Critical Periods for Visual Development and the Timing of Congenital Cataract Surgery
Eileen E. Birch
Anna R. O’Connor
CRITICAL PERIODS
The influence of early experience on development has been and continues to be a dominant theme in developmental neurobiology. The explosion of interest in visual system development was kindled in the early 1960s by the investigations of David Hubel and Torsten Wiesel into the complex organization of the primary visual cortex where, among other features, they were the first to describe the organization of monocular connections between the lateral geniculate nucleus and layer 4C of the visual cortex into ocular dominance columns and the higher-level binocular connections that provide sensitivity to binocular disparity.1,2 Following this extremely important initial work, they turned to the question of neurodevelopment, investigating how the highly specific response properties of cortical cells emerged during postnatal development.1,2
Their research led to three influential ideas. First, there is a critical period for visual development that requires normal postnatal visual experience. Their earliest investigations looked at the effects of depriving one eye of vision during the first weeks of life. In the cat, normal visual experience leads to a visual cortex that has a normal distribution of ocular dominance, some left eye driven cells, some driven by the right eye, and most binocular cells. However, if one eye is deprived of vision during the critical early weeks, the visual cortex develops only cells connected to the nondeprived eye. If this same deprivation is performed at an older age, the critical period for visual development has already ended and there is no effect on ocular dominance. Second, not only is it possible to induce cortical changes by visual deprivation during the critical period, but there is also a critical period during which these changes can be reversed in whole or in part by forcing use of the previously deprived eye. Moreover, the critical period for rehabilitation may extend beyond the critical period for visual development. Third, areas that are normally controlled by the deprived eye are not just empty areas, which lack connections due to disuse. Instead, the areas connected to the deprived eye actually shrink relative to the areas controlled by the normal fellow eye; in other words, there is competition between the eyes for cortical space during the critical period for visual development.
Although ophthalmology was developing an awareness of these important discoveries in neurobiology, there was a long delay before they were translated into clinical practice, particularly for the treatment of unilateral cataracts. As recently as 1980, papers in pediatric ophthalmology stated that there is “virtually no chance of achieving a good visual result” in children with congenital unilateral cataracts.3 In fact, it was not until the publication of two seminal papers in 1981 that pediatric ophthalmology took notice of the importance of critical periods for visual development and rehabilitation in the treatment of congenital unilateral cataracts. The first paper was the result of a collaboration between Creig Hoyt and Elwin Marg in which eight children had dense unilateral congenital cataracts removed at 7 hours to 41 days of age and all achieved visual acuity of 20/80 or better (≤0.6 logMAR), including two children who astoundingly achieved 20/20 (0.0 logMAR) vision.4 This paper provided the impetus for a major shift in thinking. The critical period paradigm altered the perception of congenital cataract from an irremediable cause of visual impairment to a leading preventable cause of visual impairment in children.
The second paper came from Richard Held’s laboratory, using the newly developed forced-choice preferential looking technique to monitor visual acuity development in a few individual children following early surgery for dense congenital unilateral cataract.5 Despite an initially large visual acuity deficit, we could see for the first time the recovery of visual acuity with occlusion of the fellow
eye, its setbacks during periods of noncompliance, and continuation of recovery once occlusion therapy was restarted.
eye, its setbacks during periods of noncompliance, and continuation of recovery once occlusion therapy was restarted.
The dramatic change in clinical practice that quickly followed the publication of the seminal papers is illustrated in Figure 6.1. Prior to 1980, the median visual acuity outcome category following surgery for congenital unilateral cataracts was >20/1,200-light perception (>1.8 logMAR)3,6,7,8,9,10,11 and, for congenital bilateral cataracts, was >20/200 to 20/400 (1.0-1.3 logMAR).9,11 With the new emphasis on surgery during the first weeks of life to minimize the effects of visual deprivation on the developing visual system and careful monitoring of occlusion therapy, the median outcome category changed dramatically to 20/15 to 20/70 (−0.1 to 0.55 logMAR) for both unilateral and bilateral congenital cataracts.12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40
MODELS OF THE CRITICAL PERIOD FOR VISUAL DEVELOPMENT: VISUAL DEPRIVATION
Numerous studies since 1981 have demonstrated that earlier treatment of dense congenital cataracts is associated with better visual acuity outcomes. More recent studies have explored the nature of the relationship between the timing of treatment and the long-term visual outcome.12,14 Three alternative models of the critical period have been evaluated:
Linear: The earlier the surgery, the better the long-term visual acuity outcome.
