Chapter 14
CORNEA

The cornea is frequently involved in facial and ocular trauma. As it provides most of the eye’s refractive power, recognition and management of corneal injuries is critical for vision; even small irregularities in the corneal contour may result in significant functional morbidity. This chapter reviews the evaluation and management of corneal injuries.
EPIDEMIOLOGY AND PREVENTION
Excluding corneoscleral injuries, the cornea is involved in 51% of all serious ocular trauma in the USEIR; additional information from this database follows.
Age (years):
• range: 0–101;
• mean: 30;
• ≤15: 26%;
• ≥60: 8%.
Sex: 83% male.
Place:
• 41% home;
• 18% work;
• 9% street and highway.
Cause:
• 27% sharp object;
• 20% blunt object;
• 6% MVC;
• 3% fall.
Rate of various diagnoses among all corneal injuries:
• laceration, full-thickness: 52%;
• laceration, partial-thickness: 1%;
• rupture: 18%;
• chemical burn: 5%;
• edema: 5%.
Rate of corneal ruptures among all ruptures: 29%.
Rate of corneal lacerations among all lacerations: 59%.
Rate of iris prolapse among corneal ruptures: 38%.
Rate of in-the-visual-axis iris prolapse among
ruptures: 19%.
Rate of iris prolapse among lacerations: 30%.
Rate of in-the-visual-axis iris prolapse among corneal
prolapses in lacerations: 19%.
The vast majority of these injuries are preventable with appropriate eye protection1 (see Chapters 4 and 27).
PATHOPHYSIOLOGY
The cornea is a five-layered tissue.
1. Epithelium, the most superficial layer, is 50 mm thick and consists of five to seven layers of cells. It is a highly active, rapidly reproducing tissue; when injured, the epithelium heals rapidly and without scarring, unless Bowman’s layer is involved. Under the epithelium and attached to the basal epithelial cells by an adhesion complexa is a basement membrane overlying Bowman’s layer.
2. Bowman’s layerb is not a true membrane but a condensation of the superficial stromal collagen.
3. The stroma makes up most of the corneal thickness and is composed of multiple lamellae of collagen fibersc packed in glycosaminoglycans. The collagen is produced by keratocytes, interspersed among the lamellae. These cells are similar to fibroblasts and can live up to 3 years.
4. Descemet’s membrane lines the posterior surface of the stroma, representing the basement membrane of the corneal endothelium.
5. Endothelium, the most posterior layer, is a single layer of hexagonal cells, which are responsible for pumping water out of the corneal stroma, thus maintaining corneal deturgesence. Endothelial cells are derived from neural crest origins, capable of only limited reproduction; they are extremely delicate and are easily damaged by hydrostatic, thermal, contusive, or concussive insults as well as by direct mechanical trauma. When a sufficient number of cells are incapacitated (death, loss, or dysfunctiond) and the endothelial density drops below a critical level, edema ensues: the cornea becomes swollen and cloudy.
see Chapter 27 for the strength of a healed wound.
EXAMINATION
History
The history frequently directs the course of subsequent laboratory and diagnostic testing. The event’s description by the patient or witnesses allows the examiner to understand the circumstances of the injury, predicting the injury severity/type, the structures likely to be involved, and the risk of occult trauma. Specific questions to be asked concern:
• foreign bodies;
• chemical exposure; and
• previous corneal surgery2–6 (see Chapter 27).
Inspection
Naked-eye
corneal trauma is frequently visible by naked-eye inspection in room illumination or with a penlight(Fig. 14–1).
• Elevate the upper and depress the lower eyelid to view the entire cornea.
• Examine the cornea while swinging the penlight through a variety of angles.e This maneuver permits examination of the corneal surface and highlights abnormalities such as foreign bodies and lacerations, especially with tangential illumination or illumination near the limbus.
PEARL… Epithelial defects can be visualized by looking at the light reflex from the corneal surface. The normal cornea has a high luster with a smooth reflective surface. Irregularities in the light reflex may indicate loss or denudation of the epithelium and possibly stroma.
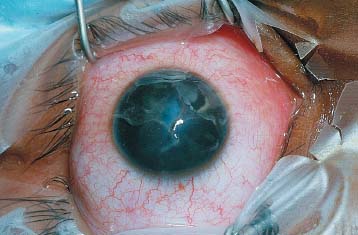
FIGURE 14–1 Corneal trauma can frequently be visualized with a penlight. In this photograph of a young boy with a corneal laceration, the edges of the laceration can be appreciated both by direct visualization and by the light reflex from the wound edge. Note also the opacified lens behind the laceration, indicating an injury involving deeper structures.
