Chapter 8
DESIGNING THE MANAGEMENT STRATEGY

Treating a patient with eye injury requires specific knowledge of the anatomy, physiology, and pathophysiology of all tissues of the globe; surgical expertise or manual skills do not by themselves suffice. It is equally important, though rarely discussed in the literature, for the ophthalmologist to develop strategic thinking so that a systematic philosophy is utilized in every case, even if the injured eye presents unique difficulties for which no published recommendation is available.
PEARL… Strategy is the general foundation based on which the specifics (tactics, plan) are developed.
This chapter provides an overview of the fundamentals in strategic thinking, based on which surgeons can develop their own, individualized approach.
PEARL… The goal is more than optimal treatment of the injured eye; it is treatment of a person who has a traumatized organ. Ophthalmologists dealing with ocular trauma are not “tissue reconstruction specialists” but physicians.
When designing the strategy (plan) to treat the eye’s specific injuries, the surgeon must understand that the relationship between the injured person and the ophthalmologist is one of chance, not of choice as with that of patients who present for elective surgery.
The ophthalmologist’s (and the medical staff’s) attitude, behavior, words, and metacommunication determine whether the patient develops sufficient confidence and trust in the treating physician—without which it is much more difficult to involve the patient as a partner.
The “partnership” is crucial because the patient is commonly:
• asked to follow instructions such as positioning after intravitreal gas injection;
• required to take all prescribed medications for extended periods of time exactly as directed; and, most importantly,
• involved in the decision-making process itself, helping to determine whether one procedure or another should be performed or whether the eye should be removed rather than reconstructed.
Proper communication with the patient requires the ophthalmologist to explain:
• the management options and their risks versus benefits and the short- and long-term implications, including a carefully pessimistic estimation of the final outcome;
• the potential for multiple surgeries;
• the potential for visual rehabilitation services;
• the advantages of safety eyewear; and
• the need for periodic follow-ups even if full vision has been restored (see Chapters 3, 5, and 6 for further details).
Such systematic thinking will result in the development of the best possible management plan (see Sections II through VI for the specifics of treating the individual tissue injuries).
HISTORY AND EVALUATION
Appropriate plans are impossible to design unless the ophthalmologist has a fairly accurate knowledge of:
• how the injury occurred; and
• what its consequences are (i.e., which tissues are involved and to what extent).
It is also mandatory to know whether the injured eye had prior surgery; for instance when struck by blunt force, eyes with ECCE or RK1 wounds can rupture years after the procedure.a
The details of evaluating the injured patient and eye are presented in Chapters 9 and 10 with additional details in the appropriate chapters. Here we emphasize only a few fundamental rules:
• in conscious and cooperating patients, always assess the visual acuity in both eyes, one eye at a time;
• avoid inflicting iatrogenic damage (e.g., extrusion of intraocular tissues) to the eye (e.g., by forceful opening of the lids in children who will not or in adults who cannot obey instructions);
• once the diagnosis of an open globe injury requiring surgery is made, delay determining nonsignificant details until the patient is asleepb;
• order only those diagnostic tests that are essentialc;
• document your oral communications with the patient and all details of the injury, especially if the incident occurred at the workplace using
 drawings (e.g., show the location and extent of the eyewall’s wound; Fig. 8–1);
drawings (e.g., show the location and extent of the eyewall’s wound; Fig. 8–1);
 pre- and postoperative photographs; and
pre- and postoperative photographs; and
 intraoperative video or videos (see Chapter 7 for the potential drawback);
intraoperative video or videos (see Chapter 7 for the potential drawback);
• try to have a witness present throughout your discussions with the patient; because of their understandable anxiety, patients frequently do not remember what they were told or remember inaccurately.
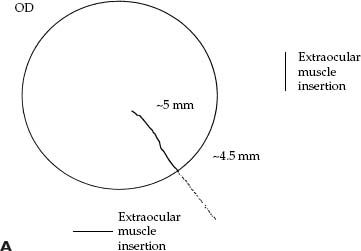
FIGURE 8–1 The power of a simple drawing (A) versus a lengthy description (B).
PEARL… Do not order tests whose results will not influence your subsequent treatment decisions. Conversely, the results of radiological tests should be checked by the ophthalmologist.
Proper documentation is critical for treatment, research, and legal purposes and in case of referral. If you participate in a surveillance system such as the USEIR, it is wise to instruct your staff to attach the initial reporting form to every trauma chart. If you see many patients with eye injuries but are not part of a data collection system, you should consider joining or establishing one (see Chapters 4 and 9) or at least designing a special chart for trauma patients.
