Purpose
To evaluate the course and outcome of patients with accidental ocular alkali burns.
Design
Prospective, interventional case series.
Methods
Study of a cohort of 16 patients (31 eyes) who sustained concomitant accidental sodium hydroxide ocular burns and received appropriate treatment at a tertiary care eye hospital in India. The patients were followed up for 1 year, and parameters including best-corrected visual acuity, epithelial defect area, conjunctival and limbal involvement, and injury-related complications were evaluated.
Results
Severe sodium hydroxide exposure of a mean duration of 12 ± 2.5 minutes and delay in specialist eye care caused moderate to severe injury (grade II, 19% [n = 6]; grade III, 19% [n = 6]; grade IV, 10% [n = 3]; and grade VI, 52% [n = 16]). Median best-corrected visual acuity at presentation was 1.0 logarithm of the minimal angle of resolution (logMAR) units (range, 0.3 to 1.9 logMAR units), and at 1 year, it was 1.0 logMAR units (range, 0 to 1.9 logMAR units; P = .121). The median initial epithelial defect was 100 mm 2 (range, 18 to 121 mm 2 ), which healed in all eyes by 3.5 months. Initial median limbal involvement was 12 clock hours (range, 3 to 12 clock hours), resulting in a residual limbal stem cell deficiency of 6 clock hours (range, 0 to 12 clock hours) at 1 year. Most common complications were glaucoma and cataract. Corneal ulcers developed in 2 eyes, and keratolimbal graft was performed in 1 patient. Grade VI injuries had significantly worse outcome than the lower-grade injuries.
Conclusions
The course and outcome of ocular alkali burns depends on effective first aid (including a thorough eyewash), age, initial grade of injury, response to treatment, prevention of secondary infection, and control of glaucoma. Despite appropriate treatment, these eyes responded poorly and carried a guarded visual prognosis.
Chemical injuries are ophthalmic emergencies that have the potential to cause significant morbidity and loss of vision. Injuries with alkaline agents are slightly more common and produce more severe burns than acids. The exposure is predominantly industrial or occupational and is more common among young males.
Herein we describe a unique cohort of 16 patients who sustained simultaneous ocular and skin burns with a highly alkaline industrial grade sodium hydroxide (NaOH) solution after a traffic accident in rural India. We studied factors determining the severity of injury, response to treatment, and final outcome over a follow-up period of 12 months.
Methods
Sixteen patients were enrolled from the eye casualty service of our hospital, where they sought treatment for ocular and skin burns of varying severity. The patients had previously received care at a local hospital near the accident site, where they received an eyewash with normal saline and were prescribed preservative-free lubricant drops and topical antibiotics (chloramphenicol 0.5% 4 times daily). At our center, the tear film showed an alkaline pH. Repeat eyewash of the ocular surface extending into the conjunctival fornices (after double eversion of the lids) was performed with normal saline until a neutral pH of 7.0 was achieved. The eyewash samples and conjunctival swabs were collected for chemical analysis.
The accident victims were treated as in-patients using a standard treatment protocol. The protocol included topical moxifloxacin hydrochloride 0.5% 4 times daily (Vigamox; Alcon, Inc, Fort Worth, Texas, USA), topical prednisolone acetate 1% 4 times daily (Predforte; Allergan, Irvine, California, USA), preservative-free lubricant drops on an hourly basis (hydroxypropyl methylcellulose 2%; Ocular Pharmacy, Dr Rajendra Prasad Centre for Ophthalmic Sciences, Delhi, India), topical sodium citrate 10% every 4 hours (Ocular Pharmacy, Dr Rajendra Prasad Center for Ophthalmic Sciences), and topical sodium ascorbate 10% every 4 hours (Ocular Pharmacy, Dr Rajendra Prasad Centre for Ophthalmic Sciences). Oral vitamin C, 1 g daily, was given for 1 month to all patients (T. Limcee; Sarabhai Piramal Pharma, Vadodara, India), and 250 mg oral acetazolamide 4 times daily (T. Diamox; Wyeth Limited, Mumbai, India) was used to lower the intraocular pressure, as needed (topical antiglaucoma medications were avoided because of the risk of epithelial toxicity). Oral ciprofloxacin 500 mg twice daily was given for 7 to 10 days (T. Ciprobid; Cadila Healthcare, Gujarat, India) in 8 patients with extensive burns. Skin burns were treated in consultation with the surgical burn specialist using silver sulfadiazine 1% w/w, chlorhexidine gluconate 0.2% w/w, and regular paraffin gauze dressings. Oral ulcers and oral, aural, and nasal burns were managed in consultation with the dental and otorhinolaryngology experts.
