CHAPTER 21 Corneal surgery

Corneal and anterior segment trauma
Amit Patel, Massimo Busin and Carlo Enrico Traverso
Corneal laceration
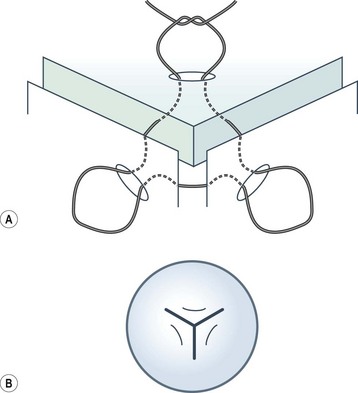
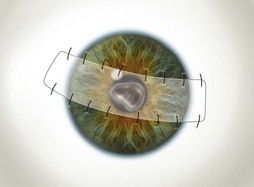
Viscoelastic may be injected through the wound or via a paracentesis to reform the anterior chamber if required. 10.0 Nylon is preferably used to close the corneal laceration. The placement of the primary suture depends on the configuration of the wound. When linear, it is placed at the center of the wound with subsequent sutures bisecting the remaining portion. If angulated, the primary suture is placed at the apex of the laceration. Stellate ruptures are difficult to repair and may require triangular, ‘X’ or purse-string sutures (Fig. 21.1). Attempts should be made to place sutures outside the visual axis if possible.
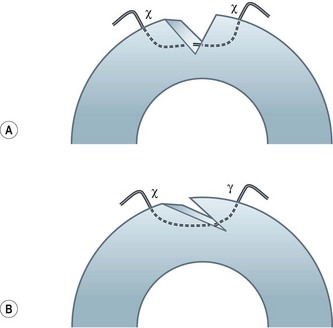
Particular care should be taken when placing sutures in bevelled lacerations. The entry and exit points of the sutures should be appropriately placed in order to avoid overriding of the wound edges or dehiscence secondary to ‘cheese-wiring’ of the tissue (Fig. 21.2).
Hyphema
Most traumatic hyphemas may be treated medically; however, surgical intervention should be considered in cases with prolonged and severely raised IOP, which may lead to optic nerve damage and corneal staining1. The corneal staining may develop rapidly, especially in younger individuals, but can take several months or years to clear.
Removal of the blood clot may be carried out with a mechanical vitrector or irrigation and aspiration2. Two paracenteses are made and an irrigation cannula or anterior chamber maintainer placed in one and a vitrector in the other. The aspiration and cutting functions of the vitrector are effective in removing the clot whilst minimizing traction on the iris and iridocorneal angle. Irrigation and aspiration may also be used without the cutter; however, the clot may be too thick to be evacuated and may result in unnecessary traction.
Postoperative care
Post-traumatic septic endophthalmitis carries a poor prognosis and, given the higher risk as well as the fact that it may be difficult to distinguish from the effects of trauma itself (i.e. pain, redness, inflammation, and reduced vision)3, prophylactic antibiotics must be prescribed in all cases.
Conjunctival flap surgery
Amit Patel, Carlo Enrico Traverso and Massimo Busin
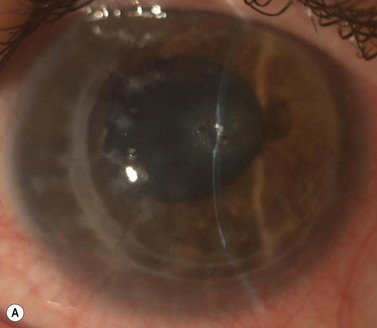
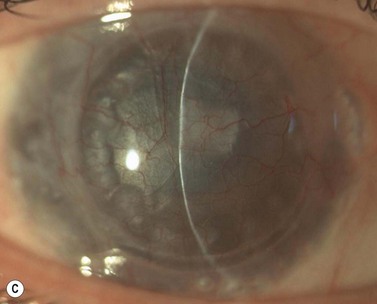
Of the numerous techniques to cover the cornea with conjunctiva, the total conjunctival flap popularized by Gundersen4 and the partial conjunctival flap are the most effective. The aim of conjunctival flap surgery in ocular surface disease and ulceration (both infectious and non-infectious) is to prevent stromal melting and possible perforation, thus stabilizing the eye and eventually allowing later surgery aimed at rehabilitating vision. However, for conditions that do not allow later corneal surgery (i.e. extreme dry eyes, high grade stem cell deficiency, etc.) a conjunctival flap may be compatible with vision up to 20/400 (see Fig. 21.4C).
