Purpose
To develop and validate an associative model using pupillography that best discriminates those with and without glaucoma.
Design
A prospective case-control study.
Methods
We enrolled 148 patients with glaucoma (mean age 67 ± 11) and 71 controls (mean age 60 ± 10) in a clinical setting. This prototype pupillometer is designed to record and analyze pupillary responses at multiple, controlled stimulus intensities while using varied stimulus patterns and colors. We evaluated three approaches: (1) comparing the responses between the two eyes; (2) comparing responses to stimuli between the superonasal and inferonasal fields within each eye; and (3) calculating the absolute pupil response of each individual eye. Associative models were developed using stepwise regression or forward selection with Akaike information criterion and validated by fivefold cross-validation. We assessed the associative model using sensitivity, specificity and the area-under-the-receiver operating characteristic curve.
Results
Persons with glaucoma had more asymmetric pupil responses in the two eyes ( P < 0.001); between superonasal and inferonasal visual field within the same eye ( P = 0.014); and smaller amplitudes, slower velocities and longer latencies of pupil responses compared to controls (all P < 0.001). A model including age and these three components resulted in an area-under-the-receiver operating characteristic curve of 0.87 (95% CI 0.83 to 0.92) with 80% sensitivity and specificity in detecting glaucoma. This result remained robust after cross-validation.
Conclusions
Using pupillography, we were able to discriminate among persons with glaucoma and those with normal eye examinations. With refinement, pupil testing may provide a simple approach for glaucoma screening.
Glaucoma is the second leading cause of blindness worldwide, affecting 60 million people, 8.4 million of whom are blind. Population-based surveys indicate that glaucoma remains undiagnosed in 90% of affected people globally and in 50% of those in developed countries. There is a need to improve screening and case detection, especially to develop methods that can be applied worldwide and in less-developed countries.
Unlike visual field testing, the assessment of pupillary response to light does not require a subjective patient response. Abnormalities in the pupillary light reflex can be detected by alternately illuminating each eye while comparing the change in pupil size. Asymmetry in this response is referred to as a relative afferent pupillary defect (RAPD) and indicates asymmetric disease in the anterior visual system. Because glaucoma is commonly more severe in one eye, an RAPD is often clinically detectable in persons with glaucoma.
An RAPD can be quantified by sequentially placing optic filters of increasing density in front of the normal eye as a light source alternately illuminates each eye. By using this technique, an RAPD can be detected when there is approximately 25% to 50% unilateral loss of retinal ganglion cells in monkeys. Compared to this method, high-resolution infrared pupillography allows for more precise quantification of the pupillary response using controlled stimulus intensities, and this has improved our ability to detect and objectively quantify subtle RAPDs.
Glaucoma does not result in uniform loss of ganglion cells across the retina. This asymmetry is detectable by comparing the pupil response between superior versus inferior quadrants or peripheral versus central parts of the visual field. This is similar to the glaucoma hemifield test, which also tests for asymmetry between the superior and inferior visual fields. In addition, it is likely that pupil responses in glaucoma may be generally diminished when compared to normal subjects, which can also help with detection.
The purpose of this study was to use pupillography to compare how pupils respond to stimuli of varied patterns, colors and intensities in normal subjects and in glaucoma patients. Further, we developed and validated an associative model that best discriminates those with and without glaucoma by combined use of (1) between-eye pupil response; (2) pupil responses in different parts of the visual field within the same eye; and (3) the absolute response of individual eyes.
Methods
Subjects and Eye Examinations
In this prospective case-control study, we enrolled a total of 243 participants, including 165 patients with glaucoma and 78 normal subjects. All participants were enrolled between March 2011 and June 2012. To be eligible for participation, participants had to be 40 years old or older at enrollment, to have presenting visual acuity better than 20/100 in both eyes, and to have not had ocular surgery within 3 months. All subjects provided informed consent to participate in the study, and the institutional review board of the Johns Hopkins University School of Medicine approved the protocol prospectively.