The treatment was adjusted according to individual response. The prominent modifications included tapering topical steroids and then discontinuing in all cases within 2 weeks, adding fortified topical antibiotics in cases suspicious for infectious keratitis, increasing the frequency of topical lubricants or addition of gel preparations in eyes with eyelid abnormalities, adding oral doxycycline 100 mg twice daily in 4 patients with progressive corneal melting, removing trichiatic lashes, as needed, and making any necessary changes after surgical interventions.
The injury was classified according to the ocular chemical burns classification created by Dua and associates. The classification scheme involves grading ocular surface burns based on limbal and conjunctival involvement and includes an analog scale. Accordingly, the ocular parameters evaluated at the primary visit included best-corrected visual acuity (BCVA), ocular congestion, conjunctival chemosis, size of epithelial defect, degree of limbal involvement (in clock hours), degree of conjunctival involvement (as a percentage), anterior chamber reaction, intraocular pressure, and evidence of any secondary bacterial infection.
The patients were closely followed up for a period of 1 year. At months 3, 6, 9, and 12, the above parameters were recorded, along with documentation of any complications, such as limbal stem cell deficiency, symblepharon formation, pseudopterygia, lid abnormalities, glaucoma, or cataract. Therapeutic keratoplasty, amniotic membrane transplantation, keratolimbal graft, and cultured limbal stem cell transplantation were undertaken, if required.
The data were entered and analyzed using SPSS software version 11.5 (SPSS, Inc, Chicago, Illinois, USA) and Stata software version 8.0 (StataCorp LP, College Station, Texas, USA) following the appropriate protocol. The Friedman and Wilcoxon rank-sum (Mann–Whitney) tests were applied to assess the BCVA, epithelial defect area, and limbal involvement. Patients with limbal involvement were categorized into 2 groups: 6 clock hours or fewer and more than 6 clock hours. The groups were analyzed using the Wilcoxon signed-rank test.
Results
The patients were all males with a mean age of 28 ± 10.28 years (range, 15 to 55 years). The median grade of injury was grade III (range, grades II through VI) in patients younger than 25 years (n = 10) and grade VI (range, grades III through VI) in patients older than 25 years (n = 6; P = .14). The mean duration of exposure to the offending agent was 12 ± 2.54 minutes, and the time from exposure to initial treatment at the first hospital was 2 hours. The mean time to presentation at our center was 1.17 days. The patients had varying degrees of skin and mucosal burns, but systemically were stable. One patient, who was older than 45 years of age, had diabetes mellitus and another patient had hypertension. Both of these patients had good disease control on oral medications.
