Fig. 1
A transoral view of the oropharynx demonstrating the arrangement of the superficial muscles of the lateral oropharyngeal wall and tonsillar fossa as it would appear with a surgical retractor in place. The vascular and neural supply to this region is outlined. From Moore, EJ, et al. Transoral robotic surgery of the oropharynx: Clinical and anatomic considerations. Clinical Anatomy, 2012. Reprinted with permission [11]
The parapharyngeal space is a well-known potential space in the shape of an inverted pyramid extending from the skull base to the greater cornu of the hyoid bone [3, 5]. This space is bounded anteriorly by the pterygomandibular raphe on the lingual surface of the mandibular ramus; laterally by the deep lobe of the parotid, pterygoid muscles, and stylomandibular ligament; medially by the buccopharyngeal fascia; and posteriorly by the retropharyngeal space. The pre- and post-styloid compartments are divided by fascial condensations arising from the stylohyoid ligament, although this boundary varies by author. Pre-styloid contents include the deep lobe of the parotid and fat tissue whereas the post-styloid contents consist of neurovascular structures including the carotid sheath and sympathetic chain. Performance of TORS tonsillectomy does not routinely involve deep dissection of the parapharyngeal space. However, intimate knowledge of this space is a requisite for safe and effective TORS surgery as the internal carotid artery (ICA) and external carotid artery (ECA) branches are encountered, and in addition, displacement or effacement of the parapharyngeal fat is indicative of the extent and resectability of tonsillar tumors.
The stepwise surgical procedure of TORS radical tonsillectomy and the nuances thereof are have been previously described and are discussed elsewhere [6, 7]. However, further consideration of muscular and vascular anatomy can be appreciated in the context of the operation itself. Radical TORS tonsillectomy begins with a vertical incision through the pterygomandibular raphe. Dissection proceeds along the fascia of the medial pterygoid muscle and the surgeon enters the plane between the superior constrictor muscle and the buccopharyngeal fascia. The styloglossus and stylopharyngeus muscles are encountered and represent important anatomic landmarks in the procedure.
The styloglossus muscle arises from the inferior aspect of the styloid process and broadens as it descends, running deep to the medial pterygoid muscle before blending with the fibers of the intrinsic tongue muscles [3]. This muscle is located anterior and lateral to the stylopharyngeus and is encountered first. The stylopharyngeus originates from the medial aspect of the styloid process and courses medial and posterior to the styloglossus [3]. After running between the external and internal carotid arteries, the stylopharyngeus fans out and inserts into the pharynx between the superior and middle pharyngeal constrictors, spreading out between the middle constrictor and the pharyngobasilar fascia (Fig. 2). As noted previously, in instances where there is an anatomic dehiscence between the superior and middle pharyngeal constrictors, the stylopharyngeus will fill the space and form that portion of the tonsil bed. The styloglossus and stylopharyngeus muscles provide a key landmark as a sheath that separates the neurovascular structures of the parapharynx from the surgical bed and lumen of the oropharynx (Fig. 3). The neurovascular structures are lateral and inferior to the plane of the styloglossus, and thus the styloglossus often represents the deep boundary of dissection. Although they are carefully transected during performance of radical tonsillectomy, and in some cases are resected for oncologic purposes, structures medial to these muscles must be respected.
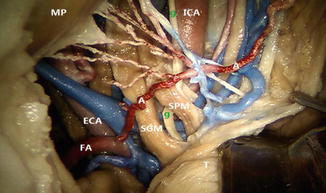
Fig. 2
External view of the musculature of the lateral oropharyngeal area and styloid apparatus. Note the course of the stylopharyngeus muscles as it starts lateral to the internal carotid artery at the level of the styloid, but at its insertion at the level of the oropharynx, lies medial to both the internal and external carotid arteries. From Tubbs RS, et al. Compression of the cervical internal carotid artery by the stylopharyngeus mucle. J Neurosurg. 2010. Reprinted with permission [8]
Fig. 3
Transoral view of the parapharyngeal space contents after removal of the superior constrictor muscle in a cadaveric dissection. Note the styloglossus and stylopharyngeus slings protecting the lateral contents including the major cervical vessels. In this anatomic variant, the ascending pharyngeal is seen arising from the facial artery rather than directly from the external carotid artery. A ascending pharyngeal artery, MP medial pterygoid muscle, ICA internal carotid artery, ECA external carotid artery, FA facial artery, SGM styloglossus muscle, SPM stylopharyngeus muscle, g glossopharyngeal nerve, T tongue. From Wang, C, et al. A description of arterial variants in the transoral approach to the parapharyngeal space. Clinical Anatomy. 2014. Reprinted with permission [9]
The lingual nerve may be encountered if dissection is continued inferiorly and anteriorly at this location (Fig. 4). This main branch of V3 is joined by the chorda tympani at the level of the posterior border of the medial pterygoid muscle and provides general sensation and taste to the anterior two-thirds of the tongue as well as parasympathetic innervation to the submandibular and sublingual salivary glands. The nerve courses anteriorly and inferiorly between the lingual surface of the mandible and the lateral surface of the medial pterygoid. At the anterior aspect of the medial pterygoid, the lingual nerve runs lateral to the superior constrictor muscle and thus may be near the field of dissection. Dissection of the nerve itself is usually not necessary in routine radical tonsillectomy, buts its location in this region should be noted to avoid injury.
