Purpose
To evaluate visual outcome and endothelial cell survival after Descemet membrane endothelial keratoplasty (DMEK) in comparison with Descemet stripping automated endothelial keratoplasty (DSAEK).
Design
Single-center, retrospective, consecutive case series.
Methods
Thirty-eight eyes of 38 consecutive patients undergoing DMEK, who completed a 6-month follow-up, were compared with 35 eyes of 35 consecutive patients undergoing DSAEK for Fuchs endothelial dystrophy or pseudophakic bullous keratopathy. Main outcome measures included best-corrected visual acuity (in logarithm of the minimal angle of resolution [logMAR] units) and endothelial cell density within a 6-month follow-up.
Results
Best-corrected visual acuity increased from 0.70 ± 0.48 logMAR and 0.75 ± 0.32 logMAR before surgery to 0.21 ± 0.14 logMAR and 0.48 ± 0.19 logMAR 3 months after DMEK and DSAEK ( P < .001), respectively, and to 0.17 ± 0.12 logMAR and 0.36 ± 0.15 logMAR 6 months after DMEK and DSAEK ( P < .001), respectively. Endothelial cell density decreased from 2575 ± 260 cells/mm 2 and 2502 ± 220 cells/mm 2 before surgery to 1498 ± 244 cells/mm 2 and 1778 ± 420 cells/mm 2 3 months after DMEK and DSAEK ( P < .001), respectively, and to 1520 ± 299 cells/mm 2 and 1532 ± 495 cells/mm 2 6 months after DMEK and DSAEK ( P = .483), respectively. Central corneal thickness decreased from 652 ± 92 μm before surgery to 517 ± 45 μm 6 months after DMEK, and from 698 ± 137 μm before surgery to 618 ± 66 μm 6 months after DSAEK.
Conclusions
DMEK provided faster and more complete visual rehabilitation when compared with DSAEK. However, there were no significant differences concerning endothelial cell survival within a 6-month follow-up.
It has been more than 100 years since Eduard Zirm performed the first penetrating keratoplasty (PK), a full-thickness replacement of the diseased cornea. Within the last decade PK has been widely replaced by new lamellar techniques such as anterior and posterior lamellar keratoplasty. This was possible because most patients who need corneal surgery suffer from diseases that are confined to 1 layer of the cornea; for example, more than one-third (37%) of the patients undergoing keratoplasty suffer from disorders of the corneal endothelium, such as Fuchs corneal endothelial dystrophy or pseudophakic/aphakic bullous keratopathy.
The first attempt to perform “posterior lamellar keratoplasty” (PLK) was described in 1950 by Barraquer, who conducted PLK after creating a corneal flap. In modern history of PLK, Melles described sutureless PLK in 1998, using an air bubble for fixation of the posterior lamella. In 2001, Terry introduced endothelial keratoplasty (EK) and coined the term “deep lamellar endothelial keratoplasty” (DLEK). A further improvement of EK was described in 2005 by Price, who performed “Descemet stripping endothelial keratoplasty” (DSEK), followed 1 year later by Gorovoy, who used a microkeratome and called this technique “Descemet stripping automated endothelial keratoplasty” (DSAEK). In the above-mentioned procedure, the diseased endothelium and Descemet membrane (DM) of a host is replaced with posterior corneal stroma, DM, and endothelium of a donor. Recently, “Descemet membrane endothelial keratoplasty” (DMEK) was described by Melles, allowing transplantation of an isolated endothelium–Descemet membrane layer (EDM) without adherent corneal stroma. Therefore, DMEK is the only technique that fully retains the anatomy of the recipient’s cornea.
Main outcome measures that define the success of a surgical technique for corneal replacement are the functional outcome as well as endothelial survival. Several studies have shown that DSAEK and DMEK offer significant advantages over PK with respect to postoperative visual outcome and postoperative astigmatism, as well as providing faster functional rehabilitation. PK might be superior to DSAEK or DMEK, with respect to endothelial cell survival in the early postoperative period. Mid-term results, however, show comparable endothelial cell survival between PK and DSAEK or DMEK. A comparison of visual outcome and endothelial cell survival between DSAEK and DMEK has not been previously described.
The aim of this study was to compare the visual outcome and endothelial cell survival of patients having undergone DSAEK or DMEK.