TRADITIONAL VERSUS PLANNED APPROACH TO EYE TRAUMA
According to the traditional concept, surgeons operating on injured eyes should proceed in a sequential fashion, reacting to the actual situation (as determined by the trauma as well as by the body’s reaction to the injury and to the applied therapeutic measures; see Fig. 8–2A). This approach requires:
• assessing the injury’s consequences;
• performing certain manipulations as appropriate;
• reassessing the eye’s condition;
• performing additional manipulations as appropriate; and
• repeating the process as many times as needed.
Example: eye with penetrating injury caused by a wire at the home; mild traumatic cataract with a large anterior capsule rupture; significant vitreous hemorrhage. This eye would undergo (1) primary wound closure, (2) secondary surgery with cataract removal (possibly with IOL implantation), (3) simultaneous or delayed vitreous hemorrhage removal if no sign of spontaneous resorption of the blood is seen after a few months, (4) treatment of retinal pathology if necessary, and (5) restoration of the lost refractive power if IOL implantation has not been performed earlier.
This traditional thinking is best characterized by the analogy of a person climbing a tree and making decisions “on the go” regarding which branch to step onto next. This traditional approach is not entirely wrong—but it forces the surgeon to view the restoration process as a series of individual surgical tasks as they emerge with time: the surgeon remains passive.
An alternative, strategically planned approach involves thinking “backwards from the desired endpoint” (see Fig. 8–2B) based on the following order of goals:
• full restoration of the eye’s visual functions;
• partial restoration of the eye’s visual functions if the former is impossible; or
• full restoration of the eye’s normal anatomy (even if no visual function is achievable), depending on
 comfort;
comfort;
 cosmesis; and
cosmesis; and
 the patient’s desire or decision when all factors, including SO (see Chapter 29), have been taken into consideration.
the patient’s desire or decision when all factors, including SO (see Chapter 29), have been taken into consideration.
In the preceding example, the eye would undergo wound closure with cataract and vitreous hemorrhage removal to allow examination of the retina and treatment of any pathologic condition that requires intervention. IOL implantation would be performed if further vitreoretinal intervention appears unlikely (see Chapter 21) and the IOL power can reasonably be determined. (Alternatively, all steps beyond wound toilette and closure may be performed a few days later—see below.)
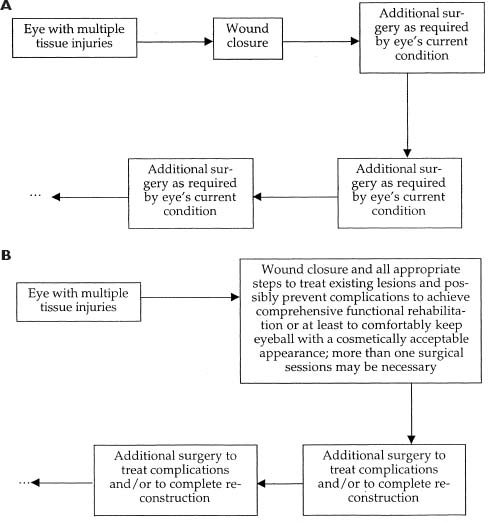
FIGURE 8–2 The traditional (A) and the suggested (B) way of thinking in approaching the eye with an eye injury.
A person with this conceptual thinking, when trying to climb a tree, would inspect the tree and design a plan, selecting from the ground a route that appears to offer the safest way to reach the highest possible altitude. Obviously, during the actual climb, the original plan may have to be modified, just as the surgeon must remain flexible to alter the initial strategy should the eye’s actual condition warrant it.
At first, there may not appear to be a tangible difference between these two approaches. However, the second concept requires that the ophthalmologist play an active role, appreciating the eye’s condition in a comprehensive way.
PEARL… An injured globe should be considered as a polytraumatized organ: a certain tissue injury may affect the condition of other tissues.
In the example, the ophthalmologist whose approach is based on strategic thinking would review the following: the lens injury makes it likely that the cataract will not remain stationary, the presence of vitreous hemorrhage in case of a penetrating injury significantly increases the chance of tractional retinal detachment,2 and there is a measurable risk of direct retinal injury. It is therefore advisable to remove all media opacity early to allow direct inspection of the retina by the surgeon to determine whether and what kind of intervention is necessary to keep the retina attached and achieve early and maximal visual rehabilitation.
This planned approach also requires immediate steps for low-vision rehabilitation (see Chapter 6) if the eye’s condition leaves no hope for significant functional improvement (see Chapter 3), e.g., a macular impact site is found during surgery in the example above.