We enrolled patients with glaucoma of any cause in at least one eye, defined by having both optic disk or retinal nerve fiber layer structural abnormalities and a visual field abnormality consistent with glaucomatous damage. We included a full spectrum of glaucoma disease severity and excluded patients with other macular or retinal comorbidities. In all patients with glaucoma, visual acuity was assessed by habitual correction; intraocular pressure measured by Goldman applanation tonometry; fundus examination by slit-lamp biomicroscopy; visual field testing by standard automated perimetry (Humphrey Field Analyzer, Carl Zeiss Meditec, Dublin, California, USA) using the Swedish Interactive Threshold Algorithm standard strategy and 24-2 pattern ; and retinal nerve fiber layer thickness (RNFL) measured by a circumpapillary scan at 3.45 mm from the center of the disk using spectral domain optical coherence tomography (SD-OCT) (Spectralis; Heidelberg Engineering, Heidelberg, Germany).
We enrolled normal subjects who were at the Wilmer Eye Institute (Baltimore, Maryland, USA) accompanying patients attending examinations. All normal subjects underwent an undilated fundus exam, visual acuity testing, intraocular pressure measurement using the Icare tonometer (Icare, Helsinki, Finland), and RNFL measurement using SD-OCT. We also assessed their visual field using frequency-doubling technology (FDT) (Humphrey Matrix Perimeter; Carl Zeiss Meditec, Dublin, California, USA). We excluded normal subjects with cup-to-disk ratios greater than 0.7, signs of retinal or optic nerve structural abnormalities, and abnormal visual field results in either eye. When analyzing the FDT results, we minimized the false-negative rate by using the N-30-5 screening protocol. The test was considered reliable if false-positives and fixation losses were less than 30%. A subject was considered eligible if there was no abnormal point in the central locations and no more than 2 abnormal points at any probability level ( P < 5%, 2%, 1%, or <0.5%) at any of the peripheral locations.
Pupillometer and Waveform Analysis
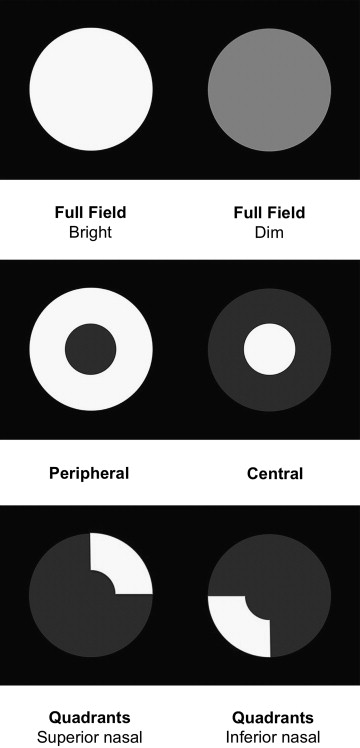
We used a prototype automated pupillometer (prototype of RAPDx; Konan Medical USA, Irvine, California, USA) to record and analyze the pupillary light reflex. Each subject was dark-adapted for 1 minute before the test. While the patient was viewing binocularly, monocular stimuli were presented on the LCD panel, alternating between eyes (similar to the swinging flashlight test). We applied stimuli of varied colors (white, red, green, blue, and yellow); of varied patterns (full field, peripheral [28 degrees with 10.5 degrees macular sparing]; central (2.9 degrees); and superior and inferior nasal quadrant arcs (21 degrees with 11.7-degree macular spacing); and of varied intensities (35 lux [bright] and 25 lux [dim] ( Fig. 1 ). All stimulus cycles added up to 2.1 seconds, with full-field stimulations of 200 ms followed by 1900 ms dark and patterned stimulations of 600 ms followed by 1500 ms dark. The entire examination lasted approximately 7 minutes.
