Purpose
To evaluate the functional and morphologic outcome of Descemet membrane endothelial keratoplasty (DMEK) combined with phacoemulsification and intraocular lens implantation in patients suffering from endothelial dysfunction and cataract.
Design
Retrospective, single-center, consecutive case series.
Methods
Triple-DMEK (DMEK with simultaneous cataract surgery) was performed in 61 consecutive eyes of 56 patients using corneal donor tissue pre-stored in either short-term culture (Optisol-GS) at 4 C or organ culture (Dulbecco’s modified Eagle’s medium, CorneaMax medium) at 34 C. Main outcome measures included the number of air injections necessary for graft attachment as well as best-corrected visual acuity (BCVA [logMAR]), central corneal thickness (CCT), endothelial cell density (ECD), refractive spherical equivalent, refractive cylinder, and topographic cylinder at 1, 3, and 6 months postoperatively.
Results
BCVA increased from 0.6 ± 0.23 logMAR preoperatively (n = 54) to 0.19 ± 0.22 logMAR at 6 months (n = 27) after surgery ( P ≤ .05). ECD of donor corneas decreased from 2573 ± 235 cells/mm 2 (n = 61) to 1550 ± 326 cells/mm 2 (n = 29) after 6 months ( P ≤ .05). CCT decreased from 651 ± 69 μm (n = 54) preoperatively to 521 ± 65 μm (n = 27) after 6 months ( P ≤ .05). Refractive spherical equivalent was −0.3 ± 2.8 D (n = 27) preoperatively and 0.9 ± 1.5 D 6 months (n = 27) after surgery. A total of 54.5% of eyes were within 1 D of emmetropia (n = 12) and 77.3% were within 2 D of emmetropia (n = 17) 6 months (n = 22) after surgery. Refractive cylinder was −0.9 ± 1.0 D preoperatively (n = 49) and −1.5 ± 1.0 D 6 months (n = 23) after surgery. The change in refractive cylinder within the first month was statistically significant ( P ≤ .05; Wilcoxon test). Topographic cylinder was 2.1 ± 1.7 D preoperatively (n = 58) and 1.7 ± 1.1 D 6 months (n = 28) after surgery. Between 3 and 6 months a significant change in topographic cylinder towards lower values was measured ( P ≤ 0.05; Wilcoxon test). Optimized spherical results were achieved by selecting intraocular lenses based on a hyperopic shift of −0.75 D.
Conclusion
DMEK combined with cataract surgery (triple procedure) can routinely be performed in cases of endothelial dystrophy and cataract. The addition of cataract surgery to DMEK had no adverse effect on endothelial function or graft adhesion and did not increase the likelihood of postoperative complications.
New techniques for lamellar corneal surgery have recently been described allowing for selective intervention at the level of the corneal endothelium. In routine corneal surgery, deep lamellar endothelial keratoplasty (DLEK), small-incision DLEK, and Descemet stripping (automated) endothelial keratoplasty (DSEK/DSAEK) have all been used to replace the host’s diseased corneal endothelium and Descemet membrane with a graft consisting of posterior corneal stroma, Descemet membrane, and endothelium. Several studies have shown that in the hands of an experienced surgeon DSAEK is superior to penetrating keratoplasty in respect to postoperative astigmatism and function. Recently, Descemet membrane endothelial keratoplasty (DMEK) has been described, allowing transplantation of the isolated endothelium–Descemet membrane layer without adherent corneal stroma. Fuchs endothelial dystrophy is one of the main diagnoses necessitating DSAEK or DMEK. Moreover, patients with Fuchs endothelial dystrophy frequently suffer from coexisting cataract. Cataract surgery can either be performed independently from lamellar keratoplasty (before or after the surgery) or can be combined with keratoplasty. Cataract surgery has successfully been combined with penetrating keratoplasty since the 1970s and became popular as the triple procedure. Lately the combination of endothelial keratoplasty (eg, DSAEK) with cataract surgery was named the “new triple procedure.” There is an ongoing discussion in the literature whether a sequential or concurrent (triple procedure) approach leads to superior postoperative results. Advantages of the triple procedure seem to be faster visual rehabilitation and no further endothelial damage induced by sequential cataract surgery. Although a triple procedure can easily be performed by an experienced surgeon, the predictability of the postoperative refractive outcome is still limited. In classic triple procedure, penetrating keratoplasty induces changes of the anterior and posterior curvature with reduced predictability because of alteration of the keratometric readings needed for intraocular lens calculation. This leads to the likelihood of postoperative refractive errors and anisometropia. DSAEK induces no significant changes in corneal topography and therefore the refractive outcome after triple-DSAEK is much more predictable, although a mild postoperative hyperopic shift was observed.
