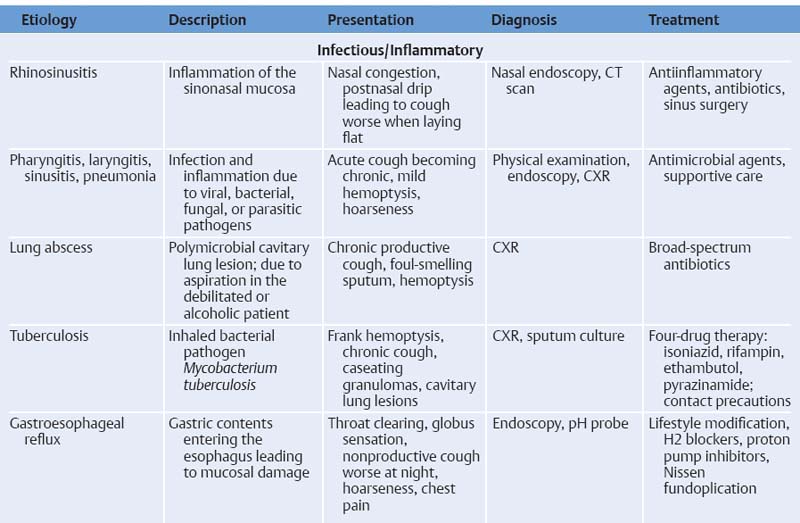
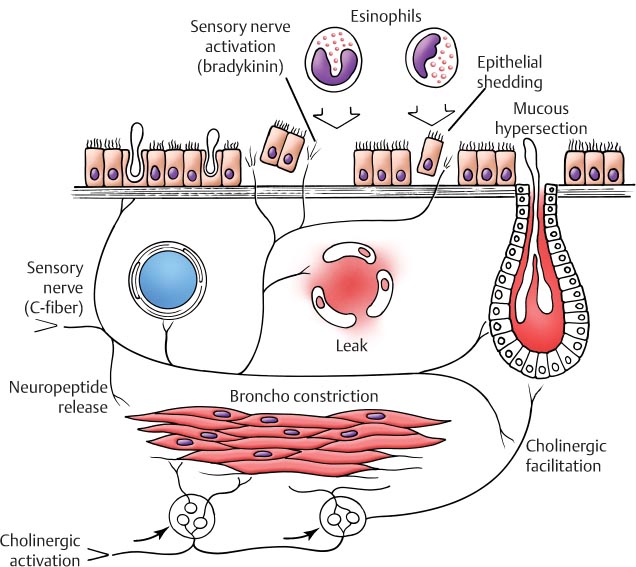
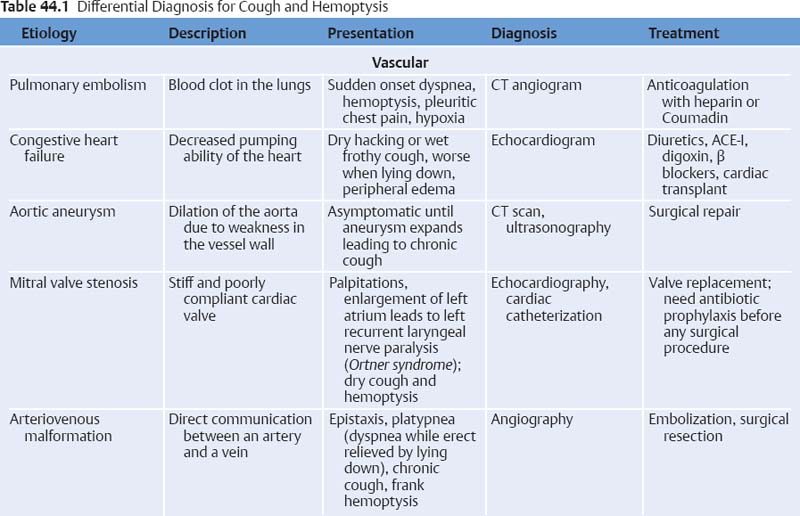
44 Cough or Hemoptysis Cough, derived from the Latin word tussis, is an expulsion of air from the lungs that is often accompanied by a characteristic sound. It is usually produced as a response to foreign matter irritating the lining of the respiratory tract, including the larynx, trachea, and distal airways. Furthermore, cough can be divided into acute, lasting less than 3 weeks, subacute, lasting 3 to 8 weeks, or chronic, lasting greater than 8 weeks. Additionally, hemoptysis is the expectoration of blood or blood-tinged sputum from any area within the airway passages, including the nose, mouth, laryngopharynx, trachea, bronchi, alveoli, and lung parenchyma. This word itself is a derivative from the Greek words haima, meaning blood, and ptyein, meaning to spit. The involuntary cough reflex is a primitive, protective action initiated by mechanical stimulation of both myelinated and unmyelinated sensory afferent nerve fibers from the larynx and lungs, chemoreceptors in the distal airway, and stretch receptors in the lungs (Fig. 44.1). Additional afferent fibers from the Arnold nerve transmit signals from the external auditory canal and tym-panic membrane. These afferent signals are then transmitted by the vagus nerve directly to the medulla. The efferent cascade is initiated with the inspiration of air followed by closure of the epiglottis. The vocal cords then adduct to entrap the air within the lungs. Next, the expiratory and accessory muscles simultaneously contract, resulting in increased intrathoracic pressure reaching upward of 300 mm Hg. The epiglottis and vocal cords then open widely, resulting in both a rapid release of air and production of a distinctive noise. This sudden gush of air can reach velocities as high as 75 to 100 miles per hour. The noncartilaginous portions of the bronchi and trachea collapse inward, thereby allowing the air passing through to carry with it the irritants present within the airway. The act of coughing can also be a voluntary event based on supramedullary central cortical stimulation, resulting in an alteration of the expiratory and accessory muscles’ activities. Voluntary control of the force of muscle contractility results in variation of cough intensity. This cough is not directly mediated by irritation of the respiratory tract, but rather as a conscious effort by the individual. Fig. 44.1 Pathophysiology of the cough reflex in response to neurogenic inflammation in asthma. Cough can be due to various etiologies, including self-limited benign illnesses to more significant and potentially fatal diseases. It can be dry or productive, the latter being associated with the expulsion of sputum, mucus, or exudate, suggestive of a possible underlying infection, a systemic disease, or even a malignancy. Hemoptysis can be a symptom of a much more severe and possibly life-threatening disease process that warrants immediate investigation. If the hemoptysis is of bronchogenic origin, it is often massive due to the pressures of the systemic circulation, whereas bleeding from the pulmonary circulation is less profuse. In adults, the differential diagnosis for both cough and hemoptysis is broad; however, the causes can be simplified into several general categories (Table 44.1).