The device records pupil diameter over time and calculates 6 metrics (response amplitude, latency, maximum constriction velocity, maximum dilation velocity, and time to peak constriction and dilation). The amplitude of pupil constriction is calculated by the percentage of change in pupil diameter (PD) between constriction onset and peak constriction in response to each stimulus [(PD resting − PD constricted )/PD resting ]. By using the first-order and second-order derivatives of the pupil diameter over time, 2 additional metrics—maximum constriction velocity and maximum dilation velocity—were calculated. We defined the onset of pupil constriction as the time when the velocity first crossed a threshold of 50% of the maximum contraction velocity and then calculated the latency using the time from the onset of stimulation to the onset of pupil constriction. We also calculated the time from stimulus onset to the time of these maximal velocities.
The between-eye score was defined as the log of the relative ratio of a given pupil metric between the right and left eye multiplied by 10. Similarly, the within-eye score was defined by taking the log of the relative ratio of the given pupil metric between the superonasal and inferonasal field and multiplying by 10.
Statistical Analysis
Differences in characteristics and pupil metrics between patients with glaucoma and normal subjects were compared using the Student t test and the χ 2 test. We used the Pearson correlation to assess the asymmetry of pupil response between the two eyes or between superior and inferior stimuli within each eye. For analyses performed at the level of individual eyes, we used the eye with the higher within-eye score or eyes with lower response amplitude. To avoid multicollinearity in a regression model, we assessed the correlations among responses to different colors, among responses to different patterns, and among the metrics of the same pupil responses. We then built models using only variables that are less correlated with each other (R < 0.6).
We used univariate and multivariate logistic regression models to assess the association between each pupil metric and glaucoma. The 5 models included (1) a univariate model with the between-eye score of response amplitude as the sole predictor; (2) a multivariable model using 4 variables: age, between-eye scores, within-eye scores, and the absolute value of response amplitude; (3) a model with variables selected using stepwise forward regression ( P < 0.1 to be included in the model and P > 0.2 to be excluded); (4) a model with variables determined using forward selection and Akaike information criteria; and (5) a model using all variables.
We determined the ability of the model to discriminate glaucomatous eyes from normal eyes by calculating the area-under-the-receiver operating characteristic curve (AUROC) by using a nonparametric approach. We used bootstrap resampling to calculate pointwise confidence intervals for the receiver operating characteristic curve at the false-positive rate of 0.2 and the true-positive rate of 0.2. The resampling was done separately for case and control strata and included 1,000 replications. We also assessed the performance of each model in patients who had visual field mean deviations (MDs) worse than −5 dB and those who had MDs of −5 dB or better. Finally, we validated the results by splitting the data randomly into quintiles, with model development in 4 of the 5 and testing in 1 of the 5, which was repeated 5 times (fivefold cross-validation). Statistical analyses were performed using STATA 12.0 (StataCorp LP, College Station, Texas, USA).
Results
A total of 236 eligible participants were enrolled in our study, and 219 (93%) of them completed the pupillographic examination. Of the 17 incomplete examinations, 4 were due to frequent blinking, 3 were due to software errors, and the pupil waveforms of the other 10 were unanalyzable. Among the 219 subjects who successfully completed the pupillographic test, 148 cases had glaucoma in at least 1 eye (93% primary open-angle glaucoma, 3% primary angle-closure glaucoma, and 4% secondary glaucoma), and 71 controls had no glaucoma in either eye. Compared to controls, patients with glaucoma were significantly older (67 ± 11 vs 60 ± 10 years of age) and were more likely to be male (51% vs 32%) ( Table 1 ). Patients with glaucoma had greater between-eye differences in intraocular pressure and RNFL thickness but had similar baseline pupil diameters when compared to controls.