Indications
Conjunctival flaps may be utilized in a variety of corneal diseases that are not responsive to medical management, induced ptosis, or tarsorrhaphy. Chronic ocular surface disease and non-healing corneal epithelial defects are excellent candidates for flap surgery5. It has also been used to stabilize the eye in chronic and non-response viral, bacterial, and fungal corneal infections6–8. In the presence of a descemetocele or perforation, a corneal patch must be carried out prior to considering a conjunctival flap.
Along with providing corneal support and fibrovascular tissue to fill epithelial defects, the associated blood supply aids to bring immunoglobulins, anticollagenases, and systemic antibiotics to the lesion9. This advantage is not afforded when applying non-living tissue such as amniotic membrane. Other indications include neurotrophic ulcers, marginal ulcers, exposure keratopathy, and bullous keratopathy with low visual potential.
Surgical technique
Total conjunctival flap
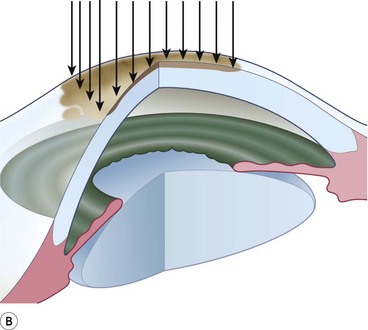
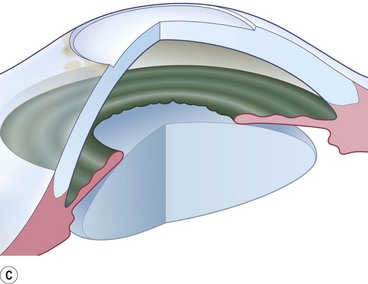
A 6.0 silk or polyglactin 910 traction suture may be placed through the cornea near the limbus to allow downward rotation of the globe during flap dissection. The superior conjunctiva is dissected from the underlying Tenon’s tissue by injecting 1–2 ml of local anesthesia (e.g. 1–2% lidocaine) or balanced salt solution with a 27 gauge needle. Epinephrine in a dilution of 1 : 100 000 may be added to achieve temporary vasoconstriction. The injection site should be situated away from the conjunctiva intended for flap use so as to prevent creating a ‘buttonhole’. A small horizontal incision is made with Wescott scissors at the fornix through conjunctiva, but not into Tenon’s fascia. Then the blunt and sharp dissection is performed with Wescott scissors and non-toothed forceps, separating conjunctiva from Tenon’s, ideally in the plane created by the local anesthesia. Dissecting the conjunctiva with the scissors placed underneath (Fig. 21.3A and B), as opposed to under direct visualization, ensures that the correct plane is maintained and minimizes the risk of buttonhole formation. The dissection is carried out in a meticulous fashion to the limbus and care is taken to avoid buttonholes, although this may be difficult in eyes that have had chronic inflammation, scarring, surgery, or trauma.