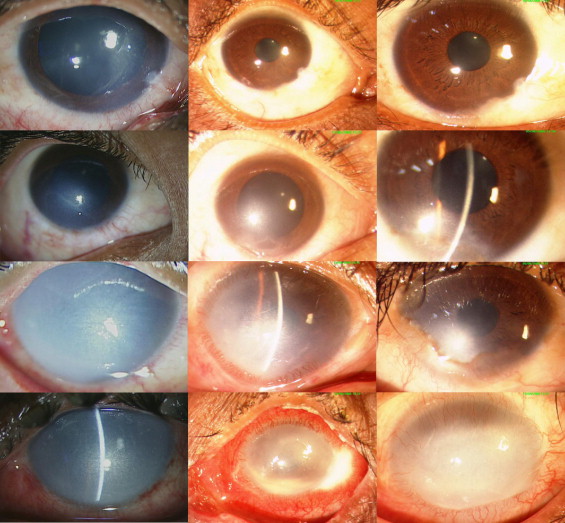
The patients had different grades according to the Dua classification. Of the patients, 6 (19%) had grade II injury, 6 (19%) had grade III injury, 3 (10%) had grade IV injury, and 16 (52%) had grade VI injury ( Figure 1 ). The median BCVA on day 1 was 1.0 logarithm of the minimal angle of resolution (logMAR) units (range, 0.3 to 1.9 logMAR units). Similarly, the BCVA at the end of 1 year was 1.0 logMAR units (range, 0 to 1.9 logMAR units; P = .121; Table 1 ). On subgroup analysis, the BCVA for grade VI injuries was significantly worse than that for lower-grade injuries, whereas comparison of the median BCVA of grade II and III injuries, grade II and IV injuries, and grade III and IV injuries revealed no significant differences ( Table 2 ).
| Serial Number | Age (years) | Grade (Dua Classification) | Best-Corrected Visual Acuity (logMAR Score) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| At Presentation | 2-Week Follow-up | 1-Month Follow-up | 3-Month Follow-up | 6-Month Follow-up | 9-Month Follow-up | 1-Year Follow-up | |||
| 1 | 25 | VI | 1.08 | 0.6 | 0.6 | 1.3 | 1.9 | 1.9 | 1.9 |
| 2 | 25 | VI | 1.18 | 1.9 | 1.9 | 1.9 | 1.9 | 1.9 | 1.9 |
| 3 | 20 | VI | 1.9 | 1.78 | 1.78 | 1.9 | 1.9 | 1.9 | 1.9 |
| 4 | 20 | VI | 1.9 | 1.78 | 1.78 | 1.9 | 1.9 | 1.9 | 1.9 |
| 5 | 32 | III | 0.48 | 0 | 0 | 0 | 0 | 0 | 0 |
| 6 | 32 | IV | 0.6 | 0.48 | 0.48 | 0.48 | 0.48 | 0.48 | 0.48 |
| 7 | 45 | III | 1.48 | 1.9 | 1.9 | 1.9 | 1.9 | 1.9 | 1.9 |
| 8 | 45 | IV | 1.3 | 1.9 | 1.9 | 1.9 | 1.9 | 1.9 | 1.9 |
| 9 | 15 | III | 0.6 | 0.3 | 0.16 | 0.16 | 0 | 0 | 0 |
| 10 | 15 | VI | 1.9 | 1.48 | 1.48 | 1.78 | 1.08 | 1 | 0.6 |
| 11 | 20 | II | 1 | 0.16 | 0.16 | 0.3 | 0 | 0 | 0 |
| 12 | 20 | VI | 1.9 | 1.48 | 1.48 | 1.3 | 1.18 | 1.18 | 1 |
| 13 | 25 | II | 0.6 | 0.16 | 0.16 | 0 | 0 | 0 | 0 |
| 14 | 25 | II | 0.6 | 0.16 | 0.16 | 0 | 0 | 0 | 0 |
| 15 | 28 | VI | 1 | 0.3 | 0.3 | 1.9 | 1.18 | 0.6 | 0.48 |
| 16 | 28 | VI | 1 | 0.48 | 0.48 | 1.9 | 1.9 | 1.3 | 1.9 |
| 17 | 55 | VI | 1.9 | 1.78 | 1.78 | 1.9 | 1.9 | 1.9 | 1.9 |
| 18 | 55 | VI | 1.78 | 1.48 | 1.48 | 1.9 | 1.9 | 1.9 | 1.9 |