| Glaucoma (n = 148) | Control (n = 71) | |
|---|---|---|
| Age, year a | 67.4 ± 10.7 | 60.4 ± 9.6 |
| Female, no. (%) a | 72 (49) | 48 (68) |
| Race, no. (%) | ||
| Non-Hispanic white | 121 (81.8) | 51 (71.8) |
| Black | 20 (13.5) | 12 (16.9) |
| Asian | 7 (4.7) | 7 (9.9) |
| Hispanic | 0 (0) | 1 (1.4) |
| Baseline pupil diameter, mm | ||
| Average between the 2 eyes | 4.10 ± 0.81 | 4.17 ± 0.71 |
| Absolute difference between the two eyes | 0.05 ± 0.04 | 0.05 ± 0.04 |
| Intraocular pressure, mm Hg | ||
| Average between the 2 eyes | 14.1 ± 3.5 | 13.6 ± 3.9 |
| Absolute difference between the 2 eyes a | 2.8 ± 3.2 | 1.1 ± 0.9 |
| Visual field mean deviation (dB) | ||
| Average between the 2 eyes a | −7.35 (6.24) | −0.72 (0.78) |
| Absolute differences between the 2 eyes a | 5.81 (5.69) | 0.69 (0.53) |
| Retinal nerve fiber layer thickness, μm | ||
| Average between the 2 eyes a | 65.8 ± 15.7 | 93.6 ± 9.6 |
| Absolute difference between the 2 eyes a | 13.4 ± 12.3 | 4.2 ± 4.9 |
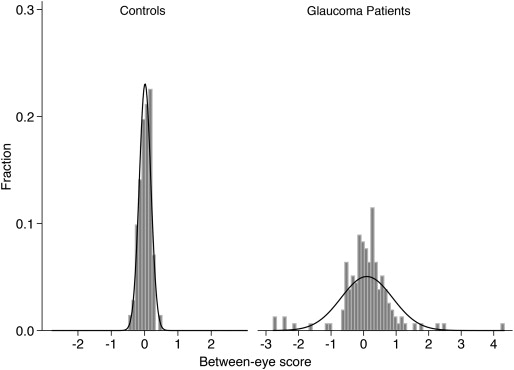
The correlation of each pupil metric was lower in the eyes of patients with glaucoma than in the eyes of controls across different stimuli ( Table 2 ). The absolute value of the between-eye scores was generally higher in patients with glaucoma, suggesting greater between-eye asymmetry ( Table 2 ). However, many patients with glaucoma also had a between-eye scores close to zero ( Fig. 2 ). When looking at within-eye responses to stimuli, the correlation between superonasal and inferonasal stimuli was lower in patients with glaucoma and their absolute within-eye scores were higher, suggesting greater within-eye asymmetry ( Table 3 ). We summarize the absolute values of each pupil metric under varied stimuli for each individual eye in Table 4 . Eyes with glaucoma had smaller response amplitude, slower velocities and longer latency than control eyes (all P < 0.05).
| Correlation Coefficient | Absolute Between-eye Score Mean ± SD | |||
|---|---|---|---|---|
| Glaucoma | Control | Glaucoma | Control | |
| White, full field, bright | ||||
| Amplitude a | 0.76 | 0.96 | 0.47 ± 0.51 | 0.14 ± 0.10 |
| Latency a | 0.83 | 0.93 | 0.23 ± 0.21 | 0.15 ± 0.14 |
| Max constriction velocity a | 0.89 | 0.98 | 0.36 ± 0.36 | 0.12 ± 0.11 |