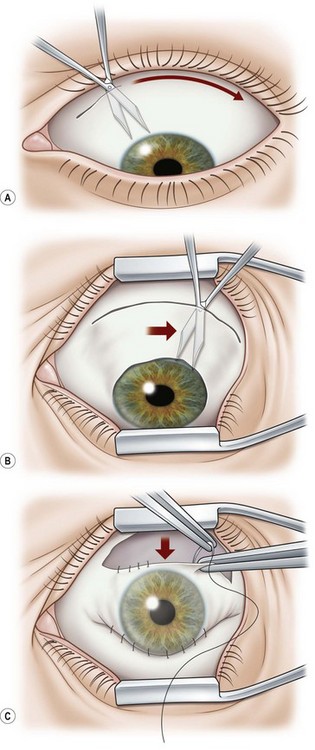
Once most of the conjunctiva is dissected down to the limbus, the horizontal incision can be extended several millimeters toward the nasal and temporal canthi (Fig. 21.3B). The nasal and temporal portions of the flap then need to be undermined. Once the entire flap has been created, the conjunctival dissection is continued forward until it comes free at the limbus. A 360° conjunctival peritomy is then performed. A small amount of undermining of the inferior limbal conjunctiva often makes the peritomy and subsequent suturing of the conjunctival edge easier. The limbus is then debrided of any remaining epithelium.
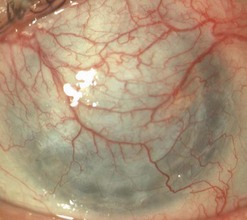
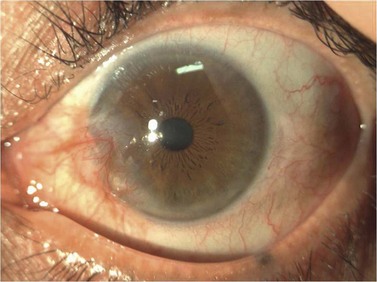
Buttonholes of the flap are the most common intraoperative complication and can lead to flap retraction. These should be closed with interrupted or purse string sutures and, if located in an area of flap that covers the cornea, the sutures should be anchored to the underlying cornea. Fig. 21.4 illustrates the pre- and postoperative appearance of a total conjunctival flap. Failure to separate Tenon’s fascia from the overlying conjunctiva leads to fibrovascular proliferation and poor transparency (Fig. 21.5).

Partial conjunctival flaps
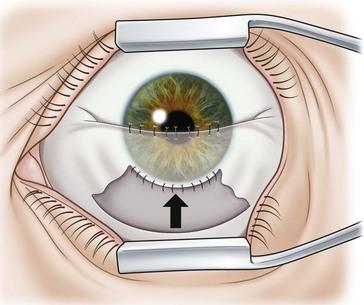
Localized limbal and paralimbal lesions in an otherwise healthy cornea may occasionally be treated with a partial conjunctival flap. The corneal epithelial debridement is carried out in the area expected to be covered by the conjunctival flap and the conjunctiva is ballooned with local anesthesia as described above. The width of the conjunctival flap should be approximately 1.5 times the width of the lesion to be covered in order to allow for proper suture placement and account for late flap retraction. In order to secure the conjunctival edge onto the cornea and prevent dehiscence and retraction, it is important to create a ledge of cornea into which to suture the conjunctiva. A groove is made into healthy cornea at the edge of the intended extension of the flap with a diamond or metal blade and a small triangular strip of cornea is removed to create a ledge (Fig 21.6).
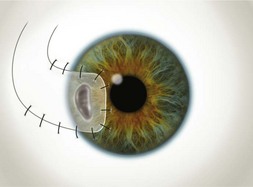
The partial flaps may be fashioned in various ways. A simple advancement flap is created much in the same manner as a total flap; however, the amount of conjunctival dissection is smaller and the edge of the flap is sutured on to the cornea with 10-0 nylon sutures. An advancement flap is prone to retraction with time and a relaxing incision through the conjunctiva and Tenon’s tissue, away from the limbus, may reduce the likelihood and allow the bulbar conjunctiva distal to the incision to retract. A pedicle (Fig. 21.7) or bridge flap (Fig. 21.8) may be considered as alternatives. A bridge flap may be created with a narrow band of conjunctiva that runs across the corneal lesion allowing a greater view of the anterior chamber. Edges of the flap overlying the cornea are sutured with 10-0 nylon and those overlying episclera with 8-0 polyglactin 910 (e.g. Vicryl). Non-absorbable suture knots must be buried.