| 19 | 18 | VI | 1.9 | 1.3 | 1.18 | 0.48 | 0.6 | 0.6 | 0.3 |
| 20 | 22 | II | 0.48 | 0.3 | 0.3 | 0.16 | 0.16 | 0.16 | 0.16 |
| 21 | 22 | II | 0.48 | 0.16 | 0.16 | 0.16 | 0.16 | 0.16 | 0.16 |
| 22 | 22 | III | 0.3 | 0.16 | 0.16 | 0 | 0 | 0 | 0 |
| 23 | 22 | III | 0.3 | 0.16 | 0.16 | 0.16 | 0 | 0 | 0 |
| 24 | 35 | VI | 1.48 | 1.3 | 1.3 | 1.9 | 1.9 | 1.9 | 1.9 |
| 25 | 35 | VI | 1.48 | 1.48 | 1.48 | 1.9 | 1.9 | 1.9 | 1.9 |
| 26 | 35 | IV | 0.6 | 0.6 | 1.9 | 1.18 | 1.9 | 1.9 | 1.9 |
| 27 | 35 | VI | 1.8 | 1.78 | 1.9 | 1.48 | 1.9 | 1.9 | 1.9 |
| 28 | 25 | VI | 1.3 | 1.3 | 1.9 | 1.9 | 1.9 | 1.9 | 1.9 |
| 29 | 25 | VI | 1 | 1.3 | 1.9 | 1.9 | 1.9 | 1.9 | 1.9 |
| 30 | 25 | II | 1 | 0.3 | 0.3 | 0.3 | 0.3 | 0.3 | 0.16 |
| 31 | 25 | III | 0.78 | 0.16 | 0.16 | 0 | 0 | 0 | 0 |
| Grade (Dua Classification) | Median (Range) Best-Corrected Visual Acuity (logMAR units) | Significance of Change between Presentation and Final Visit ( P Value) | |
|---|---|---|---|
| At Presentation | At 1 Year | ||
| II | 0.6 (0.48 to 1) | 0.08 (0 to 0.16) | .03 |
| III | 0.54 (0.3 to 1.48) | 0.0 (0 to 1.9) | .11 |
| IV | 0.6 (0.6 to 1.3) | 1.9 (0.48 to 1.9) | .29 |
| VI | 1.63 (1 to 1.9) | 1.9 (0.3 to 1.9) | .50 |
The corneal epithelium showed signs of healing with medical management ( Table 3 ). Likewise, the limbal involvement ( Table 4 ) and conjunctival involvement ( Table 5 ) also showed improvement. The median epithelial defect area at day 1 was 100 mm 2 (range, 18 to 121 mm 2 ), which decreased to a median of 0 mm 2 (range, 0 to 28 mm 2 ) by 3 months. Seven patients with grade VI injury still had epithelial defects ranging from 4 to 28 mm 2 at the 3-month follow-up visit. However, by week 14, all epithelial defects had healed. The epithelial defect area varied substantially according to the severity of injury ( Tables 6 and 7 ). Patients with grade IV and VI injuries had significantly worse epithelial defects than patients with other grades of injury ( Table 7 ). There was no significant difference between the grade II and III injuries ( P = .14, Mann–Whitney U test).
