Purpose
To study the effect of different protocols of collagen cross-linking on visual, refractive, and tomographic parameters in patients with progressive keratoconus.
Design
Prospective randomized interventional study.
Methods
In this study, 138 eyes of 138 patients with progressive keratoconus underwent corneal collagen cross-linking (CXL). Following detailed preoperative examination, Group I underwent conventional cross-linking (36 patients, 3 mW/cm 2 for 30 min); Group II (36 patients, 9 mW/cm 2 for 10 min), Group III (33 patients, 18 mW/cm 2 for 5 min), and Group IV (33 patients, 30 mW/cm 2 for 3 min) underwent accelerated cross-linking. Changes in corrected distance visual acuity (CDVA), spherical equivalent (SE), flat keratometry, steep keratometry, thinnest pachymetry, specular microscopy, and demarcation line were studied at 6 and 12 months.
Results
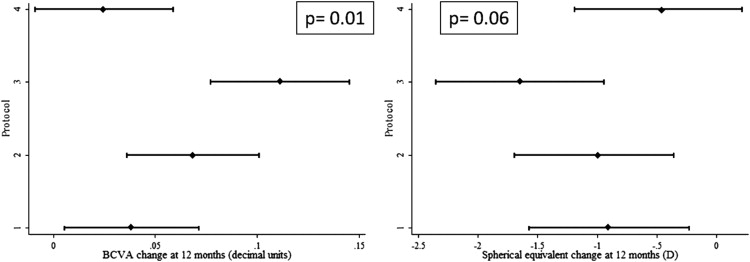
Improvement in the mean CDVA and SE were statistically significant in all groups except Group IV ( P = .15 at 6 months, P = .17 at 12 months), with Group III ( P = .01 at 6 and 12 months) showing the best results. Flattening of steep and flat keratometry was significant in Groups I ( P = .01) and II ( P = .01) as compared to the other groups. There was no significant difference in the pachymetry or specular microscopy in any of the groups. Groups I and II demonstrated a good demarcation line when compared to other groups.
Conclusion
Conventional CXL (Group I) and accelerated CXL with irradiations of 9 mW/cm 2 (Group II) and 18 mW/cm 2 (Group III) showed better visual, refractive, and tomographic improvements at the end of 12 months.
Keratoconus is characterized by biomechanical instability and thinning of the corneal stroma as a result of weak collagen fibers, which leads to progressive irregular myopic astigmatism, higher-order aberrations, and corneal scarring, resulting in decreased visual acuity. In the early stages spectacle correction, contact lenses, and intrastromal corneal ring segments can aid in visual rehabilitation, whereas penetrating and lamellar keratoplasty become necessary in the advanced stages. However, none of these treatment modalities stabilize the disease or stop the progression of ectasia.
Corneal collagen cross-linking (CXL) was first performed at the Dresden Technical University in 1998 and its use in keratoconus was first reported by Wollensak and associates in 2003. CXL increases the corneal collagen cross-links, thereby strengthening the cornea and leading to stabilization of the ectasia and flattening of the cornea, which in turn can cause a reduction in myopia and astigmatism. There have been various modifications to the conventional CXL like increasing the intensity of ultraviolet A (UV-A) irradiation and shortening the exposure time (accelerated CXL; ACXL) without altering the total energy delivered. Another modification has been to perform the CXL through an intact epithelium (transepithelial CXL) with less discomfort to the patient and reduced postoperative complications. Though the different protocols have been evaluated individually, there are no comparative studies with conventional CXL. In this study, we evaluate the effectiveness and safety of conventional CXL and ACXL in a subset of our patients.
Patients and Methods
A written informed consent for participating in the study was obtained from all patients undergoing the procedure. The study was approved by the Narayana Nethralaya ethics committee and was performed according to the tenets of the Declaration of Helsinki.
This was a prospective interventional study of 138 eyes of 138 patients with progressive keratoconus documented by serial tomography for at least 6 months, corneal thickness >400 μm at the thinnest location, and age between 15 and 30 years. We randomized the subjects into the 4 groups according to the alternating assignment method. In our study, an increase in the steep K-value by more than 1.0–1.5 diopters (D), a corresponding change (>1.0–1.5 D) in the subjective refraction, or a 5% or more decrease in the thinnest pachymetry in the preceding 6 months was defined as “progression.”