| Time to max constriction velocity a | 0.86 | 0.92 | 0.16 ± 0.13 | 0.11 ± 0.08 |
| Max dilation velocity | 0.76 | 0.77 | 0.42 ± 0.53 | 0.30 ± 0.49 |
| Time to max dilation velocity a | 0.74 | 0.88 | 0.24 ± 0.19 | 0.12 ± 0.11 |
| Red, full field, bright | ||||
| Amplitude a | 0.66 | 0.91 | 0.68 ± 0.72 | 0.28 ± 0.25 |
| Latency | 0.73 | 0.85 | 0.31 ± 0.26 | 0.25 ± 0.23 |
| Max constriction velocity a | 0.79 | 0.90 | 0.50 ± 0.50 | 0.36 ± 0.28 |
| Time to max constriction velocity a | 0.80 | 0.81 | 0.23 ± 0.23 | 0.17 ± 0.13 |
| Max dilation velocity | 0.73 | 0.83 | 0.55 ± 0.49 | 0.47 ± 0.52 |
| Time to max dilation velocity a | 0.65 | 0.74 | 0.30 ± 0.25 | 0.20 ± 0.19 |
| Green, full field, bright | ||||
| Amplitude a | 0.74 | 0.94 | 0.57 ± 0.57 | 0.22 ± 0.19 |
| Latency | 0.82 | 0.87 | 0.24 ± 0.25 | 0.24 ± 0.20 |
| Max constriction velocity a | 0.83 | 0.96 | 0.49 ± 0.44 | 0.21 ± 0.18 |
| Time to max constriction velocity | 0.73 | 0.79 | 0.22 ± 0.20 | 0.19 ± 0.14 |
| Max dilation velocity | 0.66 | 0.48 | 0.55 ± 0.63 | 0.51 ± 0.68 |
| Time to max dilation velocity | 0.66 | 0.59 | 0.29 ± 0.24 | 0.25 ± 0.20 |
| Blue, full field, bright | ||||
| Amplitude a | 0.76 | 0.92 | 0.60 ± 0.58 | 0.28 ± 0.20 |
| Latency a | 0.74 | 0.92 | 0.33 ± 0.27 | 0.18 ± 0.14 |
| Max constriction velocity a | 0.84 | 0.92 | 0.45 ± 0.43 | 0.33 ± 0.23 |
| Time to max constriction velocity | 0.77 | 0.77 | 0.23 ± 0.22 | 0.19 ± 0.15 |
| Max dilation velocity | 0.68 | 0.69 | 0.59 ± 0.64 | 0.46 ± 0.52 |
| Time to max dilation velocity a | 0.61 | 0.68 | 0.34 ± 0.24 | 0.22 ± 0.19 |
| Yellow, full field, bright | ||||
| Amplitude a | 0.75 | 0.93 | 0.59 ± 0.55 | 0.23 ± 0.19 |
| Latency a | 0.85 | 0.91 | 0.27 ± 0.19 | 0.20 ± 0.17 |
| Max constriction velocity a | 0.86 | 0.96 | 0.46 ± 0.41 | 0.23 ± 0.17 |
| Time to max constriction velocity a | 0.66 | 0.86 | 0.25 ± 0.24 | 0.16 ± 0.15 |
| Max dilation velocity | 0.75 | 0.79 | 0.48 ± 0.57 | 0.40 ± 0.42 |
| Time to max dilation velocity a | 0.60 | 0.69 | 0.31 ± 0.25 | 0.23 ± 0.21 |
| White, peripheral, bright | ||||
| Amplitude a | 0.62 | 0.85 | 0.81 ± 0.63 | 0.46 ± 0.33 |
| Latency a | 0.61 | 0.75 | 0.41 ± 0.36 | 0.27 ± 0.26 |
| Max constriction velocity a | 0.75 | 0.88 | 0.73 ± 0.53 | 0.47 ± 0.43 |
| Time to max constriction velocity a | 0.58 | 0.59 | 0.37 ± 0.29 | 0.28 ± 0.22 |
