Corneal and Conjunctival Manifestations of Dietary Deficiencies
Peter C. Donshik
Dietary deficiencies rarely produce clinical disease in developed countries; however, they are an important factor in the production of systemic and ocular disease in other parts of the world. Ocular problems associated with vitamin A deficiency and protein-energy malnutrition are the most common. Hundreds of thousands of preschool-age children may be afflicted each year with potentially blinding consequences of poor nutrition. The clinical disease, together with limited or poor access to preventive and curative health services, leads to enhanced ophthalmic disease. Although there is wide variability in the prevalence of the ocular manifestation of vitamin A deficiency (1), an example of the potential magnitude of the problem is indicated by a study performed in Aborigine children in Malaysia. In this study, night blindness was found in 16% of the children, conjunctival xerosis in 57.3%, Bitot’s spot in 2.8%, and corneal xerosis in 0.5% (2). It is estimated that in Africa, Asia, and South America, 10 million new cases of xerophthalmia occur per year, of which 280,000 to 500,000 result in blindness (3). Worldwide vitamin A deficiency is probably the leading cause of blindness in children, with approximately 228 million children affected (4).
TYPES OF MALNUTRITION
Two categories of malnutrition have been associated with specific clinical syndromes in children. These are marasmus, a generalized protein-energy deficiency, and kwashiorkor, which is associated primarily with protein deficiency. Both of these conditions are seen most frequently in those between weaning and 6 years of age. Ocular manifestations of vitamin A deficiency are seen in both conditions.
Marasmus
When environmental factors, such as widespread famine, lead to chronic deficiency of all food categories, marasmus results. This manifestation of starvation is illustrated in Fig. 50-1, which shows the small and poorly developed child. Body fat does not develop, muscles waste away, the muscle tone is significantly deceased, skin elasticity is lost, and there is mental dullness. The eyes are staring, with a decreased blink rate. There is little animation or response to stimulation, and if the child does cry, it is usually a very weak cry.
The prognosis for children with marasmus is guarded. It is estimated that 40% of children who are treated for marasmus will ultimately die of starvation. One of the main factors for the poor prognosis is that even if the child is treated in the hospital, once he or she returns home, the underlying problems that caused the condition in the first place have not changed. These children are at high risk for development of vitamin A deficiency, and they are also more vulnerable to the complications of routine childhood diseases such as measles or herpes simplex infection.
Kwashiorkor
Kwashiorkor occurs when an infant is placed on a diet high in carbohydrate and low in protein. There is an insufficient supply of essential amino acids, which affects normal protein synthesis. This results in an inability to maintain the usual intravascular volume, which results in edema. Clinically, a child with kwashiorkor has edema of the abdomen and extremities with wastage of the musculature (Fig. 50-2). A change in the color and texture of the hair with a loss of the usual pigmentation as well as coarsening of the hair strands can also occur. In addition, because vitamin A is transported on protein carriers, the abnormalities of protein synthesis can have a direct effect on the transport of vitamin A.
Nonspecific Protein-Energy Malnutrition
When malnutrition in children and adults does not result in either marasmus or kwashiorkor, the nutritional deficiencies
may be classified under a more general term of protein-energy malnutrition. In these conditions, replacement therapy should include a wide variety of nutrients (5). The tissues and organs usually affected are those in which cells are constantly turning over and being replaced. Thus, the skin and mucous membranes, hematopoietic tissue, and the gastrointestinal tract are commonly affected. The effect on the gastrointestinal tract reduces absorption, which compounds the inadequate intake of food with malabsorption. Vitamin A deficiency is frequently associated with nonspecific protein-energy malnutrition.
may be classified under a more general term of protein-energy malnutrition. In these conditions, replacement therapy should include a wide variety of nutrients (5). The tissues and organs usually affected are those in which cells are constantly turning over and being replaced. Thus, the skin and mucous membranes, hematopoietic tissue, and the gastrointestinal tract are commonly affected. The effect on the gastrointestinal tract reduces absorption, which compounds the inadequate intake of food with malabsorption. Vitamin A deficiency is frequently associated with nonspecific protein-energy malnutrition.