Eyes with <400 μm corneal thickness at the thinnest point, concurrent corneal infections, or central or paracentral scarring and those with a history of herpetic keratitis were excluded from the study. All patients underwent a detailed ophthalmic examination including uncorrected distance visual acuity (UCDVA), corrected distance visual acuity (CDVA), and subjective acceptance. Visual acuity was recorded using the Snellen chart and was later converted to decimal values. All patients underwent corneal tomography using the Pentacam (Oculus, Inc, Lynnwood, Washington, USA), a rotating Scheimpflug camera system for anterior segment analysis, which measures topography and elevation of the anterior and posterior corneal surface and the corneal thickness. Simulated keratometric (Sim K) values represented by flat and steep keratometry (K1 and K2, respectively) of the central cornea and minimum pachymetry values were derived from the Pentacam and the corneal thickness was confirmed with ultrasound pachymetry. Spectral-domain optical coherence tomography (SD OCT) was performed using a handheld device (Bioptigen Inc, Research Triangle Park, North Carolina, USA) in the postoperative period to look for the demarcation line. All patients underwent the above tests at baseline and at all subsequent visits.
Based on the Amsler-Krumeich classification, patients with grade 1 and 2 progressive keratoconus underwent conventional CXL (Group I) or one of the protocols of ACXL (Groups II, III, and IV) after removal of the epithelium (epi-off).
Surgical Procedure
All procedures were performed under topical proparacaine hydrochloride 0.5% eye drops under sterile precautions in the operating room. In all groups, the central 8 mm of the corneal epithelium was debrided using an epithelial scraper.
Riboflavin drops
Riboflavin 0.1% solution (10 mg riboflavin-5-phosphate in 10 mL dextran-T-500 20% solution) was applied as a photosensitizer every 2 minutes for the first 30 minutes in all groups.
Ultraviolet-A irradiation
In all groups, once permeation of riboflavin through the cornea using a Portable Slit Lamp (PSL; Reichert, Depew, New York, USA) was confirmed, UV-A irradiation of wavelength 365 nm was initiated using the Avedro KXL system (Waltham, Massachusetts, USA). Application of riboflavin drops every 2 minutes during the irradiation was used to maintain its necessary concentration. The UV-A irradiation intensity used in different groups is as follows: Group I (conventional CXL): 3 mW/cm 2 for 30 minutes; Group II: 9 mW/cm 2 for 10 minutes; Group III: 18 mW/cm 2 for 5 minutes; Group IV: 30 mW/cm 2 for 3 minutes.
A 9 mm beam was used, and care was taken to avoid any damage to the limbus by using a limbal guard made of polymethyl methacrylate. A silicone hydrogel bandage contact lens (Pure Vision; Bausch and Lomb, Rochester, NY) was applied following the treatment and removed on the third postoperative day or once the epithelium healed.
Postoperative treatment included prednisolone acetate 1% eye drops in tapering doses for 3 weeks, moxifloxacin hydrochloride 0.5% eye drops 4 times a day for 1 week, nepafenac 0.1% eye drops 3 times a day for 3 days, and topical artificial tears supplements 4 times a day for 3 months.
Statistical Analyses
All continuous variables were represented as mean and standard deviation (SD). One-way analysis of variance was used to evaluate the differences in the preoperative values of the parameters between the groups. The main outcome measure was the difference between the preoperative and postoperative parameters evaluated at 6 and 12 months post procedure. As the change in postoperative parameters was significantly related to the preoperative values, analysis of covariance models were used to adjust for the differences in the preoperative values during the comparison of outcomes between the various groups. Statistical analyses were performed using the commercial software (Stata ver. 12.0; StataCorp, College Station, Texas, USA). P value less than .05 was considered statistically significant.