| Max dilation velocity a | 0.60 | 0.65 | 0.75 ± 0.78 | 0.52 ± 0.68 |
| Time to max dilation velocity | 0.57 | 0.43 | 0.32 ± 0.28 | 0.31 ± 0.24 |
| White, peripheral, dim | ||||
| Amplitude a | 0.68 | 0.75 | 0.77 ± 0.63 | 0.54 ± 0.45 |
| Latency | 0.61 | 0.75 | 0.45 ± 0.39 | 0.42 ± 0.31 |
| Max constriction velocity a | 0.78 | 0.85 | 0.71 ± 0.54 | 0.58 ± 0.49 |
| Time to max constriction velocity | 0.38 | 0.55 | 0.42 ± 0.43 | 0.33 ± 0.28 |
| Max dilation velocity | 0.48 | 0.39 | 0.71 ± 0.83 | 0.67 ± 0.85 |
| Time to max dilation velocity | 0.50 | 0.26 | 0.33 ± 0.30 | 0.28 ± 0.22 |
| White, central, bright | ||||
| Amplitude a | 0.54 | 0.57 | 1.52 ± 1.42 | 1.04 ± 0.80 |
| Latency | 0.35 | 0.32 | 0.73 ± 0.67 | 0.67 ± 0.60 |
| Max constriction velocity | 0.70 | 0.66 | 0.99 ± 0.98 | 0.78 ± 0.64 |
| Time to max constriction velocity | 0.27 | 0.49 | 0.54 ± 0.64 | 0.40 ± 0.32 |
| Max dilation velocity | 0.10 | 0.19 | 1.18 ± 1.53 | 1.30 ± 1.80 |
| Time to max dilation velocity | 0.40 | 0.26 | 0.51 ± 0.42 | 0.46 ± 0.38 |
| White, central, dim | ||||
| Amplitude a | 0.61 | 0.62 | 1.54 ± 1.72 | 1.00 ± 0.89 |
| Latency | 0.31 | 0.11 | 0.91 ± 0.81 | 0.88 ± 0.84 |
| Max constriction velocity | 0.70 | 0.75 | 1.02 ± 0.89 | 0.81 ± 0.64 |
| Time to max constriction velocity | 0.29 | 0.49 | 0.60 ± 1.16 | 0.45 ± 0.42 |
| Max dilation velocity | 0.42 | 0.46 | 0.93 ± 0.97 | 0.91 ± 0.84 |
| Time to max dilation velocity | 0.45 | 0.25 | 0.46 ± 0.35 | 0.50 ± 0.40 |
| Correlation Coefficient | Absolute within-eye Score Mean ± SD | |||
|---|---|---|---|---|
| Glaucoma | Normal | Glaucoma | Normal | |
| White | ||||
| Amplitude a | 0.62 | 0.64 | 1.63 ± 1.23 | 1.20 ± 0.78 |
| Latency | 0.30 | 0.43 | 0.93 ± 0.70 | 0.78 ± 0.60 |
| Max constriction velocity | 0.72 | 0.70 | 1.17 ± 0.75 | 1.01 ± 0.56 |
| Time to max constriction velocity | 0.08 | 0.26 | 0.71 ± 0.96 | 0.51 ± 0.47 |
| Max dilation velocity | 0.13 | 0.52 | 1.29 ± 1.29 | 0.97 ± 0.72 |
| Time to max dilation velocity a | 0.26 | 0.24 | 0.54 ± 0.35 | 0.41 ± 0.26 |
| Red | ||||
| Amplitude a | 0.41 | 0.54 | 2.97 ± 2.48 | 2.28 ± 1.63 |
| Latency | 0.10 | 0.32 | 1.11 ± 0.80 | 0.99 ± 0.64 |
| Max constriction velocity a | 0.45 | 0.63 | 1.90 ± 1.39 | 1.47 ± 0.92 |
| Time to max constriction velocity | 0.22 | 0.39 | 0.72 ± 0.50 | 0.60 ± 0.39 |