Methods
Patients
Thirty-eight eyes of 38 consecutive patients undergoing DMEK between August 27, 2009 and December 17, 2009, who completed a 6-month follow-up, were included in this study. These patients were compared with 35 eyes of 35 consecutive patients undergoing DSAEK between August 7, 2008 and March 25, 2009, after having been matched with the DMEK patients, with respect to diagnosis and donor characteristics. Indications for surgery were Fuchs endothelial dystrophy (n = 34 and n = 28 in DMEK and DSAEK, respectively) and pseudophakic bullous keratopathy (n = 4 and n = 7 in DMEK and DSAEK, respectively) ( Table 1 ). Patients with other ocular pathologies were not included in this study. All patients received either a graft prepared from a corneoscleral button that had been stored in Optisol-GS (Bausch & Lomb, Irvine, California, USA) at 4 C (short-term-cultured graft) or a graft prepared from a corneoscleral button that had been stored in Dulbecco’s modified Eagle medium (DMEM) containing streptomycin and penicillin (Biochrom, Berlin, Germany) as well as fetal calf serum (Linaris, Bettingen am Main, Germany) at 34 C (organ-cultured graft) in coordination with our eye bank.
| DMEK (n = 38) | DSAEK (n = 35) | |
|---|---|---|
| Sex (female:male) | 16:22 | 20:15 |
| Mean age ± SD, y (range) | 68.3 ± 9 (42–85) | 68.1 ± 11 (48–87) |
| Indication, n (%) | ||
| Fuchs endothelial dystrophy | 34 (89%) | 28 (80%) |
| Pseudophakic bullous keratopathy | 4 (11%) | 7 (20%) |
| Surgical procedure | ||
| DMEK/DSAEK | 21 (55%) | 23 (66%) |
| Triple-DMEK/Triple-DSAEK | 17 (45%) | 12 (34%) |
Corneal Donor Tissue
All patients received corneal grafts from eye banks in Europe or the United States. In DMEK, 20 corneoscleral buttons (53%) were short-term cultured in Optisol-GS at 4 C and 18 corneoscleral buttons (47%) were organ-cultured in DMEM at 34 C. In DSAEK, 13 corneoscleral buttons (37%) were short-term cultured in Optisol-GS at 4 C and 22 corneoscleral buttons (63%) were organ-cultured in DMEM at 34 C. There was no statistically significant difference concerning donor age (66 ± 11 years and 69 ± 13 years in DMEK and DSAEK, respectively), storage duration (341 ± 160 hours and 309 ± 158 hours in DMEK and DSAEK, respectively), postmortem time (13 ± 12 hours and 10 ± 9 hours in DMEK and DSAEK, respectively), and endothelial cell density (ECD) of donor corneas (2575 ± 260 cells/mm 2 and 2502 ± 220 cells/mm 2 in DMEK and DSAEK, respectively) between DMEK and DSAEK ( Table 2 ). Published data by Laaser and associates suggests that donor tissue culture conditions have no significant effect on visual outcome and endothelial cell survival.
| DMEK | DSAEK | P Value a | |
|---|---|---|---|
| Donor age (y) | 66 ± 11 | 69 ± 13 | .185 |
| Storage duration (hours) | 341 ± 160 | 309 ± 158 | .310 |
| Postmortem time (hours) | 13 ± 12 | 10 ± 9 | .104 |
| Mean ECD ± SD (cells/mm 2 ) | 2575 ± 260 | 2502 ± 220 | .196 |
a P value is assessed by Mann-Whitney U test for independent samples.
Surgery
All surgeries were performed by 2 surgeons (F.E.K., C.C.) under general anesthesia using the same technique. One day prior to surgery, all patients received a neodymium–yttrium-aluminum-garnet laser iridotomy, in order to avoid pupillary block or Urrets-Zavalia syndrome. Donor preparation was performed immediately prior to transplantation. Donor preparation was successful in all DMEK/DSAEK cases, without any loss of corneoscleral buttons.
Descemet Membrane Endothelial Keratoplasty
The EDM was stripped from the donor corneal stroma by a technique previously described by Kruse, which included several modifications from the original technique described by Melles. After mounting the corneoscleral buttons on a suction block (Hanna trephination system; Moria SA, Antony, France) the endothelium was marked by gentle touch with an 8.0-mm trephine and stained with 0.06% trypan blue (Vision Blue; D.O.R.C. Deutschland GmbH, Berlin, Germany) for 60 seconds. A small strip of submerged EDM peripheral to the mark was removed with a razor blade. The central edge was first lifted with a round blade and then grasped with 2 forceps. By simultaneous centripetal movement of the 2 forceps the EDM was incompletely detached, followed by trephination with an 8-mm trephine and marking the edges with a 1-mm trephine as previously described. For better visualization the EDM was stained with trypan blue for 10 seconds and stripping was completed. Transfer of the graft into the patient’s eye and unfolding was achieved by a standardized technique; due to the elastic properties of DM, the EDM roll, which formed spontaneously, was transferred into a standard intraocular lens injector cartridge (Acri.Tec GmbH, Hennigsdorf, Germany). After marking the epithelium with a 9-mm marker, the patient’s EDM was removed under air using an inverted hook (Price hook; Moria SA) inside the 9-mm marking. The graft was injected into the anterior chamber maintaining the volume of the anterior chamber with the irrigation hand piece (diameter 0.6 mm) (Geuder AG, Heidelberg, Germany) attached to the phaco system (Pharo; A.R.C. Laser GmbH, Nuremberg, Germany) with the intraocular pressure set to 30 mm Hg, which is the lowest possible pressure used by the irrigation/aspiration mode of the phaco system to maintain stability of the anterior chamber. The EDM was positioned centrally using short bursts of balanced salt solution (BSS) and unfolded by injecting a series of subsequent small air bubbles. By enlarging the air bubble the EDM was then flattened out on the surface of the iris and air was completely removed, resulting in shallowing of the anterior chamber. Air was injected underneath the graft until the anterior chamber was completely filled with air, which was left in place for 60 minutes. Upon completion of the surgery, air was reduced to about 50% of the anterior chamber volume.