Results
A total of 138 eyes of 138 patients (36 each in Groups I and II; 33 each in Groups III and IV) were included in the study; 82 patients (59.4%) were female and 56 (40.6%) male. Mean (± SD) age of the patients was 22.8 ± 5.0 years (range: 14–33 years) in Group I, 23.1 ± 4.7 years (range: 13–33 years) in Group II, 19.9 ± 5.8 years (range: 10–32 years) in Group III, and 24.2 ± 7.1 years (range: 11–45 years) in Group IV. Mean follow-up time was 15.32 ± 3.39 months (range: 12–19 months). Table 1 shows the preoperative spherical equivalent (SE), CDVA, K1, K2, pachymetry, and endothelial cell density values of the patients in each of the 4 groups; the differences were statistically significant for CDVA (between Group I and II, and Group I and IV) and pachymetry values (between Group I and III). Tables 2 and 3 show the change in the values at 6 and 12 months postoperative follow-up. Figures 1 , 2 , and 3 show the mean change in postoperative parameter values (with 95% confidence interval) at 1 year follow-up.
| Preoperative Parameters | Group I (n = 36) | Group II (n = 36) | Group III (n = 33) | Group IV (n = 33) | P Value |
|---|---|---|---|---|---|
| Spherical equivalent | −3.51 ± 4.91 | −4.27 ± 3.27 | −3.74 ± 4.01 | −4.17 ± 4.58 | .85 |
| CDVA (decimal) | 0.29 ± 0.20 | 0.15 ± 0.13 | 0.20 ± 0.15 | 0.17 ± 0.14 | .002 |
| K1 (D) | 46.2 ± 2.6 | 45.9 ± 3.3 | 45 ± 2.7 | 45.8 ± 3.6 | .39 |
| K2 (D) | 50.5 ± 4.2 | 49.9 ± 3.8 | 48.6 ± 3.5 | 49.4 ± 4.2 | .23 |
| Thinnest pachymetry (μm) | 448 ± 26 | 450 ± 18 | 468 ± 34 | 460 ± 36 | <.01 |
| Specular microscopy (cell/mm 3 ) | 2760 ± 285 | 2669 ± 200 | 2733 ± 214 | 2686 ± 303 | .41 |
| Change at 6 Months Postoperative | Group I (n = 36) | Group II (n = 36) | Group III (n = 33) | Group IV (n = 33) | P Value |
|---|---|---|---|---|---|
| Spherical equivalent | −0.23 (−0.79 to 0.34) | −0.30 (−0.86 to 0.26) | −0.75 (−1.3 to −0.16) | −0.13 (−0.72 to 0.45) | .46 |
| CDVA (decimal) | 0.02 (−0.01 to 0.05) | 0.02 (−0.01 to 0.06) | 0.01 (−0.02 to 0.04) | 0.01 (−0.02 to 0.04) | .89 |
| K1 (D) | 0.46 (0.18–0.72) | 0.39 (0.13–0.66) | 0.13 (−0.14 to 0.41) | −0.03 (−0.31 to 0.24) | .004 |
| K2 (D) | 0.73 (0.33–1.13) | 0.32 (−0.07 to 0.72) | 0.20 (−0.21 to 0.62) | −0.03 (−0.45 to 0.37) | .06 |
| Thinnest pachymetry (μm) | 21 (16–27) | 14 (8–19) | 13 (7–19) | 3 (−2 to 9) | <.001 |
| Specular microscopy (cell/mm 3 ) | 98 (23–173) | 147 (73–222) | 100 (22–178) | 94 (16–172) | .73 |
| Change at 12 Months Postoperative | Group I (n = 36) | Group II (n = 36) | Group III (n = 33) | Group IV (n = 33) | P Value |
|---|---|---|---|---|---|
| Spherical equivalent | −0.85 (−1.44 to −0.25) | −1 (−1.65 to −0.46) | −1.68 (−2.30 to −1.06) | −0.49 (−1.11 to 0.12) | .06 |
| CDVA (decimal) | 0.04 (0–0.07) | 0.06 (0.03–0.1) | 0.10 (0.07–0.14) | 0.02 (−0.005 to 0.06) | .01 |
| K1 (D) | 0.91 (0.56–1.26) | 0.54 (0.19–0.88) | 0.29 (−0.06 to 0.66) | 0.15 (−0.20 to 0.52) | .01 |
| K2 (D) | 1.32 (0.84–1.79) | 0.67 (0.2–1.13) | 0.52 (0.03–1.02) | 0.18 (−0.30 to 0.68) | .01 |
| Thinnest pachymetry (μm) | 27 (22–33) | 19 (13–25) | 16 (9–22) | 7 (0.5–13) | <.001 |
| Specular microscopy (cell/mm 3 ) | 166 (96–236) | 187 (116–257) | 162 (88–234) | 215 (141–288) | .73 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