Pterygium surgery
Amit Patel, Carlo Enrico Traverso and Massimo Busin
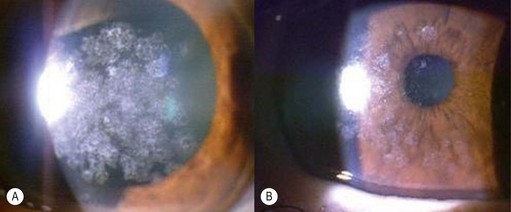
A pterygium (from the Greek pterygion meaning ‘wing’) is a degenerative wing-like fleshy mass of bulbar conjunctival and subconjunctival tissue that arises at the limbus and encroaches onto the corneal surface (Fig. 21.9). It consists of an elevated leading edge (head) and a broad triangular fibrovascular mass (body). Although it most commonly originates from the nasal limbus, temporal or simultaneous nasal and temporal pterygia may occasionally exist. Histopathologically, it is characterized by fibrovascular proliferation and ‘elastotic degeneration’, i.e. positive to elastic tissue stain, but is not sensitive to elastase. In addition, there is alteration of the basal corneal epithelial layer, destruction of Bowman’s layer, and scarring of the superficial corneal stroma.
Although the precise pathogenesis of pterygia formation remains speculative, it is largely thought to be related to ultraviolet light exposure10,11. This is supported by its formation in the interpalpebral fissure as well as the higher prevalence among people living closer to the equator and in those with outdoor occupations. Ocular surface irritation from dust, sand, etc. has also been implied as a causative factor.
Surgical technique
Primary pterygium
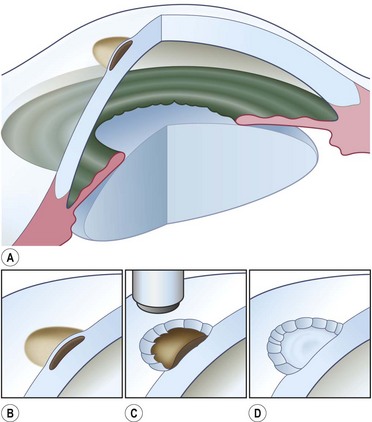
The outline of the pterygium is marked with a gentian violet marker, and anesthetic or balanced salt solution is injected subconjunctivally to balloon the pterygium (Fig. 21.10A). This allows easier dissection and protects the underlying rectus muscle from accidental damage.
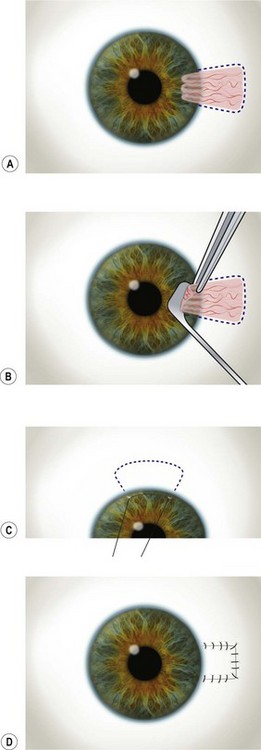
The head of the pterygium is lifted with fine toothed forceps and gentle dissection using a rounded sharp blade (e.g. Beaver No. 57) or Tooke’s knife is employed to roll the tissue towards the limbus (Fig. 21.10B). A superficial keratotomy may be made to outline the leading edge prior to the dissection and a superficial plane of dissection is maintained up to the limbus. Attempts must be made to maintain a level and smooth plane of dissection. On reaching the limbus, the bulbar portion (body) of the pterygium is then excised carefully down to the sclera using Wescott scissors. Particular attention should be paid in dissecting and removing all the underlying Tenon’s tissue. To minimize the risk of recurrence, this dissection should lead to complete removal of all the hypertrophic fibrotic tissue underlying the pterygium and must be carried out up to the recti perimysium, into which it usually blends. The gentian violet marks allow visualization of the margins following the subconjunctival injection and avoid inadvertent excision of the plica semilunaris and caruncle. Wet field cautery may be applied sparingly to achieve hemostasis. Remnant tissue at the limbus and sclera is scraped using a rounded blade or large diamond burr.
