | 1 (2.6) | 0 (0) | 0 (0) |
| Missing data | 0 | 0 | 1 | 1 |
| Meiboscore | ||||
| 0 | 1 (2.7) | 0 (0) | 12 (60.0) | 16 (80.0) |
| 1 | 11 (29.7) | 15 (40.5) | 8 (40.0) | 4 (20.0) |
| 2 | 17 (45.9) | 10 (27.0) | 0 (0) | 0 (0) |
| 3 | 8 (21.6) | 12 (32.4) | 0 (0) | 0 (0) |
| Missing data | 1 | 1 | 0 | 0 |
New Grading System
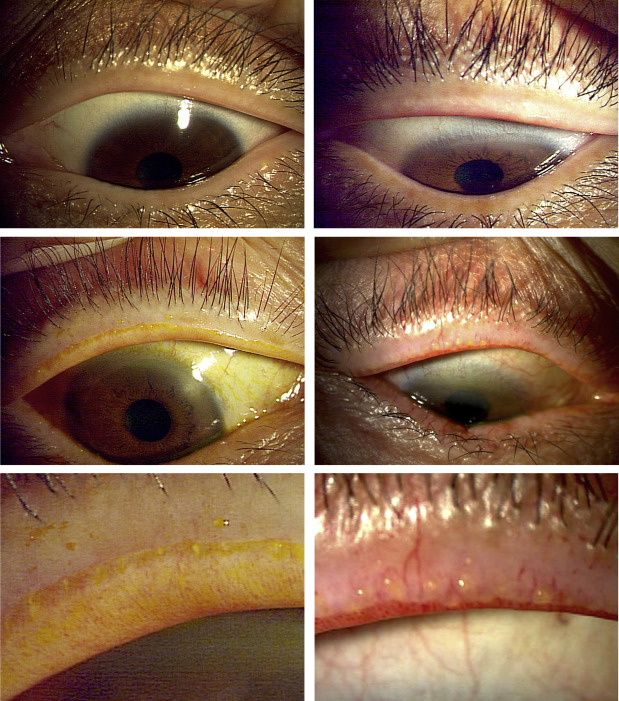
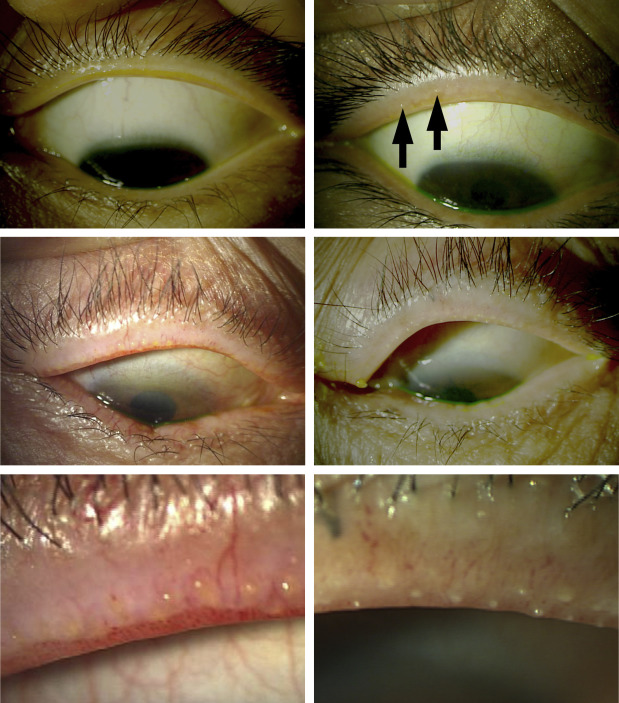
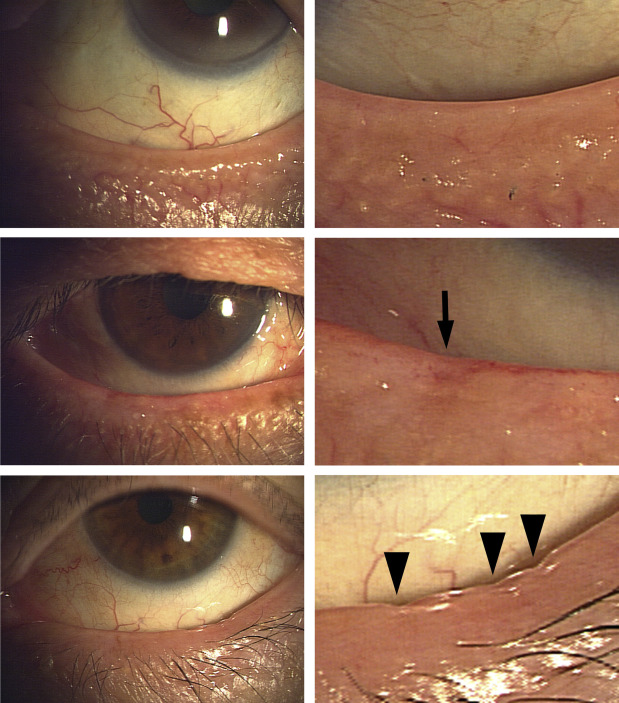
We developed 6 grading scales for MGD based on images of the upper and lower eyelids of 38 MGD patients and 20 control subjects ( Table 3 , Supplemental Figure ; Supplemental Material available at AJO.com ). Abnormal lid margin findings of vascularity ( Figure 2 ), plugging of gland orifices ( Figure 3 ), lid margin irregularity ( Figure 4 ), and lid margin thickening ( Figure 5 ) were evaluated in the full-length images of each eyelid obtained with a slit-lamp microscope. Partial glands ( Figure 6 ) and gland dropout ( Figure 7 ) were evaluated by noncontact meibography for meibomian glands in the middle two-thirds of each eyelid, given that it is difficult to capture and examine glands at the ends of each eyelid in a single photograph ( Figure 6 ).
| Abnormal Lid Margin Findings of Vascularity |
| 0 = No or slight redness in lid margin conjunctiva and no telangiectasia crossing meibomian gland orifices |
| 1 = Redness in lid margin conjunctiva and no telangiectasia crossing meibomian gland orifices |
| 2 = Redness in lid margin conjunctiva and telangiectasia crossing meibomian gland orifices with a distribution of less than half of the full length of the lid |
| 3 = Redness in lid margin conjunctiva and telangiectasia crossing meibomian gland orifices with a distribution of half or more of the full length of the lid |
| Plugging of Gland Orifices |
| 0 = No plugging of gland orifices |
| 1 = Fewer than 3 pluggings of gland orifices |
| 2 = Three or more pluggings of gland orifices with a distribution of less than half of the full length of the lid |
| 3 = Three or more pluggings of gland orifices with a distribution of half or more of the full length of the lid |
| Lid Margin Irregularity |
| 0 = No lid margin irregularity |
| 1 = Fewer than 3 lid margin irregularities with shallow notching |
| 2 = Three or more lid margin irregularities or deep notching |
| Lid Margin Thickening |
| 0 = No lid margin thickening |
| 1 = Lid margin thickening with or without localized rounding |
| 2 = Lid margin thickening with diffuse rounding |
| Partial Glands |
| 0 = No partial glands |
| 1 = Fewer than 3 partial glands |
| 2 = Three or more partial glands and fewer than 3 partial glands with loss of half or more of the full length |
| 3 = Three or more partial glands with loss of half or more of the full length |
| Gland Dropout |
| 0 = No gland dropout |
| 1 = Fewer than 3 gland dropouts |
| 2 = Three or more gland dropouts |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