 FIGURE 50-1. Marasmus. This disease is caused by a chronic deficiency of all food categories. |
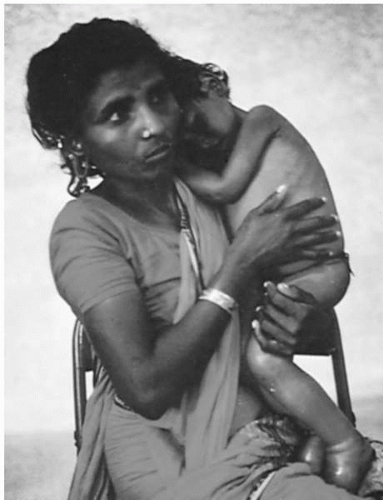 FIGURE 50-2. Kwashiorkor. The manifestations of this clinical entity are due largely to protein deficiency. A characteristic feature is massive edema of the abdomen and extremities, concurrent with muscle wastage. |
VITAMIN A DEFICIENCY
Vitamin deficiencies occur in the presence of protein-energy malnutrition, and it is often impossible to separate them. However, of the vitamin deficiencies, vitamin A deficiency is the most important cause of ocular diseases, and a number of clinical conditions are ascribed specifically to vitamin A deficiency. In addition, many of these conditions can be reproduced in a vitamin A-deficient animal model (6,7).
Vitamin A is found in foods such as milk, eggs, fish, meat, and liver. It is fat soluble, ingested in the form of retinol. In the mucosal cells of the small intestine, it is esterified to palmitic acid. Vitamin A can also be obtained from its precursors, the carotenes. These substances are found in yellow fruits, green leafy vegetables, and red palm oils (8). In the small intestine, they are metabolized into retinol and absorbed. However, the carotenes are not active biologically, and it requires six times by weight to achieve the same metabolic effect as ingestion of retinol (9). After retinol is esterified to palmitic acid, the retinyl palmitate then travels to the liver through the lymphatic system. When metabolic demands require vitamin A, retinyl palmitate is hydrolyzed to retinol, released from the liver, attached to retinol-binding protein (RBP), a carrier protein produced by the liver, and transported by the bloodstream to the required tissue, such as the conjunctiva or cornea. Vitamin A is important in conjunctival cell RNA and glycoprotein synthesis, which are necessary in maintaining the health of the conjunctival mucosa and corneal stroma. Both zinc and protein are required for the production of RBP, without which vitamin A cannot be transported (10).
In the neonatal period, the child depends on the mother’s milk for vitamin A. The levels of vitamin A in breast milk are similar to plasma levels (40 μg/100 mL) (11). Thus, if the mother is deficient in vitamin A, the child’s supply of vitamin A is also deficient. This is one of the reasons why vitamin A-deficient ocular surface diseases are more prevalent in young children. They are born with low vitamin A stores, get little from breastfeeding, yet have the demands of rapid growth and the added complication of infectious childhood diseases that increase the body’s requirements for vitamin A (10).
Abnormalities involving the ocular surface secondary to vitamin A deficiency are referred to as xerophthalmia. In 1976, the World Health Organization (WHO) published a classification for xerophthalmia (12), which was modified in 1982 (13).