The rolled edges of the remaining conjunctiva are unraveled with forceps, and the conjunctival defect is then measured with calipers. The globe is rotated upward with the limbal traction suture and the inferior bulbar conjunctiva away from the pterygium excision is exposed. In general, it is advisable to spare the superior conjunctiva, in case filtration surgery is needed later in life. A limbal edge is preferred and a gentian violet marker is used to mark the outline of the remaining three sides of conjunctival graft to be created (Fig. 21.10C). The conjunctiva is dissected from the underlying Tenon’s tissue by injecting 1–2 ml of local anesthesia (e.g. 1%–2% lidocaine) with a 27-gauge needle. The injection site should be situated away from the conjunctival graft intended for use so as to prevent creating a buttonhole. A small incision is made just peripheral to the superior corner of the marked area. Blunt and sharp dissection is performed with Wescott scissors and non-toothed forceps to ensure that the conjunctiva is separated from Tenon’s, ideally in the plane created by the local anesthesia. The dissection is carried out in a meticulous fashion to the limbus and care is taken to avoid buttonholes. Once the conjunctiva is dissected free from the underlying Tenon’s, the edges of the graft are cut slightly larger than the outline marks. This allows for the natural tissue shrinkage and also incorporates the gentian violet marks, which are useful in aiding graft orientation.
Once the edges of the graft are approximated to the edges of the bulbar conjunctiva, absorbable sutures (e.g. polyglactin) are used to secure the graft. The first sutures are positioned through the two limbal corners of the graft, into sclera, and then into conjunctiva to place the limbal edge of the graft on gentle stretch. If the limbal edge is on good stretch, no additional sutures are required. The next two sutures secure the posterior corners of the graft to the bulbar conjunctiva. Additional sutures are placed to close the wound edges and horizontal mattress sutures may be used to anchor the edges to the underlying sclera (Fig. 21.10D). It is important to suture the graft to conjunctival edges, and not just Tenon’s, as these two tissues may appear similar. A wet swab may be used to distinguish between the two, as Tenon’s tends to stick to the swab whereas conjunctival tissue does not. The conjunctival defect in the area from which the graft is harvested may be sutured, but is usually allowed to re-epithelialize spontaneously. Suture knots are not generally buried and any buttonholes are sutured and anchored to the underlying sclera.
Excimer laser phototherapeutic keratectomy
Angelo Macrì and Carlo Enrico Traverso
Excimer laser phototherapeutic keratectomy (PTK) has been performed to treat anterior corneal pathology for the last 20 years. FDA approved PTK in 199513. Since then indications and techniques have continuously evolved.
Indications and contraindications
The three diagnostic categories better responding to PTK are:
As with any corneal surgery, caution should be taken in patients with potential corneal healing abnormalities, such as neurotrophic corneas (e.g. after herpes simplex or herpes zoster keratitis), exposure keratitis, severe keratoconjunctivitis sicca or blepharitis, collagen vascular conditions (e.g. rheumatoid arthritis) and diabetes mellitus. Additionally, patients with herpes simplex keratitis are at risk14–16.
Recurrent corneal erosions
Recurrent corneal erosion syndrome with anterior basement membrane dystrophy was treated in the past with simple epithelial debridement, therapeutic contact lenses, or anterior stromal puncture. However long-term data have proved that diamond burr superficial keratectomy at the slit lamp and, above all, PTK have significantly minor recurrences13,17,18.
Stromal lesions
Best results are obtained when the opacities are in the anterior 20% of the cornea. It is a general opinion that PTK may be tried in all patients with dense superficial opacities before undergoing a more invasive procedure, such as lamellar or penetrating keratoplasty13,19.
Corneal haze after excimer laser corneal surgery
PTK can be also used to treat late haze and subepithelial scarring after PRK (Fig. 21.11). In both cases MMC is utilized because predominant effect of MMC in blocking haze formation was at the level of profound inhibition of the replication of keratocytes and myofibroblast progenitor cells in the corneal stroma that occur following the normal keratocyte apoptosis response to epithelial removal during surface ablation.