Descemet Stripping Automated Endothelial Keratoplasty
The preparation of donor corneal lenticules was performed using a Moria ALTK microkeratome (Moria SA) with the blade set to 350-μm depth. Thus, the desired thickness of the posterior donor lenticule was 150 μm. We had previously shown that the actual thickness of the posterior donor lenticule was 191 ± 56 μm (mean ± SD) 1 day after surgery and 100 ± 38 μm (mean ± SD) 6 months after surgery. The stromal side of the corneal lenticule was marked with 3 spots of different size to ensure correct orientation in the anterior chamber of the host. The corneal lenticule was mounted on a suction block (Hanna trephination system; Moria SA) with the endothelial side up, followed by trephination with an 8-mm trephine. Transfer of the graft into the patient’s eye was achieved by using the Busin glide (Moria SA) through a 3.2-mm nasal clear cornea tunnel, as previously described. After marking the epithelium with a 9-mm marker, the patient’s EDM was removed under air using an inverted hook (Price hook; Moria SA) inside the 9-mm marking. The graft was delivered to the patient’s eye using the standardized pull-through technique by Busin : The graft was placed on the plate and pulled into the funnel-shaped part of the Busin glide using a microincision forceps. The Busin glide was then inverted and positioned at the nasal clear cornea tunnel. On the temporal side, a microincision forceps was inserted to pull the graft into the anterior chamber, allowing it to unfold spontaneously. Air was injected underneath the graft until the anterior chamber was completely filled with air, which was left in place for 60 minutes. Upon completion of the surgery, air was reduced to about 50% of the anterior chamber volume.
Triple Procedures
In patients undergoing a triple procedure (endothelial keratoplasty, phacoemulsification, and intraocular lens implantation), phacoemulsification and intraocular lens implantation were performed prior to DMEK/DSAEK surgery. For cataract surgery hyaluronic acid was used as viscoelastic. After intraocular lens implantation and following scarring of DM but prior to insertion of the graft into the anterior chamber, all hyaluronic acid was completely removed. Intracameral acetylcholine chloride (Miochol-E; Novartis Pharma GmbH, Nuremberg, Germany) was used to constrict the pupil prior to DMEK/DSAEK surgery. The patients received either a spherical single-piece acrylic intraocular lens (46 S AcriSmart; Acri.Tec GmbH, Hennigsdorf, Germany) or a multi-piece acrylic AcrySof (MA 60 AC; Alcon Pharma GmbH, Freiburg i. Breisgau, Germany). In DMEK surgery, 17 of 38 patients (45%) underwent a triple DMEK. In DSAEK surgery, 12 of 35 patients (34%) underwent a triple DSAEK.
Main Outcome Measures
Main outcome measures included best-corrected visual acuity (BCVA, logMAR), central corneal thickness (CCT), and endothelial cell density (ECD) within 6 months follow-up. CCT was analyzed by Scheimpflug imaging (Pentacam; Oculus, Wetzlar, Germany) and ECD was analyzed by in vivo confocal microscopy (SeaEagle; HAI Laboratories, Lexington, Massachusetts, USA). A disadvantage of this study is a relatively low number of participants (n = 73) and a relatively short follow-up period of 6 months. Seventeen DMEK patients have been analyzed before in other published literature.
Statistical evaluation was performed using SPSS version 18.0 for Windows (SPSS Inc, Chicago, Illinois, USA). The level of significance was set at P = .05. Because of no normal distribution in all groups of this study, nonparametric tests were used. Differences between groups were assessed by the Mann-Whitney U test. Differences within groups were assessed by the Wilcoxon test.
