Certain anatomic variations of the lower lateral cartilages can predispose patients to nasal obstruction. One particular orientation is the cephalic malposition of the lower lateral cartilages which often results in both cosmetic and functional nasal effects. This article will discuss the pertinent surgical anatomy, diagnosis, the process to identify patients at risk with cephalic malposition of the lower lateral cartilages, pitfalls, and poor surgical changes that result in external nasal valve collapse. Appropriate diagnosis, prevention, and surgical maneuvers to address this will be discussed.
L.B. is a 35-year-old female who presented with nasal obstruction and a nasal deformity. She had a history of trauma to her nose when she was accidentally struck by a golf club at the age of 15. She had an attempted closed reduction of the nasal fracture at that time and now complains of persistent left- and right-side nasal obstruction. Additionally, she was concerned about the appearance of her nose and disliked the large size and fullness of the tip. A review of systems and her past medical history was unremarkable. Physical examination with attention to nasal analysis revealed a nose with an acute nasolabial angle that is overprojected. Analysis of the nasal septum revealed a C-shaped deformity to the left. The nasal tip appeared to have a boxy configuration with significantly medially rotated supra-alar creases. A hanging columella was identified. The external valves were deficient bilaterally with incomplete collapse on inspiration ( Fig. 1 ).

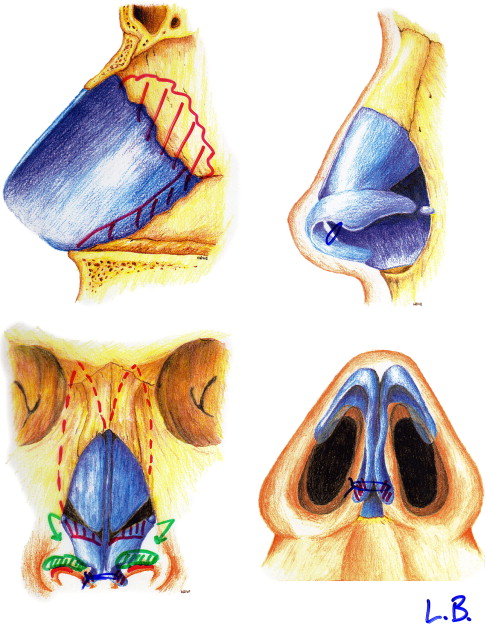
The patient underwent a rhinoplasty using an endonasal approach. A septoplasty was performed first to correct the C-shaped deformity. Cephalic malposition of the lower lateral cartilages, which was suspected preoperatively, was confirmed intraoperatively. A conservative cephalic trim was performed through an intracartilaginous incision with careful attention paid to identifying the true cephalic border of the alar cartilage. Cartilage harvested from the cephalic trim was weakened and placed as an alar rim graft bilaterally through a small pocket created along the mid ala. A tongue-in-groove suture was placed to reduce the hanging columella, and medial and lateral osteotomies were performed to correct the position of the nasal bones ( Fig. 2 ).
Postoperatively, the patient was pleased with her rhinoplasty results, particularly the correction of her tip deformity. Her nasal breathing was improved and there was no further evidence of external nasal valve collapse on inspiration ( Fig. 3 ).

Rhinoplasty is a surgical procedure that requires a meticulous nasal evaluation, while simultaneously challenging the surgeon’s judgment and technical execution. The time spent critically analyzing the patient’s nasal anatomy allows the surgeon to appreciate the individual contributions of the underlying bone, cartilage framework, and skin and soft tissue envelope to the nasal shape and form. This evaluation should include both careful inspection of the nasal topography and thorough palpation of the cartilage framework and skin. Surgeons who fail to recognize functional nasal abnormalities or inadvertently create breathing problems from a rhinoplasty are not maximizing their patients’ outcomes.
Cephalic malposition: common anatomic variation
Cephalic malposition of the paired lower lateral cartilages is a common anatomic variation of the underlying cartilage framework. Normally, the lateral crura follow the curvature of the alar margin before diverging at a 30 to 45° angle toward the lateral canthus at the mid ala. Sheen was one of the first to describe the cephalic malposition abnormality, in which the lateral crura diverge early and at a greater than 45° angle from the alar margin toward the ipsilateral medial canthus. This anatomic variation occurs commonly as illustrated in multiple reports by Constantian. In his study of 200 consecutive primary and secondary rhinoplasty patients, the majority of the patients had alar cartilage malposition. Sixty-eight percent of primary rhinoplasty patients and 87% of secondary rhinoplasty patients manifested this anatomic abnormality. In an earlier study, Constantian found that cephalic malposition of the alar cartilage occurred at lower rates with 18% of primary rhinoplasty patients and up to 42% of secondary rhinoplasty patients affected. While this may be a reflection of selection bias to a specific rhinoplasty practice, it is more important to realize that this anatomic abnormality was found to strongly predispose a patient to unfavorable rhinoplasty results. It is clear that the effect of cephalic malposition of the lower lateral cartilages on both the cosmetic nasal contour and functional nasal breathing is frequently underappreciated.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