Bilinear/Early Window: There exists an early window of time during which the optimum long-term visual acuity outcome can be obtained; beyond this window, visual acuity outcome declines linearly with further delay in treatment.
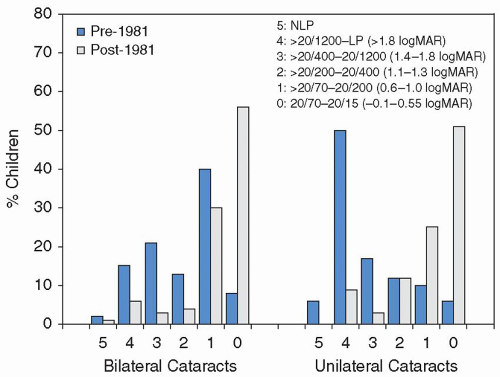
Figure 6.1. Visual acuity (logMAR) outcomes following surgery for dense congenital unilateral or bilateral cataracts from manuscripts published pre- and post-1981. Only children with age of onset of dense cataracts documented during the 1st week of life are included. Visual acuity categories correspond to the current World Health Organization International Statistical Classification of Diseases for Visual Impairment. NLP, no light perception; LP, light perception.
Bilinear/Plateau: Delay in treatment degrades long-term visual acuity outcome only during the first weeks or months of life, after which the outcome changes little with further delay.
Using a likelihood ratio test to determine which model best fit the data from children treated for dense congenital unilateral and bilateral cataracts, the slope (rate of change in outcome with delay in treatment) and critical ages were determined.12,14 The best-fit model for the critical period for visual deprivation due to dense congenital unilateral cataracts is shown in Figure 6.2. The Bilinear/Early Window model provides the best fit. During the first 6 weeks of life, there is little effect of age at surgery and long-term visual acuity outcome with a mean visual acuity outcome of 0.3 logMAR (20/40). After the critical age of 6 weeks, there is a steep decline in visual acuity outcome with further delay in treatment; each doubling in age at surgery (e.g., surgery at 10 weeks versus surgery at 20 weeks) is accompanied by a 0.3 logMAR drop in visual acuity (e.g., 20/80 versus 20/160).
The best-fit model for visual deprivation due to dense congenital bilateral cataracts is shown in Figure 6.3. The Bilinear/Plateau model provides the best fit. During the first 14 weeks of life, mean visual acuity decreased by one line with each 3 weeks’ delay in surgery, from
0.2 logMAR (20/30) at 1 week to 0.6 logMAR (20/80) at 14 weeks. After the age of 14 weeks, there is little change in visual acuity outcome with further delay in treatment, at least up to 40 weeks; mean visual acuity outcome for surgery delayed until 14 to 40 weeks is 0.6 logMAR (20/80).
0.2 logMAR (20/30) at 1 week to 0.6 logMAR (20/80) at 14 weeks. After the age of 14 weeks, there is little change in visual acuity outcome with further delay in treatment, at least up to 40 weeks; mean visual acuity outcome for surgery delayed until 14 to 40 weeks is 0.6 logMAR (20/80).