Results
Visual Outcome
Patients with other ocular comorbidity, besides Fuchs endothelial dystrophy or pseudophakic bullous keratopathy, were not included in this study. All DMEK patients (n = 38) and DSAEK patients (n = 35) completed a 6-month follow-up. Primary graft failure was not observed during follow-up.
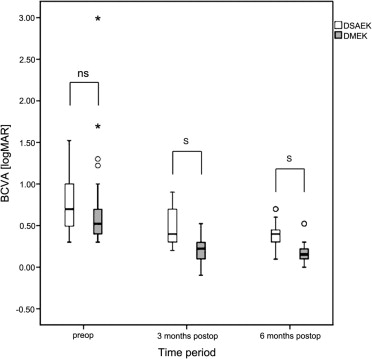
Mean BCVA ± SD in DMEK patients was 0.70 ± 0.48 logMAR preoperatively (n = 38) and increased to 0.21 ± 0.14 logMAR at 3 months (n = 36) and to 0.17 ± 0.12 logMAR at 6 months (n = 38) after surgery. Increase in BCVA within the first 3 months was statistically significant ( P < .001). Between 3 and 6 months after surgery, no further statistically significant increase in BCVA was achieved ( P = .156).
A total of 83% (30/36) of eyes reached a visual acuity of 20/40 or better 3 months after surgery, which increased to 95% (36/38) 6 months after surgery. A total of 36% (13/36) of eyes reached a visual acuity of 20/25 or better 3 months after surgery, which increased to 50% (19/38) 6 months after surgery.
Mean BCVA ± SD in DSAEK patients was 0.75 ± 0.32 logMAR preoperatively (n = 35) and increased to 0.48 ± 0.19 logMAR at 3 months (n = 32) and to 0.36 ± 0.15 logMAR at 6 months (n = 35) after surgery. Increase in BCVA within the first 3 months and between 3 and 6 months after surgery was statistically significant ( P < .001).
A total of 28% (9/32) of eyes reached a visual acuity of 20/40 or better 3 months after surgery, which increased to 43% (15/35) 6 months after surgery. No patient reached a visual acuity of 20/25 or better 3 months after surgery. Six percent (2/35) of eyes reached a visual acuity of 20/25 or better 6 months after surgery.
Preoperative BCVA between DMEK and DSAEK patients was not significantly different ( P = .185). BCVA 3 and 6 months after surgery showed statistically significant difference between DMEK and DSAEK ( P < .001) ( Figure 1 , Table 3 ).
| DMEK a | DSAEK a | P Value b | |
|---|---|---|---|
| Preoperative | 0.70 ± 0.48 | 0.75 ± 0.32 | .185 |
| 3 months postoperative | 0.21 ± 0.14 | 0.48 ± 0.19 | <.001 |
| 6 months postoperative | 0.17 ± 0.12 | 0.36 ± 0.15 | <.001 |
a Values are given as mean ± standard deviation in logMAR (logarithm of the minimal angle of resolution).
b P value is assessed by Mann-Whitney U test for independent samples.
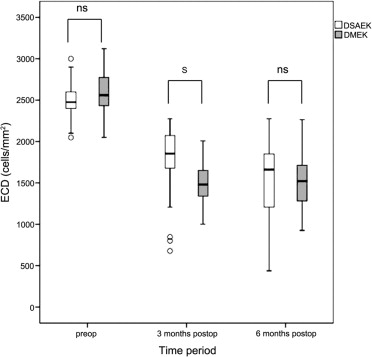
Endothelial Cell Density
Mean preoperative ECD ± SD of donor corneas in DMEK patients was 2575 ± 260 cells/mm 2 (n = 38) and decreased to 1498 ± 244 cells/mm 2 at 3 months (n = 36) and to 1520 ± 299 cells/mm 2 at 6 months (n = 38) after surgery. Decrease in ECD within the first 3 months was statistically significant ( P < .001). Between 3 and 6 months after surgery, no further statistically significant difference in ECD was observed ( P = .494). Mean loss rate of ECD was 41% 6 months after surgery.
Mean preoperative ECD ± SD of donor corneas in DSAEK patients was 2502 ± 220 cells/mm 2 (n = 35) and decreased to 1778 ± 420 cells/mm 2 at 3 months (n = 32) and to 1532 ± 495 cells/mm 2 at 6 months (n = 35) after surgery. Decrease in ECD within the first 3 months and between 3 and 6 months after surgery was statistically significant ( P < .001). Mean loss rate of ECD was 39% 6 months after surgery.
The difference of preoperative ECD between DMEK and DSAEK patients was not statistically significant ( P = .196). ECD 3 months after surgery showed statistically significant difference between DMEK and DSAEK ( P < .001). Six months after surgery, no statistically significant difference was observed ( P = .483) ( Figure 2 , Table 4 ).