Initial results after sole DMEK are equivalent or even superior to that of DSAEK, possibly because of less alteration of the posterior surface of the cornea.
The purpose of this study was to describe the results of triple-DMEK, including postoperative best-corrected visual acuity (BCVA), refractive outcome, endothelial cell density (ECD), central corneal thickness (CCT), and detachment rate within a follow-up of 6 months.
Methods and Patients
Patients
Triple-DMEK (DMEK with simultaneous cataract surgery) was performed in 61 consecutive eyes of 56 patients (37 eyes of 34 male patients, and 24 eyes of 22 female patients) aged between 42 and 79 years (mean age 66.3 ± 12.4 years). Indications for surgery were Fuchs endothelial dystrophy (n = 60) and bullous keratopathy after failed DMEK (n = 1). Thirty-two eyes received an isolated endothelium–Descemet membrane layer prepared from a corneoscleral button that had been stored in Optisol-GS (Bausch & Lomb, Irvine, California, USA) at 4 C for 243 ± 79 hours. Twenty-nine eyes received an isolated endothelium–Descemet membrane layer from a corneoscleral button that had been stored in Dulbecco’s modified Eagle’s medium (DMEM) containing streptomycin and penicillin (Biochrom, Berlin, Germany) as well as fetal calf serum (Linaris, Bettingen am Main, Germany) at 34 C for 397 ± 155 hours. In all eyes DMEK was combined with phacoemulsification and implantation of an intraocular lens. In 40 eyes a spherical single-piece acrylic intraocular lens (46 S AcriSmart; Acri. Tec GmbH, Hennigsdorf, Germany) and in 21 eyes a multi-piece acrylic intraocular lens (AcriSof MA 60 AC; Alcon Pharma, Fort Worth, Texas, USA) was implanted.
Intraocular Lens Power Calculation
Axial length, keratometry, and anterior chamber depth were measured using the IOLMaster (V.4.08; Carl Zeiss Meditec, Jena, Germany). The keratometry readings obtained by the IOLMaster were compared with keratometry readings obtained by the Zeiss keratometer (Carl Zeiss Meditec). Intraocular lens power calculation was performed by the IOLMaster using the Haigis formula in all patients. In 3 patients intraocular lens power calculation had to be performed by measuring axial length using an A-scan (CinescanS; Haag-Streit Deutschland GmbH, Wedel, Germany) because of media opacification.
The target refraction was chosen as close as possible to emmetropia. In 5 patients a target refraction of −3.0 diopters (D) was chosen to satisfy the patients’ desire to read without correction. A hyperopic shift was taken into account in all patients, because of previously published data. The mean target refraction of all eyes was −0.53 ± 0.95 D (n = 61).
Surgery
DMEK procedures were performed by 2 experienced surgeons (F.E.K., C.C.) using the same technique. One day before surgery all patients received a neodymium–yttrium-aluminum-garnet laser iridotomy at the 12-o’clock and the 6-o’clock position. It is important to ensure a sufficient size of the iridotomy and ensure removal of the pigment layers. Immediately prior to transplantation the endothelium–Descemet membrane complex was stripped from the donor corneal stroma by a technique published by Kruse and associates, which included several modifications from the original technique described by Melles and associates. In all cases cataract extraction with phacoemulsification and intraocular lens implantation was performed prior to DMEK surgery. In none of our patients was a clear lens extraction performed. Cataract surgery was performed only in cases with moderate to advanced cataract density (nuclear and cortical). The primary incision site was at the 12-o’clock position and 2 additional side-port incisions at the 3-o’clock and 9-o’clock position were made. The same incision was used for delivery of the intraocular lens and the graft in all patients. Visibility into the anterior chamber was impaired in some patients because of stromal edema. In these patients we did remove the epithelium during surgery and 3 patients received glycerol 10% eye drops in addition, to reduce corneal edema. For cataract surgery hyaluronic acid (Z-Hyalon plus; Acri.Tec GmbH) was used. Following intraocular lens implantation, which was performed with viscoelastic in the bag, the remaining viscoelastic that was still in the syringe was injected in the chamber angle to push down the iris. Since the anterior chamber was filled with Z-Hyalon plus (Acri.Tec GmbH, Hennigsdorf, Germany), scoring of the Descemet membrane was very easy. With the help of the inverted Price hook, the Descemet membrane was scored. Then the initial detachment towards the center was performed for about 1 mm. Then viscoelastic was removed and the anterior chamber was filled with air following injection of Miochol (Novartis Pharma GmbH, Nürnberg, Germany) to narrow the pupil. In contrast to the regular cases, the cataract surgery in which adrenalin (1 mg/500 mL) was used in the irrigation solution, we used pure balanced salt solution in all cases with sufficient mydriasis in order to allow best constriction of the pupil after Descemet membrane removal. Intracameral acetylcholine chloride (Miochol-E; Novartis, Nuremberg, Germany) was used to constrict the pupil prior to DMEK surgery.