| Serial Number | Age (years) | Grade (Dua Classification) | Epithelial Defect Area (mm 2 ) | ||||
|---|---|---|---|---|---|---|---|
| At Presentation | 2-Week Follow-up | 1-Month Follow-up | 3-Month Follow-up | 6-Month Follow-up | |||
| 1 | 25 | VI | 100 | 31.5 | 5.2 | 0 | 0 |
| 2 | 25 | VI | 100 | 44 | 10.8 | 0 | 0 |
| 3 | 20 | VI | 100 | 23.76 | 16.4 | 0 | 0 |
| 4 | 20 | VI | 100 | 3.51 | 0.8 | 0 | 0 |
| 5 | 32 | III | 56 | 0 | 0 | 0 | 0 |
| 6 | 32 | IV | 120 | 1.3 | 0 | 4.5 | 0 |
| 7 | 45 | III | 121 | 14 | 10.5 | 24 | 0 |
| 8 | 45 | IV | 121 | 17.5 | 9 | 9 | 0 |
| 9 | 15 | III | 40 | 7 | 2 | 0 | 0 |
| 10 | 15 | VI | 121 | 48 | 44.1 | 0 | 0 |
| 11 | 20 | II | 64 | 0 | 0 | 0 | 0 |
| 12 | 20 | VI | 121 | 56 | 23.94 | 0 | 0 |
| 13 | 25 | II | 17.5 | 0 | 0 | 0 | 0 |
| 14 | 25 | II | 39.2 | 0 | 0 | 0 | 0 |
| 15 | 28 | VI | 121 | 30 | 25 | 6 | 0 |
| 16 | 28 | VI | 121 | 56 | 52.5 | 8 | 0 |
| 17 | 55 | VI | 121 | 80 | 20.79 | 0 | 0 |
| 18 | 55 | VI | 121 | 64 | 59.25 | 28 | 0 |
| 19 | 18 | VI | 64 | 16 | 12 | 0 | 0 |
| 20 | 22 | II | 48 | 0 | 0 | 0 | 0 |
| 21 | 22 | II | 36 | 0 | 0 | 0 | 0 |
| 22 | 22 | III | 68 | 0 | 0 | 0 | 0 |
| 23 | 22 | III | 22.5 | 0 | 0 | 0 | 0 |
| 24 | 35 | VI | 121 | 84 | 81.81 | 4 | 0 |
| 25 | 35 | VI | 121 | 91.8 | 81.34 | 0 | 0 |
| 26 | 35 | IV | 121 | 22.5 | 10.5 | 0 | 0 |
| 27 | 35 | VI | 121 | 38 | 28 | 0 | 0 |
| 28 | 25 | VI | 121 | 98 | 100 | 0 | 0 |
| 29 | 25 | VI | 121 | 95.06 | 60.8 | 0 | 0 |
| 30 | 25 | II | 30.25 | 4.2 | 0 | 0 | 0 |
| 31 | 25 | III | 48.75 | 0 | 0 | 0 | 0 |
| Serial Number | Age (years) | Grade (Dua Classification) | Limbal Involvement (in Clock Hours) | Limbal Stem Cell Deficiency | |||||
|---|---|---|---|---|---|---|---|---|---|
| At Presentation | 2-Week Follow-up | 1-Month Follow-up | 3-Month Follow-up | 6-Month Follow-up | 9-Month Follow-up | 1-Year Follow-up | |||
| 1 | 25 | VI | 12 | 6 | 6 | 9 | 9 | 9 | 9 |
| 2 | 25 | VI | 12 | 7 | 7 | 12 | 12 | 12 | 12 |
| 3 | 20 | VI | 12 | 6 | 6 | 7 | 12 | 12 | 12 |
| 4 | 20 | VI | 12 | 3 | 3 | 8 | 9 | 9 | 9 |
| 5 | 32 | III | 4 | 2 | 0 | 0 | 0 | 0 | 0 |
| 6 | 32 | IV | 9 | 6 | 0 | 0 | 0 | 0 | 0 |
| 7 | 45 | III | 4 | 3 | 3 | 5 | 5 | 5 | 5 |
| 8 | 45 | IV | 8 | 3 | 3 | 5 | 6 | 6 | 6 |
| 9 | 15 | III | 6 | 2 | 1 | 0 | 0 | 0 | 1 |
| 10 | 15 | VI | 12 | 12 | 9 | 9 | 9 | 9 | 9 |