THE SURGEON: KNOW YOUR CAPABILITIES AND LIMITATIONS
Reconstruction of a traumatized globe can be a complex procedure; life does not recognize artificial boundaries such as “anterior” versus “posterior” segment. if an ophthalmologist cannot address all treatable lesions (see Table 8–1), it is usually preferable not to perform any surgery but to refer the patient. To decide in favor of intervention, the physician must have adequate experience and expertise as well as access to the required equipment and personnel and facility.
If any one of these is missing, deferral or referral is probably a better option for both ophthalmologist and patient. Do not attempt, for instance, to remove traumatic cataracts if vitrectomy instrumentation is unavailabled or you have no experience in its use; do not try to close corneal/scleral wounds if a good microscope is not available. Violation of these basic rules can worsen the eye’s condition. Before deciding to “go in”, the ophthalmologist should do a brief (self) assessment.
PEARL… The most fundamental rule in the treatment of an injured globe: If you can’t, don’t.
PITFALL
An error all too commonly seen is the “forced” use of the technique a surgeon is most familiar or comfortable with instead of using the technique most suitable to solve the particular problem (i.e., trying to adopt the eye to the intervention rather than selecting the technique with the highest success rate). Typical examples: the application of phacoemulsification to remove a traumatic cataract despite the risk of vitreous prolapse (instead of using vitrectomy instrumentation); prophylactic blind cryopexy of a scleral wounde (instead of removing the vitreous hemorrhage to inspect the retina underneath the wound and applying laser if a retinal break is present).
Conversely, an ophthalmologist is rightly called a “trauma expert” if possessing sufficient expertise in treating all globe injuries.
An institution is de facto an eye trauma center if the following are in place:
• appropriate on-call system with all specialists available;
• complete technical infrastructure;
• data collection system (tracking both epidemiological and clinical information);
• active pursuit (follow-up) of all accessible patients; and
• continual quality control process with periodical external reviews.
| Procedure | Example | |
|---|---|---|
| Reappose/reattach | Closure of corneal wound/retinal detachment | |
| Reformat | Injection of BSS into the AC | |
| Remove/excise | Traumatic cataract/prolapsed uvea | |
| Reduce | SCH | |
| Replace | Vitreous with air | |
| Reposition | Prolapsed uvea/dislocated IOL | |
| Seal | Retinal break | |
| Reconstruct† | Anterior segment |
* Breaking down the four basic elements in surgery (excisional; reconstructive; transplant; inductive). +May be a combination of all of the above.
† May be a combination of all of the above.
RECONSTRUCTION VERSUS ENUCLEATION:f THE SIGNIFICANCE OF NLP VISION
Enucleation is a point of no return. Ophthalmologists rarely review enucleated eyes with the pathologist, although such clinicopathologic correlations should be routinely performed and would reduce unindicated removals of eyes.g
Truly medical reasons to perform primary enucleation are very few:
• when the eye is destroyed or cannot be reconstructed anatomically (i.e., wound or wounds are too large and posterior) and/or
• most of the globe’s contents, including a substantial portion of the retina, are lost, leaving no hope for any function.
PEARL… Loss of light perception in the immediate postinjury period does not by itself justify enucleation. We have found that of NLP eyes reconstructed on the basis of the ophthalmologist’s judgment (i.e., excluding eyes reconstructed solely because of the patient’s request), 64% improved.3 Even a preoperatively nonrecordable bright-flash ERG is compatible with visual recovery if appropriate and timely reconstruction is persued.3
Several reversible factors may be responsible for NLP initial vision:
• media opacity (corneal edema, hyphema4, cataract5, vitreous hemorrhageh;
• retinal edema (commotio retinae);
• retinal detachment/subretinal hemorrhage; and
• the patient’s mental condition.
PEARL… No eye in the first few weeks after an injury should be enucleated based solely on its inability to detect light or because “the globe appears so badly damaged.” Patients can be offered exploration and direct inspection by the vitreoretinal surgeon as a decision point.
It must also be mentioned that even in cases of TON being responsible for NLP vision, treatment, rather than abandonment, is recommended (see Chapter 37).
Secondary enucleation may be performed if:
• the eye chronically and despite reconstruction efforts remains NLP; and
• the risk of SO is determined to be higher than usual (see Chapter 29).
Even if this is the case, the ophthalmologist must, however, discuss all options with the patient, and not simply “prescribe” eye removal. Most patients prefer retaining the reconstructed eye to enucleationi (see Fig. 8–3
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