After mounting the corneoscleral buttons on a suction block (Hanna trephination system; Moria Instruments, Antony, France), the endothelium was marked by gentle touch with an 8.0-mm trephine and stained with 0.06% trypan blue (Vision Blue; D.O.R.C. Deutschland GmbH, Berlin, Germany) for 60 seconds. A small strip of submerged endothelium–Descemet membrane layer peripheral to the mark was removed with a razor blade. The central edge was first lifted with a round blade and then grasped with 2 forceps. By simultaneous centripetal movement of the 2 forceps the endothelium–Descemet membrane layer was incompletely detached, followed by trephination with an 8-mm trephine and marking the edges with a 1-mm trephine as previously described. For better visualization the endothelium–Descemet membrane layer was stained with trypan blue for 10 seconds and stripping was completed. Transfer of the graft into the patient’s eye and unfolding was achieved by a standardized technique: because of the elastic properties of the Descemet membrane, the endothelium–Descemet membrane roll, which formed spontaneously, was transferred into a standard intraocular lens injector cartridge (Acri.Tec GmbH). The graft was injected into the anterior chamber, maintaining the volume of the anterior chamber with the irrigation handpiece (diameter 0.6 mm) of ARC phaco system set in irrigation/aspiration mode with a hydrostatic pressure of 30 mm Hg (A.R.C. Laser GmbH, Nürnberg, Germany). The endothelium–Descemet membrane layer was positioned centrally using short bursts of balanced salt solution and unfolded by injecting a series of subsequent small air bubbles. By enlarging the air bubble the endothelium–Descemet membrane layer was then flattened out on the surface of the iris and air was completely removed, resulting in flattening of the anterior chamber. Air was injected underneath the graft until the anterior chamber was completely filled with air, which was left in place for 30 minutes. Upon completion of the surgery, air was reduced to about 50% of the anterior chamber volume.
Postoperative Follow-Up
Patients were examined before as well as 1, 3, and 6 months after surgery. BCVA (logMAR), refractive cylinder, and refractive spherical equivalent were assessed. Topographic cylinder was measured using a topographic modeling system (TMS-4, version 3.5 D; Tomey, Erlangen, Germany). CCT was quantified by Scheimpflug imaging (Pentacam; Oculus, Wetzlar, Germany) and ECD was evaluated by in vivo confocal microscopy (SeaEagle; HAI Laboratories, Lexington, Massachusetts, USA).
The decision for additional air injections in the postoperative follow-up was based upon slit-lamp biomicroscopy and the results of examinations using the SL-OCT (slit-lamp OCT; Heidelberg Engineering, Heidelberg, Germany). SL-OCT was routinely performed every third day within the first 2 weeks after surgery and included at least 2 sections in each of the 4 quadrants. Rebubbling was performed in all patients with significant corneal edema over more than 3 clock hours in conjunction with a detachment of the endothelium–Descemet membrane layer of more than 100 μm in depth. Air was injected under topical anesthesia, filling the chamber completely for 1 hour and removing the air bubble to 50% of the volume of the anterior chamber. Special care was taken to ensure correct positioning of the bubble immediately after surgery by keeping the patients in a supine or otherwise fixed position in the hospital for 36 hours after the procedure.
Statistical Evaluation
Statistical evaluation was performed using SPSS version 17.0 (SPSS Inc, Chicago, Illinois, USA). The normal distribution of all tested values was assessed by using the method of Kolmogorov-Smirnov. Because of some cases of non-normal distribution, sample differences between samples in each group were assessed by the Wilcoxon test. Sample differences between groups were assessed by the Mann-Whitney U test. The significance level was set at α = 0.05.
