Purpose
To develop a score along with an estimated probability of disease for detecting angle closure based on anterior segment optical coherence tomography (AS OCT) imaging.
Design
Cross-sectional study.
Methods
A total of 2047 subjects 50 years of age and older were recruited from a community polyclinic in Singapore. All subjects underwent standardized ocular examination including gonioscopy and imaging by AS OCT (Carl Zeiss Meditec). Customized software (Zhongshan Angle Assessment Program) was used to measure AS OCT parameters. Complete data were available for 1368 subjects. Data from the right eyes were used for analysis. A stepwise logistic regression model with Akaike information criterion was used to generate a score that then was converted to an estimated probability of the presence of gonioscopic angle closure, defined as the inability to visualize the posterior trabecular meshwork for at least 180 degrees on nonindentation gonioscopy.
Results
Of the 1368 subjects, 295 (21.6%) had gonioscopic angle closure. The angle closure score was calculated from the shifted linear combination of the AS OCT parameters. The score can be converted to an estimated probability of having angle closure using the relationship: estimated probability = e score /(1 + e score ), where e is the natural exponential. The score performed well in a second independent sample of 178 angle-closure subjects and 301 normal controls, with an area under the receiver operating characteristic curve of 0.94.
Conclusions
A score derived from a single AS OCT image, coupled with an estimated probability, provides an objective platform for detection of angle closure.
Primary angle-closure glaucoma accounts for approximately 50% of people with bilateral glaucoma blindness worldwide, with significant impact on individuals, societies, and health care systems. Identifying people with the early asymptomatic stages of the disease may allow for prophylactic treatment by laser iridotomy to prevent visual loss. Therefore, it is desirable to augment the efficiency and effectiveness of screening practices above and beyond the current approaches.
Anterior segment optical coherence tomography (AS OCT) technology enables the acquisition and visualization of high-resolution images of the anterior segment (AS) structures in vivo. Recently, several novel AS OCT parameters have been associated with angle closure, including smaller anterior chamber width, area, and volume ; greater iris thickness, curvature, and area ; and a larger lens vault. In addition to their individual association with angle closure, it was shown recently that more than 80% of the variation in angle width is explained by these newly identified risk factors, with lens vault, anterior chamber area, and volume being the most important determinants.
We recently evaluated the diagnostic ability of a range of biometric, demographic, and AS OCT-based parameters to detect angle closure. A stepwise logistic regression model with a variable set consisting of just 6 AS OCT-derived parameters—namely, lens vault; anterior chamber width, area, and volume; iris thickness; and iris area—had a high diagnostic capability with an area under the receiver operating characteristic curve (AUC) of more than 0.95 in identifying eyes with gonioscopic angle closure. We believe that these findings can be useful in developing a feasible, imaging-based tool for the detection of eyes with angle closure.
The purpose of this study was to develop an angle-closure score and probability estimate based on AS OCT imaging that would allow for objective identification of eyes with gonioscopic angle closure. As a secondary aim, we wanted to dissect out the contribution of the various anatomic factors imaged by AS OCT to identify the likely mechanism(s) contributing to angle closure.
Methods
Approval for the study was granted by the Singapore Eye Research Institute Institutional Review Board. The study was conducted in accordance with the tenets of the Declaration of Helsinki, and written informed consent was obtained from all subjects before enrolment into the study. Analysis was performed on data collected from a community-based cross-sectional study performed in Singapore, the details of which have been described previously. In brief, the subjects for the study were recruited from a government-run community-based clinic facility that provides primary health care services for local residents. The study participants were 50 years of age and older.
Examination and Definition of Gonioscopic Angle Closure
All study participants underwent a standardized eye examination that included measurements of visual acuity using a logarithm of the minimal angle of resolution chart (Lighthouse, Inc, Long Island, New York, USA), slit-lamp examination (Model BQ 900; Haag-Streit, Bern, Switzerland), stereoscopic optic disc examination with a 78-diopter lens (Volk Optical, Inc, Mentor, Ohio), measurement of intraocular pressure by Goldmann applanation tonometry (Haag-Streit, Koniz, Switzerland), and gonioscopy performed in the dark using a Goldmann 2-mirror lens at high magnification (×16) by a single examiner.
An eye was considered to have gonioscopic angle closure if the posterior pigmented trabecular meshwork was not visible for at least 180 degrees on nonindentation gonioscopy with the eye in the primary position. Axial length and anterior chamber depth (ACD) were measured using partial coherence laser interferometry by IOLMaster (Carl Zeiss Meditec, Dublin, California, USA).