Technique
The technique varies according to size, shape, density, and numbers of the cornea lesions (Figs 21.12 and 21.13).
Elevated lesions are generally debulked with a blade before PTK.
PTK can be also performed topographically guided or ‘customized’13,21.
Commonly MMC is used at 0.02% (0.2 mg/ml) concentration, on a 6–8 mm circular sponge for 60 seconds; it is then irrigated with 30 ml of saline13,20,22. Other regimens are also suggested.
Postoperative treatment
Pain is the most important issue in the early postoperative period. Immediately after surgery, the eye is treated with either a bandage soft contact lens or a pressure patch. Ice packs are often very effective in treating the pain. Strong anti-pain medications are also widely used. Eyes with BSCLs are treated with topical antibiotic drops. The pressure patch is removed from the other eyes after 1 day and frequent antibiotic ointment is prescribed. Patients are followed every few days and the antibiotics are continued until the epithelial defect heals. There is a higher risk of postoperative problems such as poor healing, infection, and scarring after PTK than after routine keratorefractive surgery, as these corneas are usually not ‘normal’13.
Summary
PTK is a very versatile technique that is quite effective at treating a wide variety of anterior corneal lesions (Figs 21.14 and 21.15) with a low risk rate if performed properly. In particular elevated lesions and opacities in the top 10–20% of the corneal stroma generally do very well. If unsuccessful, an anterior lamellar graft can almost always be performed and thus PTK may be tried before proceeding to a corneal transplant, considering its excellent risk/benefit ratio13.

Corneal transplantation
Massimo Busin, Amit Patel, Davide Venzano and Carlo Enrico Traverso
Historical perspective
There is considerable debate regarding who first came forth with the concept of replacing diseased or scarred corneas with living tissue. Guillaume Pellier de Quengsy first suggested replacing the diseased cornea with a thin glass disc (similar to a keratoprosthesis) in 1789, and Erasmus Darwin, grandfather of the famed Charles Darwin, first suggested replacing a scarred cornea with a small piece of living donor corneal tissue. Franz Reisinger published the results of his experiments on corneal transplantation in rabbits and chickens in Germany in 182423–25. S.L. Bigger successfully replaced the scarred cornea of his pet gazelle with a healthy donor cornea from another gazelle in 183724. Richard Kissam, a New York ophthalmologist and general practitioner, was the first to operate on a human using a pig donor cornea; however, the graft became opaque shortly thereafter24. The advent of ether and chloroform inhalation anesthesia, topical cocaine anesthesia, local infiltrative anesthesia, and antiseptic surgery during this early period revolutionized corneal transplantation, as it also did for many other types of surgery.
These important companion discoveries were undoubtedly instrumental in accelerating the progress of corneal transplantation. Considerable amounts of experimental work using living corneal grafts ensued. Von Hippel was the first to improve vision with LK, consisting of a full-thickness rabbit donor cornea placed into a human recipient lamellar bed24. He was also the first to use a circular trephine. In 1906 successful total penetrating corneal graft in a human was reported by Zirm in a laborer with bilateral lye burns to the cornea26. Ironically, alkali burns like this are now known to have one of the worst transplantation prognoses. Anton Elschnig of Prague, with his extensive experimental and clinical work in the 1920s through the 1930s, is credited with refining the crude technique into an elegant, reliable procedure. Filatov, Tudor Thomas, Paton, Franceschetti, Paufique, Sourdille, Castroviejo, Arruga, and the Barraquer brothers, all eminent surgeons, based much of their knowledge and methodologies on the foundation laid by Elschnig24. Ramon Castroviejo, a Spanish ophthalmologist practicing in New York City, initiated detailed grafting methodologies, expounding the use of the square graft (Fig. 21.16), and developing and refining keratoplasty instrumentation. A. Edward Maumenee extensively studied the immunology and physiology of corneal graft rejection. Claes H. Dohlman came to the United States from Sweden and established the first cornea fellowship program in 1961, emphasizing the importance of both clinical and research training. With more recent ophthalmological advances consisting of microscopic surgery, inert sutures, antiviral and antibiotic medications, topical and systemic corticosteroids, tissue-preservation/eyebanking strategies, and progress in immunology, the success of corneal transplantation has grown rapidly over the last 30 years. Paralleling these advances, clinical indications for corneal transplantation surgery have also expanded considerably.
