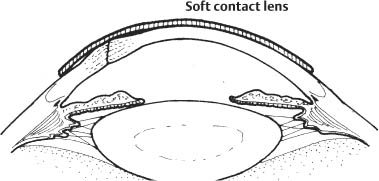
28 To obtain complete watertight closure of the globe with restoration of structural integrity. Overall goals for treating a patient with a possible corneal or scleral laceration include: 1. Recognize and address any life-threatening systemic conditions. 2. Obtain a detailed history. a. Specifically address the possibility of an intraocular foreign body. b. Determine if previous eye surgery took place (e.g., radial keratotomy or RK incisions and cataract wound predispose to rupture: LASIK scars predispose to flap dehisence). 3. Carefully evaluate the eye and adnexa. a. Eyelid irregularities may be a foreign body entrance site. b. Assess pupillary function and inspect pupil at slit lamp. c. Severe subconjunctival hemorrhage and shallow or unusually deep anterior chamber are strong indicators of ruptured globe. d. Document hyphema size, lens or iris injury, and optic nerve or retinal damage. Note: Avoid intraocular pressure measurements when there is a possibility of globe rupture. 4. Obtain imaging studies as necessary (plain film, computed tomographic scan). a. Magnetic resonance imaging should be avoided in any case where a metallic foreign body is possible. b. A- and B-scans should be avoided in cases of globe rupture until the globe is watertight. 1. Shield (metal or plastic) the affected eye at all times. 2. Reduce pain and nausea to prevent lid squeezing. 3. Confine patient to bed rest and fasting until time of surgery. 4. Administer prophylactic intravenous broad spectrum antibiotics. a. Cefazolin (1 g IV every 8 hours) and ciprofloxacin (400 mg IV 2 times per day) are a typical combination. b. Clindamycin is added when an intraocular foreign body is suspected (for Bacillus coverage). 5. Tetanus toxoid as needed. 1. A Seidel test should be conducted to rule out occult perforation. 2. Provocation with gentle finger pressure at the slit lamp may be done. If either (1) or (2) above are positive, broad spectrum antibiotic coverage should be initiated and patient should be followed closely. Figure 28.1 3. If minimal wound gape is present, the edges do not override, and the anterior chamber remains formed—usually in lacerations smaller than 3 mm—a bandage contact lens may be used (Fig. 28.1). 4. Alternatively, a pressure patch may be used. 5. A cycloplegic agent (e.g., homatropine 5%) and antibiotic drop (e.g., moxifloxacin 0.5% [Vigamox, Alcon Laboratories, Inc., Fort Worth, TX, US], gatifloxacin 0.3% [Zymar, Allergan, Inc., Irvine, CA, US]) 6 times per day should be used. 6. Bandage lens should be left on for 2–4 weeks, or when the stromal wound appears to be stabilized. 7. A plastic or metal shield should be placed over affected eye each evening and protective daytime eyewear should be worn until wound is sufficiently healed. 1. Cyanoacrylate glue may be useful in these situations (see Chapter 21). 2. For children and uncooperative patients, and those who may have difficulty keeping follow-up exams, definitive surgical closure is more appropriate. The surgeon should remember that the best way to ensure good tissue closure is with suture placement. Any wound with significant override or gape—whether partial or full thickness—should be repaired with sutures. Any case of traumatic conjunctival laceration should be suspected to be a ruptured globe. If any examination findings are suggestive of scleral laceration, the patient should be taken to the operating room for exploration. Exploration of the sclera with cotton-tipped applicator under topical anesthesia (e.g., proparacaine) may be useful. If the injury involves only the conjunctiva, treatment is as follows: 1. Conjunctival lacerations less than 1.0 cm, with minimal exposed Tenon capsule: a. Antibiotic ointment (e.g., erythromycin) or drops (e.g., moxifloxacin 0.5% [Vigamox, Alcon Laboratories, Inc.], gatifloxacin 0.3% [Zymar, Allergan, Inc.]) 4–6 times per day. b. Consider pressure patching for the first 24 hours. 2. For conjunctival lacerations larger than 1 cm, or irregular wounds with exposed Tenon capsule or muscle sheath: a. Carefully inspect tissue edges to excise Tenon capsule (blunt Westcott scissors). b. Perform interrupted suture closure with absorbable sutures (e.g., 8–0 Vicryl). i. Avoid burying edge of conjunctiva when closing wound. ii. Avoid suturing directly to the plica semilunaris or caruncle.
Corneoscleral Lacerations and Ruptured Globe Repair
Indications
 Partial-thickness wounds with significant override or gape
Partial-thickness wounds with significant override or gape
 Specific partial-thickness wounds that are at a higher risk of perforation (e.g., children)
Specific partial-thickness wounds that are at a higher risk of perforation (e.g., children)
 Full-thickness wounds larger than 3 mm that do not self-seal
Full-thickness wounds larger than 3 mm that do not self-seal
 Full-thickness wounds that do not close adequately with bandage lens or tissue glue placement
Full-thickness wounds that do not close adequately with bandage lens or tissue glue placement
 Wounds with loss of corneal tissue
Wounds with loss of corneal tissue
 All full-thickness wounds with iris incarceration
All full-thickness wounds with iris incarceration
 All full-thickness wounds with vitreous incarceration
All full-thickness wounds with vitreous incarceration
 All posterior scleral lacerations (and any suspected posterior lacerations based on exam)
All posterior scleral lacerations (and any suspected posterior lacerations based on exam)
Objectives
Primary Objective
Secondary Objectives
 Remove disrupted tissues (e.g., lens, vitreous).
Remove disrupted tissues (e.g., lens, vitreous).
 Remove intraocular foreign bodies.
Remove intraocular foreign bodies.
 Prevent infection.
Prevent infection.
 Prepare for future reconstruction and rehabilitation strategies.
Prepare for future reconstruction and rehabilitation strategies.
Preoperative Procedure
Supportive Treatment
Nonsurgical Management
Self-Sealing or Partial-Thickness Wounds
Puncture Wounds or Small Tissue-Loss Wounds
Conjunctival Laceration Repair
Instrumentation
 Lid speculum (e.g., Lieberman)
Lid speculum (e.g., Lieberman)
 Fine-toothed tissue forceps (e.g., 0.12 mm forceps)
Fine-toothed tissue forceps (e.g., 0.12 mm forceps)
 Westcott scissors
Westcott scissors
 Sutures (4–0 silk, 8–0 nylon, 10–0, and 11–0 nylon with spatulated needle, 8–0 Vicryl)
Sutures (4–0 silk, 8–0 nylon, 10–0, and 11–0 nylon with spatulated needle, 8–0 Vicryl)
 Needle holder
Needle holder
 Smooth forceps (e.g., Chandler or Bracken forceps)
Smooth forceps (e.g., Chandler or Bracken forceps)
 Viscoelastic material (e.g., Amvisc, Viscoat)
Viscoelastic material (e.g., Amvisc, Viscoat)
 Cyclodialysis spatula
Cyclodialysis spatula
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