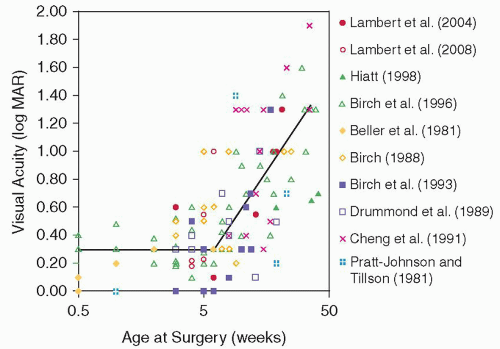 Figure 6.2. Best-fit model of the critical period for development with visual deprivation due to congenital unilateral cataract based on the data from Birch and Stager.14 The bilinear model exhibits a “latent period” that lasts up to 6 weeks of age during which the optimum long-term visual acuity outcome can be obtained; beyond 6 weeks, visual acuity outcome declines linearly with further delay in surgery. Data from other studies that evaluated the effect of age at surgery on long-term visual outcome have been added to the figure.4,13,16,17,18,24,28,30,36 Only children with age of onset of dense cataracts documented during the first week of life are included. Lambert et al. (2004)28; Lambert et al. (2008)30; Hiatt (1998)24; Birch et al. (1996)14; Beller et al. (1981)4; Birch (1988)13; Birch et al. (1993)16; Drummond et al. (1989)18; Cheng et al. (1991)17; Pratt-Johnson and Tillson (1981).36 |
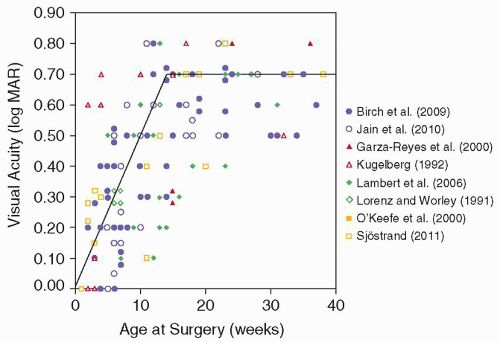 Figure 6.3. Best-fit model of the critical period for development with visual deprivation due to congenital bilateral cataract based on the data from Birch et al.12 Delay in treatment degrades long-term visual acuity outcome only during the first 14 weeks, decreasing by one line with each 3 weeks’ delay in surgery; after the critical age of 14 weeks, there is little change in visual acuity outcome with further delay in treatment up to at least 40 weeks. Data from other studies that evaluated the effect of age at surgery on long-term visual outcome have been added to the figure.11,20,27,29,34,35,39 Only children with age of onset of dense cataracts documented during the first week of life are included. Birch et al. (2009)12; Jain et al. (2010)29; Garza-Reyes et al. (2000)20; Kugelberg (1992)27; Lambert et al. (2006)29; Lorenz and Wörle (1991)33; O’Keefe et al. (2000)35; Sjöstrand et al. (2011).39 |
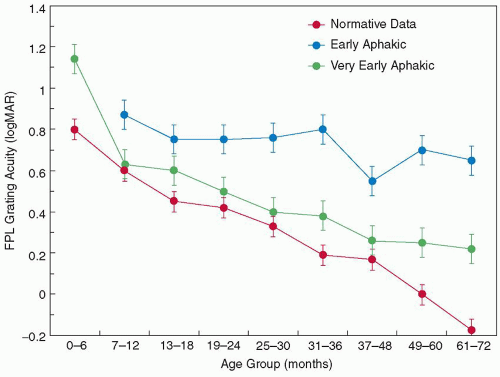 Figure 6.4. Grating acuity development during the first 6 years of life assessed by forced-choice preferential looking for children who had surgery for dense congenital unilateral cataracts at 1 to 6 weeks (very early) or 2 to 8 months (early). Also shown are normative data.48 (From Birch EE, Hale LA. Criteria for monocular acuity deficit in infancy and early childhood. Invest Ophthalmol Vis Sci 1988;29:636-643.) |
CRITICAL PERIOD FOR REHABILITATION
Following the influential studies by Held et al.,5,41,42 there were a large number of studies using the forced-choice preferential looking or visual evoked potential technique that showed that these visual acuity assessments were useful in guiding occlusion therapy, providing regular feedback on the progress of visual rehabilitation after each change in treatment protocol and/or a proxy measure for compliance with the prescribed occlusion therapy regimen.15,16,34,43,44,45,46,47 The ability to quantify visual acuity during the first years of life gave us a new means of understanding the critical period. The effect of age at surgery on long-term visual acuity outcome described in the section above helped us to define the critical period from the perspective of sensitivity to abnormal visual experience. On the other hand, evaluation of the development of visual acuity during infancy and early childhood allowed us to examine the critical period from the perspective of response to attempts to reverse the effects of visual deprivation through optical correction and occlusion therapy. In the example shown in Figure 6.4, visual acuity development of children with dense congenital unilateral cataracts who had “very early surgery” (by 6 weeks of age) was compared with the maturation of children who had surgery at 2 to 8 months.16




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