 Pathophysiology
Pathophysiology
 Etiology
Etiology
 Pulmonary embolism (PE): Associated with a sudden onset of dyspnea, hemoptysis, pleuritic chest pain, and hypoxia. Hemoptysis can occur in the setting of a massive PE. Risk factors include immobility, recent surgery, obesity, malignancy, history of thromboembolism, and smoking. Clinical symptoms include tachycardia, tachypnea, hypoxia, rales or decreased breath sounds, and elevated jugular venous distension. It is second only to coronary artery disease as the most common cause of unexpected natural death in any age group.
Pulmonary embolism (PE): Associated with a sudden onset of dyspnea, hemoptysis, pleuritic chest pain, and hypoxia. Hemoptysis can occur in the setting of a massive PE. Risk factors include immobility, recent surgery, obesity, malignancy, history of thromboembolism, and smoking. Clinical symptoms include tachycardia, tachypnea, hypoxia, rales or decreased breath sounds, and elevated jugular venous distension. It is second only to coronary artery disease as the most common cause of unexpected natural death in any age group.
 Congestive heart failure (CHF): Can have either a dry hacking or a wet frothy cough that may worsen when lying down or on exertion. Impaired systolic function results in a sympathetically mediated retention of salt and water, thereby leading to systemic as well as pulmonary fluid overload. The most common risk factors for CHF include heart disease, hyper-tension, and diabetes.
Congestive heart failure (CHF): Can have either a dry hacking or a wet frothy cough that may worsen when lying down or on exertion. Impaired systolic function results in a sympathetically mediated retention of salt and water, thereby leading to systemic as well as pulmonary fluid overload. The most common risk factors for CHF include heart disease, hyper-tension, and diabetes.
 Aortic aneurysm: Patients often remain asymptomatic until the aneurysm begins to expand, at which time they may develop a chronic cough due to pressure on the respiratory tract or recurrent laryngeal nerve. This vascular pathology is associated with hypertension, autoimmune diseases, syphilis, and genetic defects in structural proteins (eg, Marfan syndrome).
Aortic aneurysm: Patients often remain asymptomatic until the aneurysm begins to expand, at which time they may develop a chronic cough due to pressure on the respiratory tract or recurrent laryngeal nerve. This vascular pathology is associated with hypertension, autoimmune diseases, syphilis, and genetic defects in structural proteins (eg, Marfan syndrome).
 Mitral valve stenosis: This can lead to left atrial enlargement, which can exert pressure on and possible paralysis of the left recurrent laryngeal nerve, resulting in a dry cough and hoarseness (Ortner syndrome). This disease process is most often seen in patients with a history of rheumatic fever, although congenital stenosis has also been reported.
Mitral valve stenosis: This can lead to left atrial enlargement, which can exert pressure on and possible paralysis of the left recurrent laryngeal nerve, resulting in a dry cough and hoarseness (Ortner syndrome). This disease process is most often seen in patients with a history of rheumatic fever, although congenital stenosis has also been reported.
 Arteriovenous malformation: Can afflict various systems; however, respiratory tract involvement may lead to frequent epistaxis, platypnea (difficulty in breathing while erect often relieved by lying down), chronic cough, and massive hemoptysis.
Arteriovenous malformation: Can afflict various systems; however, respiratory tract involvement may lead to frequent epistaxis, platypnea (difficulty in breathing while erect often relieved by lying down), chronic cough, and massive hemoptysis.
 Infectious/inflammatory etiology
Infectious/inflammatory etiology
 Acute or chronic rhinosinusitis: Results in postnasal drip, which is one of the leading causes for cough. This is exacerbated by lying flat. Bacterial infections will lead to a productive cough and discolored rhinorrhea.
Acute or chronic rhinosinusitis: Results in postnasal drip, which is one of the leading causes for cough. This is exacerbated by lying flat. Bacterial infections will lead to a productive cough and discolored rhinorrhea.
 Cardiovascular etiology
Cardiovascular etiologyStay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