| 11 | 20 | II | 3 | 0 | 0 | 0 | 0 | 0 | 0 |
| 12 | 20 | VI | 12 | 9 | 9 | 9 | 9 | 9 | 8 |
| 13 | 25 | II | 3 | 0 | 0 | 0 | 0 | 0 | 0 |
| 14 | 25 | II | 3 | 0 | 0 | 0 | 0 | 0 | 0 |
| 15 | 28 | VI | 12 | 6 | 6 | 6 | 6 | 6 | 7 |
| 16 | 28 | VI | 12 | 7 | 8 | 7 | 8 | 8 | 9 |
| 17 | 55 | VI | 12 | 9 | 9 | 12 | 12 | 12 | 12 |
| 18 | 55 | VI | 12 | 12 | 12 | 12 | 12 | 12 | 12 |
| 19 | 18 | VI | 12 | 6 | 6 | 5 | 5 | 6 | 7 |
| 20 | 22 | II | 3 | 1 | 0 | 0 | 0 | 0 | 0 |
| 21 | 22 | II | 3 | 0 | 0 | 0 | 0 | 0 | 0 |
| 22 | 22 | III | 6 | 1 | 1 | 1 | 1 | 1 | 1 |
| 23 | 22 | III | 6 | 0 | 0 | 0 | 0 | 1 | 1 |
| 24 | 35 | VI | 12 | 9 | 9 | 9 | 4 | 12 | 12 |
| 25 | 35 | VI | 12 | 7 | 7 | 7 | 6 | 6 | 4 |
| 26 | 35 | IV | 9 | 9 | 9 | 9 | 9 | 9 | 7 |
| 27 | 35 | VI | 12 | 7 | 7 | 7 | 7 | 7 | 12 |
| 28 | 25 | VI | 12 | 9 | 12 | 12 | 12 | 12 | 12 |
| 29 | 25 | VI | 12 | 9 | 12 | 12 | 12 | 12 | 12 |
| 30 | 25 | II | 4 | 1 | 1 | 1 | 1 | 3 | 3 |
| 31 | 25 | III | 6 | 3 | 2 | 0 | 0 | 0 | 0 |
| Serial Number | Age (years) | Grade (Dua Classification) | Conjunctival Involvement (%) | |
|---|---|---|---|---|
| At Presentation | Final Outcome (1 Year) | |||
| 1 | 25 | VI | 90 | Symblepharon |
| 2 | 25 | VI | 95 | Symblepharon |
| 3 | 20 | VI | 95 | Pseudopterygium |
| 4 | 20 | VI | 95 | Pyogenic granuloma |
| 5 | 32 | III | 50 | Scarring |
| 6 | 32 | IV | 60 | Scarring |
| 7 | 45 | III | 40 | Normal |
| 8 | 45 | IV | 70 | Scarring |
| 9 | 15 | III | 40 | Normal |
| 10 | 15 | VI | 90 | Scarring |
| 11 | 20 | II | 20 | Normal |
| 12 | 20 | VI | 95 | Scarring |
| 13 | 25 | II | 20 | Normal |
| 14 | 25 | II | 20 | Normal |
| 15 | 28 | VI | 90 | Scarring |
| 16 | 28 | VI | 95 | Scarring |
| 17 | 55 | VI | 95 | Symblepharon |
| 18 | 55 | VI | 95 | Scarring |
| 19 | 18 | VI | 95 | Pseudopterygium |
| 20 | 22 | II | 20 | Pseudopterygium |
| 21 | 22 | II | 20 | Normal |
| 22 | 22 | III | 40 | Normal |
| 23 | 22 | III | 40 | Normal |
| 24 | 35 | VI | 95 | Scarring |
| 25 | 35 | VI | 95 | Pseudopterygium |
| 26 | 35 | IV | 70 | Scarring |
| 27 | 35 | VI | 90 | Pseudopterygium |
| 28 | 25 | VI | 95 | Pyogenic granuloma |
| 29 | 25 | VI | 90 | Scarring |
| 30 | 25 | II | 20 | Normal |
| 31 | 25 | III | 50 | Normal |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