Classification | Primary Sign |
|---|---|
X1A | Conjunctival xerosis |
X1B | Bitot’s spot with conjunctival xweosis |
X2 | Corneal xerosis |
X3A | Corneal ulceration with xerosis |
X3B | Keratomalacia |
XN | Night blindness |
XS | Corneal scars |
Biochemical criterion | Plasma vitamin A 0.35 umol/L (10 μg/dl) or Less |
Ocular Manifestations of Vitamin A Deficiency
X1A: Conjunctival Xerosis
Dryness, lack of wettability, loss of transparency, thickening, wrinkling, and pigmentation are features of conjunctival xerosis. The dry patches often stand out “like sandbanks at receding tide” (14) and usually stain with rose bengal or lissamine green. The bulbar conjunctiva, especially the temporal interpalpebral areas, is usually involved. Histologically, there is a change in the conjunctival epithelium. The epithelium changes from its normal columnar appearance to a stratified squamous appearance. There is a loss of goblet cells and the epithelium becomes keratinized. The severity of these findings depends on the severity of the condition. Conjunctival disease is more common in children between 3 and 6 years of age. This sign can easily be overdiagnosed, especially because there is often observer variability. In addition, conjunctival thickening, wrinkling, and pigmentation can be seen in chronic ultraviolet light, smoke, and dust exposure, and eye infections (15). As a result, this is considered a “soft sign” in evaluating nutritional eye disease in a population. However, the dry patches, especially if they extend to and involve the inferior conjunctiva, are a fairly reliable sign of vitamin A deficiency (16).
X1B: Bitot’s Spot with Conjunctival Xerosis
A Bitot’s spot is a small, light-gray plaque with a foamy surface that appears on the bulbar conjunctiva in the temporal or nasal quadrants, and is frequently bilateral (Fig. 50-3). Histologically, an inflammatory infiltration of the subepithelial tissue is present. The conjunctival epithelium is keratinized and shows acanthotic thickening and loss of goblet cells (signs of xerosis). The Bitot’s spot is a mixture of keratin, bacteria (often Corynebacterium xerosis is present), and occasionally fungi (17). The “foamy” appearance is thought to be due to the mixture of bacteria and mucus (18). Although the foamy spots can be removed, the underlying base remains and the foamy spots reform in a few days.
There has been some question as to whether Bitot’s spots are always associated with vitamin A deficiency because there are cases in which the Bitot’s spot does not respond to vitamin A therapy. Sommer has reported that nasally located Bitot’s spots are a more reliable sign of vitamin A deficiency than temporally located lesions. In addition, he found that in children younger than 6 years of age, 97% of the lesions were responsive to vitamin A therapy, whereas 60% of the lesions in children older than 10 years were unresponsive to therapy. Thus, the presence of Bitot’s spot accompanied by conjunctival xerosis in a child younger than 6 years of age is strong evidence of vitamin A deficiency (10). However, serious eye disease can occur in vitamin A deficiency without the presence of a Bitot’s spot. The disease does not necessarily progress through the stages of the WHO classification.
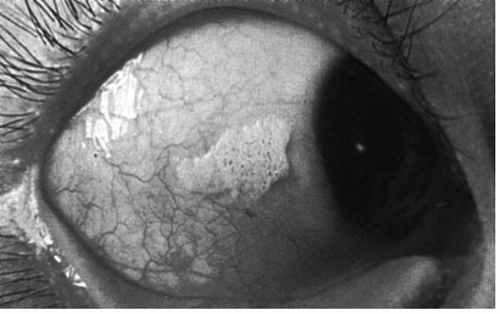 FIGURE 50-3. Bitot’s spot, a foamy, light-gray area of conjunctiva frequently found in vitamin A deficiency in humans. (From Sommer A. Nutritional blindness: xerophthalmia and keratomalacia. New York: Oxford University Press, 1982, with permission.)(see color image) |
X2: Corneal Xerosis
Corneal involvement can first appear as superficial punctate staining involving the inferior-inferonasal corneal surface. It can then progress to involve the entire corneal surface. As the corneal involvement progresses, a roughened, lusterless, dull appearance of the cornea develops, with keratinization and stromal edema (19) (Fig. 50-4). The corneal
surface becomes less wettable and the tear breakup time is significantly reduced as a result of corneal surface changes. This leads to desiccation of the corneal epithelial cells. The accumulation of keratin debri and bacteria can form lesions that resemble Bitot’s spots (20).
surface becomes less wettable and the tear breakup time is significantly reduced as a result of corneal surface changes. This leads to desiccation of the corneal epithelial cells. The accumulation of keratin debri and bacteria can form lesions that resemble Bitot’s spots (20).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


