Chapter 5
COUNSELING THE PATIENT AND THE FAMILY

Although any injury is stressful, eye trauma, among non life-threatening injuries, is especially so.1 Blindness has regularly been found the most feared of all disabilities in Gallup polls, and any threat to vision is emotionally wrenching.
Of all causes of sight loss, injury is the most sudden and dramatic because it is instantaneous (Fig. 5–1). Humans rely heavily on vision to avoid bodily trauma, and therefore it is particularly shocking if the eye itself is injured. This makes counseling of eye trauma patients and their families uniquely important. Adequate and skilled counseling is especially critical in cases of serious injuries that require surgical intervention.
COUNSELING GOALS
Counseling must be
• comforting;
• informative;
• truthful;
• accurate;
• compassionate;
• patient;
• dynamic; and
• continuing at least until the conclusion of treatment.
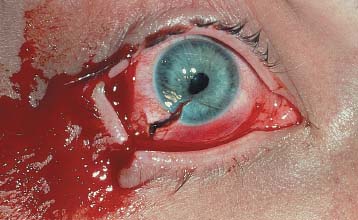
FIGURE 5–1 Corneoscleral laceration at presentation.
Comforting the Patient
Because the first contact occurs in the emergency setting, the physician-patient relationship does not enjoy the usual benefits of an orderly, planned encounter. In view of the stress associated with an unexpected injury, it is especially important for the ophthalmologist to communicate calmness and seriousness of purpose. Careless words or gestures may quickly handicap this delicate and growing relationship.
The counselor is preferably the treating physician, instilling confidence and hope to the extent that hope is justified by increasingly detailed knowledge of the prognosis.
PEARL… Although it is true that the final visual outcome often remains in doubt for weeks or even months, the physician should encourage the patient not to give up hope unless the eye has permanently (see Chapter 8) lost all potential for vision.
Modern techniques of globe reconstruction enable visual recovery in eyes that would have been considered lost even as recently as a few years ago. The external appearance of the injury’s severity and the loss of light perception must not by themselves guide management (see Fig. 5–2 and Chapter 8). It is the vitreous surgeon’s responsibility to distinguish reasonable hope from futility in the search for vision.
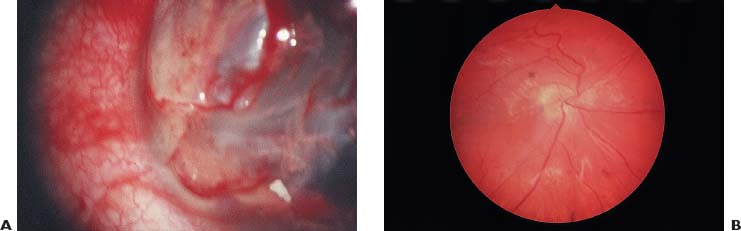
FIGURE 5–2 (A) Preoperative photograph of retinal prolapse through a severe corneoscleral laceration, an injury unsalvageable only years ago. (B) Reattached retina under silicone oil.
SPECIAL CONSIDERATION
Hope for visual improvement may increase or decrease throughout the course of therapy; counseling therefore has to continue through the entirety of the patient—physician relationship. The patient’s occasional inappropriately optimistic or pessimistic attitude must be recognized by the physician, who, even if it is extremely time consuming, must respond to it.
The physician who is not effectively communicating with the patient and familya may engender false hope or unnecessary anxiety. Without a reasonable measure of compassion and empathy, the physician will fail to observe these reactions, which may lead to:
• sudden depression when a poor prognosis is belatedly understood; or
• unnecessary suffering when the outcome is clearly better than the patient has come to expect.
No matter what the treatment outcome, it will be more acceptable to, and appreciated by, the patient at the conclusion of the treatment if the physician has maintained effective communication throughout their encounters.
Informing the Patient
Providing comfort to the patient and family is inseparable from the goal of providing information to obtain the patient’s participation and informed consent because realistic decisions cannot be based on inaccurate information. Major recent milestones in the ophthalmologist’s ability to provide an injury-specific prognosis include the BETT,2 the classification of injuries,3 and the OTS (see Chapters 1, 2, and 3).
After the initial assessment, the counseling physician should keep the patient and family regularly apprised of the eye’s response to the applied treatment and of additional treatment options. The latter is especially important for gaining both acceptance of the recurrent surgical intervention commonly needed after injury and patience to allow full recovery without avoidable frustration or depression.
The constant flow of information from the ophthalmologist is also important to facilitate the patient’s cooperation (e.g., positioning after the application of certain vitreous substitutes; see the Appendix). The patient must plan life adjustments and will deeply appreciate the accurate and timely information that enables such planning.
As required, vocational and psychological counseling must also be offered, as well as low-vision rehabilitation (see Chapter 6).
PEARL… The emotions associated with eye injury and its treatment run the gamut from depression to exhilaration. Compassion, competence, and commitment on the part of the treating physician and support staff are appreciated by the patient.
No list of specific counseling issues can be totally comprehensive, given:
• the variability of eye injuries and the response of the eyes to treatment;
• the different patient-family personalities; and
• the physicians’ treatment philosophies.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