| Max dilation velocity | 0.02 | 0.05 | 1.97 ± 1.50 | 2.19 ± 2.00 |
| Time to max dilation velocity | 0.07 | 0.08 | 0.82 ± 0.47 | 0.85 ± 0.52 |
| Green | ||||
| Amplitude a | 0.63 | 0.59 | 1.70 ± 1.14 | 1.31 ± 0.92 |
| Latency | 0.40 | 0.50 | 0.90 ± 0.63 | 0.78 ± 0.45 |
| Max constriction velocity | 0.73 | 0.69 | 1.18 ± 0.82 | 1.05 ± 0.66 |
| Time to max constriction velocity | 0.31 | 0.27 | 0.67 ± 0.86 | 0.53 ± 0.35 |
| Max dilation velocity | 0.07 | 0.05 | 1.57 ± 1.25 | 1.66 ± 1.69 |
| Time to max dilation velocity a | 0.26 | 0.07 | 0.61 ± 0.37 | 0.74 ± 0.42 |
| Blue | ||||
| Amplitude | 0.62 | 0.60 | 1.99 ± 1.91 | 1.51 ± 1.10 |
| Latency a | 0.20 | 0.53 | 0.98 ± 0.74 | 0.74 ± 0.46 |
| Max constriction velocity | 0.70 | 0.67 | 1.37 ± 1.05 | 1.16 ± 0.87 |
| Time to max constriction velocity a | 0.25 | 0.47 | 0.64 ± 0.48 | 0.50 ± 0.36 |
| Max dilation velocity | 0.06 | 0.38 | 1.75 ± 1.62 | 1.47 ± 1.16 |
| Time to max dilation velocity | 0.28 | 0.13 | 0.68 ± 0.38 | 0.79 ± 0.43 |
| Yellow | ||||
| Amplitude a | 0.62 | 0.58 | 1.87 ± 1.37 | 1.51 ± 1.16 |
| Latency a | 0.31 | 0.55 | 0.88 ± 0.62 | 0.71 ± 0.48 |
| Max constriction velocity | 0.63 | 0.68 | 1.35 ± 1.01 | 1.14 ± 0.76 |
| Time to max constriction velocity a | 0.21 | 0.38 | 0.70 ± 0.58 | 0.46 ± 0.43 |
| Max dilation velocity | 0.03 | 0.30 | 1.72 ± 1.59 | 1.57 ± 1.42 |
| Time to max dilation velocity | 0.29 | 0.03 | 0.61 ± 0.36 | 0.61 ± 0.37 |
| Amplitude (Ratio) | Latency (second) | Max Contraction Velocity (mm/ms) | Time to Max Contraction (second) | Max Dilation Velocity (mm/ms) | Time to Max Dilation (second) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Glaucoma | Control | Glaucoma | Control | Glaucoma | Control | Glaucoma | Control | Glaucoma | Control | Glaucoma | Control | |
| Full, bright | ||||||||||||
| White | 0.25 ± 0.05 | 0.29 ± 0.04 | 0.20 ± 0.03 | 0.18 ± 0.02 | 3.28 ± 0.79 | 3.81 ± 0.74 | 0.42 ± 0.04 | 0.40 ± 0.03 | 2.02 ± 0.47 | 2.18 ± 0.43 | 1.20 ± 0.11 | 1.16 ± 0.09 |
| Red | 0.21 ± 0.05 | 0.25 ± 0.05 | 0.22 ± 0.03 | 0.20 ± 0.03 | 2.95 ± 0.74 | 3.39 ± 0.76 | 0.43 ± 0.04 | 0.41 ± 0.03 | 1.79 ± 0.42 | 2.03 ± 0.60 | 1.16 ± 0.11 | 1.10 ± 0.09 |
| Green | 0.24 ± 0.06 | 0.28 ± 0.05 | 0.21 ± 0.03 | 0.19 ± 0.03 | 3.19 ± 0.81 | 3.75 ± 0.78 | 0.42 ± 0.04 | 0.40 ± 0.03 | 1.95 ± 0.47 | 2.11 ± 0.41 | 1.18 ± 0.11 | 1.13 ± 0.09 |