Anterior Segment Optical Coherence Tomography Imaging
AS OCT images were acquired from all participants in dark room conditions by a single operator. Each scan was centered on the pupil, and a single cross-sectional horizontal scan (nasal-temporal angles at 0 degrees and 180 degrees) was evaluated for each subject. The best-quality images were obtained by adjusting the saturation and noise and by optimizing the polarization for each scan during the examination. A customized software, the Zhongshan Angle Assessment Program (Guangzhou, China), was used to process the AS OCT images. For each image, the only observer input was to determine the location of the 2 scleral spurs, which is described as the inward protrusion of the sclera with a change in curvature of its inner surface. The algorithm then automatically calculated the various AS parameters. The reproducibility of the AS parameters was excellent, with the intraclass correlation coefficient ranging from 0.88 to 0.97.
Definition of Anterior Segment Optical Coherence Tomography Parameters
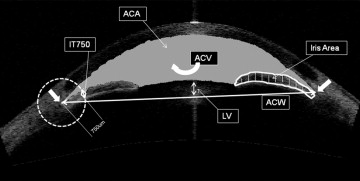
The parameters as measured by AS OCT ( Figure 1 ) were defined as follows. Anterior chamber width was defined as the horizontal scleral spur-to-spur distance (in millimeters), and lens vault was the perpendicular distance between the anterior pole of the crystalline lens and the horizontal line joining the 2 scleral spurs (in micrometers). The iris thickness was measured at 750 and 2000 μm from the scleral spur. The iris area was calculated as the cross-sectional area of the full length (from spur to pupil) of the iris (in square millimeters). To determine iris curvature, the software draws a line from the most peripheral to the most central points of the iris pigment epithelium. A perpendicular line then is extended from this line to the iris pigment epithelium at the point of greatest convexity. The length of this perpendicular line is a measure of the iris curvature (in millimeters). The anterior chamber area was defined as the cross-sectional area (in square millimeters) of AS bounded by the corneal endothelium, the anterior surface of the iris, and the anterior surface of the lens (within the pupil). To assess anterior chamber volume, the algorithm first plots a vertical axis through the midpoint (center) of the anterior chamber area, and by rotating the anterior chamber area 360 degrees around this vertical axis, the anterior chamber volume was calculated (in cubed millimeters).
Statistical Analysis
Development of the angle closure score and estimated probability
Data from right eyes were used for analysis. After an evaluation of the diagnostic accuracy of several classification algorithms to detect gonioscopic angle closure, we found that the stepwise logistic regression model with Akaike information criterion consisting of only 6 AS OCT parameters was both the most accurate and least variable. Akaike information criterion measures both the accuracy and complexity of a model, and in the context of a given problem, a model with lower Akaike information criterion often will have better generalizability. Stepwise logistic regression was begun with none of the 6 variables in the model. At each stage, the possibilities of (1) adding each variable not yet included, (2) removing each of the currently included variables, and (3) leaving the model unchanged were considered in turn. The action with minimum Akaike information criterion was taken with the algorithm terminating when leaving the model unchanged had minimum Akaike information criterion. The logistic regression yields a score that is a shifted linear combination of the selected variables. This score can be converted to an estimated probability of angle closure using the relationship: estimated probability = e score /(1 + e score ), where e is the natural exponential.
Determination of the relative contributions of the anterior segment optical coherence tomography parameters and their graphical representation
An assessment of the relative contributions of the variables to the angle closure score for a given subject was achieved first by standardizing each of the variables, so that each had a mean of 0 and a standard deviation of 1. This was achieved by subtracting each variable’s mean and then dividing each variable by its standard deviation. Then, the shifted linear combination of selected variables that constitutes the score was re-expressed in terms of the standardized variables. For a particular subject and their standardized variable values, the product of each standardized variable value and its associated coefficient represented the relative contribution of that variable to a high or low angle-closure score. Across all subjects, the sum of these contributions was approximately 0. A positive relative contribution indicated a push toward higher likelihood of angle closure, whereas a negative relative contribution indicated a push toward a lower likelihood of angle closure.
For each subject, their AS OCT-derived parameters were entered into the formula for the angle closure score, and the corresponding score was calculated. These scores were analyzed alongside the known angle closure status to calculate the AUC, by varying the diagnostic threshold from −∞ to ∞ to obtain all possible combinations of sensitivity and specificity.