Results
Visual Outcome
The BCVA achieved following DMEK is shown in Figure 1 . For final analysis 6 patients were excluded because of preexisting conditions limiting visual potential: macular degeneration (n = 3), epiretinal gliosis with cystoid macular edema (n = 1), advanced glaucomatous optic atrophy (n = 1), and prior retinal surgery because of retinal detachment (n = 1). BCVA was 0.6 ± 0.23 logMAR preoperatively (n = 54) and increased to 0.31 ± 0.18 logMAR at 1 month (n = 47), to 0.23 ± 0.23 logMAR at 3 months (n = 37), and to 0.19 ± 0.22 logMAR at 6 months (n = 27) after surgery. Increase in BCVA within the first month, between 1 month and 3 months ( P ≤ .005; Wilcoxon test), and between 3 months and 6 months ( P ≤ .05; Wilcoxon test) was statistically significant ( Figure 1 ). A total of 36.2% of eyes reached a visual acuity of 20/40 or better after 1 month (n = 17), which increased to 67.6% after 3 months (n = 25) and to 81.4% after 6 months (n = 22).
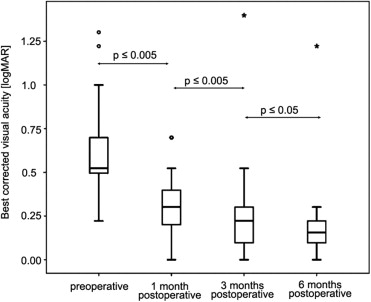
A total of 21.3% of eyes reached a visual acuity of 20/25 or better after 1 month (n = 10), which increased to 32.4% after 3 months (n = 12) and to 37.0% after 6 months (n = 10).
Endothelial Cell Density
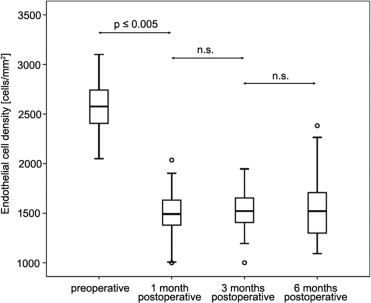
The mean preoperative ECD of donor corneas was 2573 ± 235 cells/mm 2 (n = 61) according to the eye banks that had processed the tissue. After 1 month the ECD had decreased to 1507 ± 213 cells/mm 2 (n = 43). This decrease was statistically significant when compared to preoperative values ( P < .005; Wilcoxon test). At 3 months an ECD of 1539 ± 228 cells/mm 2 (n = 41) and at 6 months an ECD of 1550 ± 326 cells/mm 2 (n = 29) was observed. The decrease of ECD between 1 month and 3 months as well as 3 months and 6 months was not statistically significant ( P = n.s.; Wilcoxon test) ( Figure 2 ) .
Central Corneal Thickness
Prior to surgery the mean CCT was 651 ± 69 μm (n = 54). CCT decreased to 540 ± 90 μm (n = 41) at 1 month, to 514 ± 51 μm (n = 39) at 3 months, and to 521 ± 65 μm (n = 27) after 6 months. The decrease of CCT within the first month was statistically significant ( P ≤ .005; t test). In the follow-up until 6 months no further statistically significant decrease was noted ( P = n.s., t test) ( Figure 3 ) .
Refractive Outcomes
For final analysis, 6 patients were excluded for examining the refractive spherical equivalent and the refractive cylinder because of preexisting conditions limiting visual potential (see above).
Refractive Spherical Equivalent
The mean refractive spherical equivalent was −0.3 ± 2.8 D preoperatively (n = 54), and 0.2 ± 1.1 D 1 month (n = 43), 0.5 ± 1.8 D 3 months (n = 37), and 0.9 ± 1.5 D 6 months (n = 27) after surgery.
A significant change in refractive spherical equivalent was noted between 1 month and 3 months, with no further significant change in a follow-up of 6 months ( P = n.s., Wilcoxon test) ( Figure 4 ) . Within the first 6 months a trend towards a small hyperopic shift was noticed. A total of 70.0% of eyes were within 1 D of emmetropia (n = 28) and 87.5% were within 2 D of emmetropia (n = 35) 1 month after surgery. Three months after triple-DMEK, 69.7% of eyes were within 1 D of emmetropia (n = 23) and 87.9% were within 2 D of emmetropia (n = 29). After 6 months 54.5% of eyes were within 1 D of emmetropia (n = 12) and 77.3% were within 2 D of emmetropia (n = 17).
Refractive Cylinder
Refractive cylinder was −0.9 ± 1.0 D preoperatively (n = 49), and −1.5 ± 1.4 D 1 month (n = 42), −1.3 ± 0.9 D 3 months (n = 33), and −1.5 ± 1.0 D 6 months (n = 23) after surgery. Change in refractive cylinder within the first month was statistically significant ( P ≤ .05; Wilcoxon test). Further changes during the 6-month follow-up period were not statistially significant ( P = n.s., Wilcoxon test) ( Figure 5 ) .
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