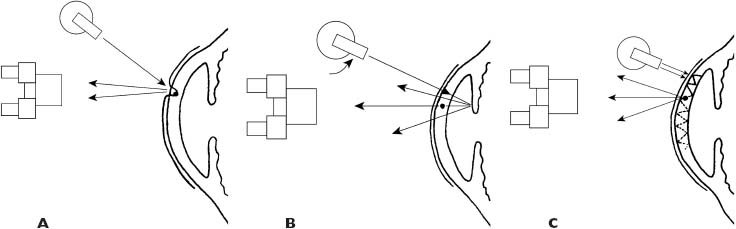
FIGURE 14–2 Diagrammatic representation of various slit-lamp illumination techniques helpful in visualizing corneal trauma. (A) Direct illumination: the cornea is illuminated directly with the slit beam. The lesion is seen by light scattering from its anterior surface. (B) Retroillumination: the light source is rotated off axis and the iris is illuminated. The examiner inspects the overlying cornea via light reflected from behind. This technique is especially useful for clear foreign bodies or wounds. The source of posterior illumination can also be the fundus red reflex. (C) Sclerotic scatter utilizes the total internal reflection of light within the cornea. Rotating the slit turret, the light beam is directed at the limbus. The cornea is inspected for discontinuities in the stroma. This technique is helpful when searching for partial-thickness foreign bodies or lacerations.
The most valuable examining tool is the slit lamp (Fig. 14–2).f
• With direct illumination, the object is viewed via light scattered from its anterior surface. Unfortunately, due to the complex optical nature of the cornea and the multiple interactive surfaces, clear foreign bodies (e.g., glass, plastic) and even lacerations may be difficult to appreciate.
• Under retroillumination, the object is illuminated from behind; the light can be reflected from the iris or the fundus, providing backlit relief of corneal lesions.
PEARL… Retroillumination can be very useful in detecting light transmission anomalies such as those caused by corneal lac-erations: light is scattered in the area of the laceration, which appears either highlighted or backlighted.
• Sclerotic scatter takes advantage of internal reflection. Light entering the cornea from the limbus is totally internally reflected from the epithelial and endothelial surfaces; any interruption in the light path results in anterior and posterior light scattering. This is very helpful in detecting corneal foreign bodies as well as structural abnormalities: interfaces between broken/cut stromal lamellae show up bright or dark.
Stains
Stains such as fluorescein and rose bengal provide additional help.
• Rose bengal is rapidly taken up by abnormal or damaged cells, making these red stained.
• Fluorescein rarely stains healthy cells, although the disruption of cell barriers or denudation of the epithelial basement membrane also results in fluorescein uptake. Fluorescein is able to show whether aqueous is leaking from a full-thickness wound (Seidel test; see Fig. 14—3 and Chapters 9 and 19). A cobalt blue filter enhances fluorescein detection.
PEARL… The cornea must be examined within seconds of fluorescein instillation as the dye rapidly diffuses into the tissue: 3 to 5 minutes after instillation, the area of uptake is blurred, the edges are diffuse, and the test’s value is significantly decreased.

FIGURE 14–3 Seidel’s test. Seidel’s testing utilizes the characteristic of fluorescein to quench fluorescence in high concentrations. In the photograph, the area of corneal injury was coated with a high concentration of fluorescein from a dampened strip. The aqueous leakage diluted the dye and allowed fluorescence to occur, thus indicating the presence of a full-thickness wound.
AbrasionEpidemiology
One of the most common globe injuries is corneal abrasion: 10% of new patient visits to an ophthalmic ER in one study were due to epithelial cell loss.7Corneal abrasion frequently accompanies deeper/ more extensive ocular trauma.
Pathophysiology
As discussed earlier, the corneal basal epithelial cells rest on a secreted basement membrane and are held in position by hemidesmosomal attachments. If the basal epithelial cells are removed from the basement membrane, corneal abrasion results. The abrasion can be partial or full thickness, and as long as Bowman’s layer is not disturbed, healing generally follows with-out scarring.
Healing of the abraded epithelium occurs in several stages:
1. initially, there is a migration of peripheral cells onto the area of denuded basement membrane;
2. this is followed by proliferation of the epithelial cells to restore epithelial thickness;
3. the process ends with the formation ofhemidesmosomal attachments to the underlying basement membrane.
It should be appreciated that corneal epithelial cells are in a constant state of reproduction, migration, and shedding. The source of restoration is felt to be the limbal stem cell located at the corneoscleral junction (see Chapter 11).8
Because of the density of the sensory nerve innervation of the corneal epithelial surface, corneal abrasions cause:
• intense pain (which is instantaneous); generally associated with significant
• photophobia, and
• lacrimation.
Patients with epithelial loss may have symptoms that appear to be out of proportion to the severity of the injury. Because of the overwhelming pain associated with corneal abrasion,g patients are able to tell the ophthalmologist the exact time and circumstance of the injury.