The last decade witnessed a strong expansion in the use of lamellar techniques.
The anterior lamellar keratoplasty performed with deep stromal separation, described by Melles (DALK) enables the surgeon to leave the recipient with healthy endothelium, with good visual results27,28.
Endothelial decompensation being the leading indication for PK procedures29–34, there has been strong interest in developing a technique able to preserve the healthy recipient stroma.
Since the original description of the posterior lamellar keratoplasty (PLK) described by Tillett and Barraquer in the 1950s and 1960s, in 1999 Melles demonstrated the first sutureless PLK35. Since then, numerous modifications in surgical technique and new instruments have led to increasing popularity of PLK.
Indications
Indications for keratoplasty have varied over the decades36–38. Box 21.1 lists the classical indications for PK; today many of these conditions may be effectively treated with LK. The Eye Bank Association of America recorded over 41 000 transplants performed in the United States in 2008, with a simultaneous increase in grafts provided for endothelial keratoplasty38. Whilst keratoconus and aphakic bullous keratopathy were major indications for corneal transplantation three decades ago, pseudophakic bullous keratopathy (PBK) rapidly emerged as a leading indication in the 1980s and 1990s38–41. This coincided with the dramatic increase in the number of cataract extractions performed. Optical indications for transplantation include corneal decompensation (e.g. bullous keratopathy and endothelial dystrophies), ectasia (e.g. keratoconus), scarring (e.g. traumatic, post-infectious or iatrogenic), and stromal dystrophies. Tectonic indications (e.g. melting, descemetoceles, perforation) are aimed primarily at preserving globe integrity and may allow optical improvement simultaneously or at a later stage. Therapeutic indications (e.g. medically unresponsive infections) provide the two-fold advantage of excisional biopsy and of elimination of the infected tissue. Causative organisms in these cases are often fungi or acanthamoeba, however, common pathogens causing microbial keratitis may also necessitate therapeutic keratoplasty.
Eye banking/donor selection
The first successful human corneal transplant by Eduard Zirm in 1905 involved the use of fresh corneal tissue from a boy whose eye was enucleated for a penetrating sclera injury. For approximately the following 30 years, all human keratoplasties were performed using fresh corneal tissue from living donors whose eyes had been enucleated due to trauma or disease not involving the anterior segment. In 1937, Filatov from the Ukraine introduced the use of whole globes from cadavers stored at 4°C in a moist chamber. Paton established in the US the first eye bank that involved procurement, processing, and distribution of donor corneas37.
Thus, cold storage and organ culture are the two main methods for preserving the donor tissue today. Cold storage (2–6°C) was introduced in 197442,43, and is commonly used in the USA. The technique is relatively simple and involves refrigeration with minimal tissue handling. No complex equipment is required. At 2–6°C, the metabolic activity of the endothelial cells is minimal and therefore deturgescent agents (e.g. dextran or chondroitin sulfate) are required to keep the cornea in a relatively dehydrated state and thus maintain corneal thickness. The original McCarey-Kaufman (M-K) medium has been modified with addition of antibiotics, energy sources, antioxidants, growth factors, and membrane stabilizing agents to improve cell survival, reduce autolysis, and maintain ultrastructural integrity. Although endothelial cell loss may be attributable to numerous factors independent of storage technique, corneas stored at 2–6°C show intercellular disruption, reduced cell adhesion as well as endothelial cell loss and death44. Modified storage media have increased the storage time for up 2 weeks, one week being most often recommended. Organ culture (31–37°C) was introduced in 197645 and is commonly used in Europe. During the storage phase in culture medium supplemented with fetal or newborn calf serum, antibiotics and antimycotics, the corneas swell considerably and can reach twice the normal thickness. Dehydrating molecules are not added as they are ingested by the corneal cells and lead to toxicity. Thus, a shorter second phase is required to reverse the swelling prior to transplantation. Dextran (4–8%), is added to the same medium to facilitate de-swelling and transportation. This phase in transport medium varies between 1 and 7 days. Overall, organ culture allows for longer periods of storage (up to 4–5 weeks). Advantages over cold storage include ease of scheduling surgery, allowing time for tissue typing/matching, and more rigorous microbiological testing.