| Blue | 0.22 ± 0.06 | 0.26 ± 0.05 | 0.22 ± 0.03 | 0.19 ± 0.03 | 3.10 ± 0.79 | 3.57 ± 0.78 | 0.43 ± 0.04 | 0.41 ± 0.04 | 1.86 ± 0.46 | 2.03 ± 0.40 | 1.17 ± 0.11 | 1.12 ± 0.09 |
| Yellow | 0.24 ± 0.06 | 0.29 ± 0.05 | 0.20 ± 0.03 | 0.18 ± 0.03 | 3.27 ± 0.83 | 3.80 ± 0.78 | 0.42 ± 0.04 | 0.40 ± 0.03 | 1.97 ± 0.51 | 2.18 ± 0.42 | 1.18 ± 0.11 | 1.14 ± 0.10 |
| Peripheral, bright | ||||||||||||
| White | 0.26 ± 0.06 | 0.31± 0.05 | 0.22 ± 0.03 | 0.19 ± 0.03 | 3.11 ± 0.81 | 3.69 ± 0.88 | 0.44 ± 0.05 | 0.41 ± 0.03 | 1.82 ± 0.49 | 2.12 ± 0.52 | 1.38 ± 0.12* | 1.37 ± 0.09* |
| Red | 0.19 ± 0.06 | 0.23 ± 0.05 | 0.23 ± 0.05 | 0.20 ± 0.03 | 2.53 ± 0.78 | 3.03 ± 0.75 | 0.45 ± 0.07 | 0.42 ± 0.04 | 1.64 ± 0.45 | 1.80 ± 0.41 | 1.29 ± 0.15* | 1.26 ± 0.12* |
| Green | 0.23 ± 0.06 | 0.28 ± 0.05 | 0.22 ± 0.04 | 0.19 ± 0.03 | 3.02 ± 0.84 | 3.55 ± 0.85 | 0.44 ± 0.05 | 0.41 ± 0.04 | 1.86 ± 0.51 | 2.02 ± 0.49 | 1.33 ± 0.12* | 1.31 ± 0.10* |
| Blue | 0.21 ± 0.06 | 0.26 ± 0.06 | 0.23 ± 0.03 | 0.20 ± 0.04 | 2.85 ± 0.80 | 3.43 ± 0.90 | 0.44 ± 0.05 | 0.41 ± 0.04 | 1.77 ± 0.48 | 1.94 ± 0.52 | 1.29 ± 0.13* | 1.25 ± 0.13* |
| Yellow | 0.24 ± 0.06 | 0.29 ± 0.05 | 0.22 ± 0.03 | 0.19 ± 0.03 | 3.08 ± 0.81 | 3.58 ± 0.82 | 0.44 ± 0.05 | 0.41 ± 0.04 | 1.90 ± 0.50 | 2.06 ± 0.45 | 1.32 ± 0.12* | 1.32 ± 0.09* |
| Peripheral, dim | ||||||||||||
| White | 0.24 ± 0.06 | 0.27 ± 0.05 | 0.23 ± 0.03 | 0.20 ± 0.03 | 2.87 ± 0.79 | 3.38 ± 0.89 | 0.45 ± 0.04 | 0.42 ± 0.04 | 1.77 ± 0.46 | 1.91 ± 0.41 | 1.37 ± 0.12* | 1.36 ± 0.08* |
| Red | 0.16 ± 0.05 | 0.19 ± 0.05 | 0.24 ± 0.04 | 0.22 ± 0.04 | 2.23 ± 0.65 | 2.61 ± 0.71 | 0.46 ± 0.05 | 0.43 ± 0.04 | 1.56 ± 0.45* | 1.61 ± 0.35* | 1.32 ± 0.12 | 1.28 ± 0.12 |
| Green | 0.21 ± 0.06 | 0.25 ± 0.06 | 0.23 ± 0.03 | 0.20 ± 0.03 | 2.73 ± 0.83 | 3.25 ± 0.79 | 0.45 ± 0.05 | 0.42 ± 0.04 | 1.76 ± 0.46* | 1.88 ± 0.54* | 1.33 ± 0.13 | 1.29 ± 0.09 |
| Blue | 0.19 ± 0.06 | 0.23 ± 0.06 | 0.24 ± 0.04 | 0.21 ± 0.04 | 2.59 ± 0.79 | 3.06 ± 0.76 | 0.45 ± 0.05 | 0.42 ± 0.04 | 1.66 ± 0.47 | 1.82 ± 0.46 | 1.30 ± 0.14 | 1.26 ± 0.10 |
| Yellow | 0.22 ± 0.06 | 0.26 ± 0.05 | 0.23 ± 0.04 | 0.20 ± 0.03 | 2.85 ± 0.79 | 3.39 ± 0.85 | 0.44 ± 0.05 | 0.41 ± 0.04 | 1.82 ± 0.51* | 1.95 ± 0.38* | 1.32 ± 0.10* | 1.29 ± 0.12* |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