To aid in the identification of important variables associated with angle closure for a particular patient, standardized parameters were used, and these are denoted with an asterisk as anterior chamber volume*, anterior chamber width*, iris thickness at 750 μm*, iris area*, anterior chamber area*, and lens vault* ( Table 1 ). The formula for the score then was re-expressed in terms of the standardized variables. For a particular subject, the values of the product of their standardized variables and the corresponding coefficients in the re-expressed score can be plotted to assess the relative contributions of each eye biometry measurement to the angle-closure score. Because anterior chamber area and anterior chamber volume are correlated strongly, their effects are closely linked. To enable interpretation, the value of the sum of the corresponding products can be plotted to assess the joint effect of anterior chamber area and volume. If a particular component of the score is large relative to the other components, then the corresponding variable is a substantial contributing factor to their risk.
| Variable | Mean | Standard Deviation |
|---|---|---|
| Anterior chamber volume (mm 3 ) | 132.23 | 30.65 |
| Anterior chamber width (mm) | 11.76 | 0.39 |
| Iris thickness (mm) | 0.45 | 0.08 |
| Iris area (mm 2 ) | 1.60 | 0.22 |
| Anterior chamber area (mm 2 ) | 19.85 | 3.64 |
| Lens vault (μm) | 470 | 288 |
Validation of the angle closure score
To validate the angle closure score, we tested it on an independent group consisting of 178 hospital-based subjects with gonioscopic angle closure (as defined previously) recruited as part of an ongoing randomized controlled trial ( NCT00347178 , clinicaltrials.gov ) and 301 normal control subjects who were recruited from an ongoing population-based study. The criteria for normals were an intraocular pressure of less than 21 mm Hg with open angles, healthy optic nerves, normal visual fields, and no previous intraocular surgery. AS OCT imaging was performed before laser peripheral iridotomy in the angle-closure subjects.
Results
A total of 2047 subjects were recruited into the study, of whom 679 (33.2%) were excluded for the following reasons: 11 (0.54%) could not undergo gonioscopy, 97 (4.7%) had incomplete demographic or biometric measurements, 62 (3.0%) could not complete the AS OCT examination or had poor quality AS OCT images, 42 (2.1%) had software delineation errors, and 467 (22.8%) had scleral spurs that were not clearly visible on AS OCT images. Therefore, data from 1368 subjects (66.8%) were included in the analysis. Of these, 750 (54.8%) were women, and 1232 (90.0%) were Chinese. The mean age ± standard deviation was 62.4 ± 7.7 years. There were no significant differences in race, spherical equivalent refraction, intraocular pressure, or axial length, but included participants were younger ( P < .001), had shallower ACD ( P = .02), and were more likely to be women ( P = .03).
There were 295 subjects (21.6%) with gonioscopic angle closure. Persons with angle closure were older; had smaller ACD; had smaller anterior chamber width, area, and volume; had greater lens vault; and had thicker irides ( Table 2 ). Findings were similar when only Chinese persons were analyzed.
| Angle Closure (n = 295) | Normal (n = 1073) | P Value | |
|---|---|---|---|
| Age (y) | 64.56 (7.42) | 62.76 (7.43) | <.0001 |
| Male gender | 34.6% | 48.1% | <.0001 |
| Ethnicity | <.0001 | ||
| Chinese | 96.3% | 88.3% | |
| Other | 3.7% | 11.7% | |
| ACD (mm) | 2.68 (0.22) | 3.20 (0.33) | <.0001 |
| AL (mm) | 23.07 (0.88) | 24.15 (1.36) | <.0001 |
| IT750 (mm) | 0.47 (0.08) | 0.45 (0.07) | <.0001 |
| IT2000 (mm) | 0.48 (0.07) | 0.47 (0.07) | .041 |
| IArea (mm 2 ) | 1.61 (0.21) | 1.60 (0.23) | .51 |
| ICurv (mm) | 0.39 (0.09) | 0.27 (0.12) | <.0001 |
| ACW (mm) | 11.57 (0.37) | 11.81 (0.37) | <.0001 |
| ACA (mm 2 ) | 15.66 (1.90) | 21.00 (3.11) | <.0001 |
| ACV (mm 3 ) | 97.70 (15.30) | 141.70 (26.73) | <.0001 |
| LV (μm) | 774 (188) | 386 (252) | <.0001 |
| SE (diopters) | +2.04 (1.78) | +0.37 (2.78) | <.0001 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