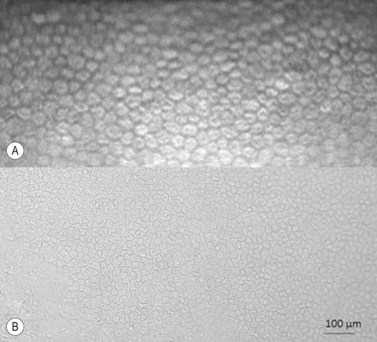
Regardless of the storage methods used, donor and tissue evaluation to assess suitability is critical. It includes obtaining a thorough medical and social history of the donor as well as serological testing, slitlamp biomicroscopy, and endothelial cell examination. The tissue is evaluated for epithelial integrity, epithelial and stromal opacities, presence of foreign bodies and infectious infiltrates, evidence of previous anterior segment surgery, degree of stromal clarity and thickness, presence of Descemet’s membrane folds and extent of endothelial guttae, snail tracks, and precipitates. Specular microscopy provides detailed microscopic analysis of individual cell morphology and an estimate of cellular density (Fig. 21.17A), however for a better and wide examination light microscopy is applied (Fig. 21.17B). The cell counts may be obtained by automated image analysis or manual counting methods.
Donor tissue has to be considered as non-sterile and effective decontamination must be in the routine. Antibiotics are less effective in cold storage than organ culture as the contaminating microbes are metabolically less active at low temperatures. For this reason, preoperative warming of the storage media is important to enhance the decontamination effect. Individuation of microbial contamination may also be better with organ culture since contamination will become more readily evident and it may therefore be considered as the storage method of choice in circumstances where corneas are suspected of being at a higher risk of contamination. However, stringent screening protocols by eye banks have minimized the risk of microbial transmission from donor to recipient and the accurate valuation of medical and social history of the donor allowed rare incidences of systemic disease like rabies, hepatitis B, Creutzfeldt–Jakob disease (CJD) and malignancies44–48. No case of seroconversion after unplanned transplantation of corneas from human immunodeficiency virus (HIV) positive patients has been reported to date49–51.
Irrespective of the storage methods, prospective studies analyzing short and long-term follow-up after PK have not found any difference in endothelial cell density or clinical outcomes52–54.
Preoperative evaluation
Examination and investigations
The status of the crystalline lens or the IOL should be assessed to ascertain the need for concurrent cataract extraction or IOL repositioning, explantation, or exchange. Preoperative biometry may not be as predictive of the final refractive status when IOL implantation is combined with PK as when it is performed in the absence of corneal disease or surgery. A combination of good clinical judgment, measurements from the other eye, reasonable choice of IOL formulas, and personalization of equations using regression analysis to estimate the surgeon’s refractive tendencies, may enhance the predictability; high refractive errors are still occurring in combined PK/IOL cases55,56.
The decision to render the eye myopic, emmetropic, or hyperopic should be influenced by the patient’s need, and the refractive status of the contralateral eye. In general, a final myopic error will lend itself better to further correction with laser or surgical treatment. The condition of the iris/iridocorneal angle and integrity of the capsular bag may be a determinant of the type of IOL to be implanted. Alternatively, the eye may be left aphakic, with view to secondary IOL implantation at a later stage. This may yield better postoperative refraction and unaided visual acuity but delays visual rehabilitation and risks damage to the graft57,58.