PEARL… An exception to the imme-diate occurrence of symptoms caused by epithelial damage is photokeratitis (e.g., a welder’s burn due to UV light-induced damage to the cornea), in which the symptoms typically follow the exposure by 6–12 hours.h
Examination
Examination of patients with corneal abrasion may be difficult because of the discomfort, lacrimation, and photophobia. A drop of topical anesthetic (e.g., proparacaine 0.5%) can be of great benefit, permitting proper evaluation.
• The first step is an overall inspection of the patient’s face for associated damage. This is followed by the examination of the cornea itself.
• A penlight is frequently helpful in detecting the irregular corneal light reflex, which may indicate the presence of an abrasion.
• Fluorescein staining makes epithelial denudation readily apparent (see Fig. 14—4).
• The underlying stroma must be examined carefully for deeper injury.
PITFALL
It is extremely important to rule out an occult open globe injury in the evaluation of patients with corneal abrasions.
In most cases of acute corneal abrasion, the underlying corneal stroma is clear, although white cell recruitment giving a granular appearance may occur 12–24 hours after epithelial absence. Stromal edema can be seen if the epithelial defect persists.
Management
The corneal epithelium represents the first line of defense against invading microorganisms; consequently, efforts should be directed at achieving corneal epithelial coverage as soon as possible. This is accomplished by:

FIGURE 14–4 Fluorescein staining of an epithelial defect. As discussed in the text, fluorescein diffuses rapidly into the stroma bordering an epithelial defect. For this reason, it is important to inspect the corneal immediately after fluorescein instillation.
• protecting the newly healing corneal epithelial surface from toxic insults (e.g., medications such as topical anesthetics) and
• sheltering the migrating cells.
PITFALL
Tight pressure patching of eyes with corneal abrasion was once a mainstay of therapy. It is now understood that this may be counterproductive to corneal healing by reducing the oxygen supply to the healing epithelium. Patching also increases the corneal temperature, increasing the risk of infection by facilitating microorganism replication in the preocular tear film under the patch.10 Treatment without patching (with concurrent use of antibiotics and cycloplegics) may result in faster healing than with patching.11
If necessary, the healing corneal epithelium can be protected with the use of a bandage soft contact lens.The contact lens offers distinct advantages:
• the lens acts as a patch to protect and cover the epithelium but
 does not prevent oxygen penetration or
does not prevent oxygen penetration or
 result in temperature elevation; in addition,
result in temperature elevation; in addition,
• the patient is able to see with the affected eye during the healing process.
PITFALL
Patient compliance is a significant issue during treatment for corneal abrasion. In one study, 40% of patients removed their patch because of discomfort.11 Soft contact lenses are generally beneficial but they may slow the healing process.12
Patient comfort can be significantly increased with the use of topical cycloplegics.
All medications, including topical antibiotics, are toxic.13,14,i An agent that does not interfere with epithelial healing has not been identified yet.
CONTROVERSY
The benefit of topical antibiotic agents in the treatment of routine corneal abrasions is questionable, given the drugs’ potential epithelial toxicity. Conversely, loss of the epithelial covering is a risk factor for infection.
The decision whether to use antibiotics is an individual one. Most clinicians utilize topical antibiotics to treat corneal abrasions; broad-spectrum coverage seems to have theoretical advantages. once the integrity of a healthy epithelial surface has been reestablished, there is no further need for topical antibiotics.
PITFALL
Under no circumstances should the patient be prescribed or given a topical anesthetic.Extended use of topical anesthetics results in corneal hyposensitivity and significantly interferes with corneal immunity.
Patients using topical anesthesia on an “ad hoc” basis generally present several days or weeks later with the classic appearance of a large epithelial defect overlying a white granular corneal opacity that is anesthetic, even though the lesion is intensely painful. Frequently these corneas become infected, which may be difficult to eradicate.
In most cases, corneal epithelial abrasions heal rapidly,j although large abrasions may take several days. The classic appearance of a healing abrasion is of advancing convex edges of epithelium, which eventually meet in an epithelial healing line.
PEARL… The healing line in corneal epithelial abrasions may be branching and appear very similar to a dendrite; for this reason, a history of epithelial abrasion is very helpful in differentiating this lesion from herpes simplex keratitis.
Fluorescein staining frequently reveals pooling of the dye in the thinned zone of the advancing epithelial edge for several days to a week after healing.
Recurrent Erosion
Although most corneal abrasions heal without sequelae, recurrent erosion occurs in 7 to 8% of eyes,15,16 presumably from abnormal adhesion complex formation in the base of epithelial defect. This results in delayed sloughing of the healed epithelial surface and is especially common if the trauma is caused by:
• fingernailk
• paper cut; or
• vegetable matter.
Diagnosis
The diagnosis is straightforward: the patient usually has a classic history.
PEARL… Typically, the patient with a recurrent erosion reports a sudden, very painful foreign body sensation with lacrimation and photophobia, which started immediately upon awakening in the morning.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