Fig. 4
A schematic drawing and correlating cadaver dissection depicting an anterior–posterior view of the dissected lateral pharyngeal wall. APA ascending pharyngeal artery, ApaA ascending palatine artery, IJV internal jugular vein, LN lingual nerve, M mandible, MPM medial pterygoid muscle, SCM superior constrictor muscle, SGM styloglossus muscle, SMG submandibular gland, SP soft palate, SPM stylopharyngeus muscle, TB tongue base, IXcn glossopharyngeus nerve, XIIcn hypoglossal nerve. From Dallan, I, et al. Transoral endoscopic anatomy of the parapharyngeal space: A step-by-step logical approach with surgical considerations. Head and Neck. 2010. Reprinted with permission [5]
The second important nervous structure to consider in TORS tonsillectomy is the glossopharyngeal nerve (CN IX). This nerve is responsible for providing sensation in the oropharynx, motor innervation to the stylopharyngeus, and autonomic innervation to the parotid gland and carotid body. After exiting the skull base via the jugular foramen, CN IX runs inferiorly, coursing medial to the styloid process between the stylopharyngeus and styloglossus muscles, laying on the lateral aspect of the stylopharyngues. As it courses toward the middle constrictor muscle, it sends terminal branches to the tonsil and posterior one-third of the tongue. The main trunk of the nerve may be very close to the tonsil fossa especially if there is dehiscence between the middle and superior pharyngeal constrictors. Transection of the lingual and tonsillar branches of CN IX occurs during the course of a TORS extirpation. This, as well as potential damage to the main nerve itself, is likely responsible for postoperative dysgeusia noted in patients undergoing routine tonsillectomy as well as TORS operations [10].
As dissection continues medial to the parapharyngeal fat, the surgeon will encounter and must control the arterial supply to the surgical field. Vascular supply to the tonsil and lateral pharyngeal wall is based on the branches of the ECA [11]. The blood supply to the tonsil includes the ascending palatine and tonsillar branches of the facial artery, the ascending pharyngeal artery, and branches from the lingual artery, ascending palatine artery, and internal maxillary artery. During routine tonsillectomy, these branches are easily controlled with cautery. However, dissection deep to the superior constrictor muscles during radical tonsillectomy encounters blood vessels of a higher caliber that may require ligation with surgical clips to avoid hemorrhage. In addition, several variations and aberrant courses of these vessels will be discussed.
The dominant arterial supply to the tonsil is the tonsillar branch of the facial artery. The facial artery, along with the lingual and ascending pharyngeal arteries, lies approximately 5- to 8-mm deep to the styloglossus muscle [12]. The tonsillar branch has a variable course and can run between, anterior, or posterior to the styloglossus and stylopharyngeus muscles. Application of surgical clips facilitates control of this dominant branch. Another consideration related to the facial artery relates to the main trunk of the vessel. After originating from the ECA in the neck, the artery courses superiorly before turning anteriorly to supply the submandibular gland and face. Tumors with anterior and inferior extension can approximate the artery at either the horizontal portion or the anterior turn, and troublesome bleeding may be encountered [13].
The pharyngeal venous plexus is encountered inferomedially when dissecting lateral to the superior constrictor muscle. These venous branches are encountered medial to the branches of the external carotid artery (ECA) within the space between the stylopharyngeus and the superior constrictor muscle [5, 12]. Terminal drainage of this plexus is to the internal jugular vein. The vessels of this plexus are highly variable in their course and redundancy and can often be controlled readily with monopolar or bipolar electrocautery.
Thus, hemostasis is readily achieved in TORS radical tonsillectomy with knowledge and anticipation and control of the known arterial supply. Further, several maneuvers have been described in order to protect the patient from vascular injury and hemorrhage encountered during TORS radical tonsillectomy. This includes, for example, ligation of the lingual artery or placement of cotton patties medial to the carotid sheath to protect the sheath contents via a cervical approach, prior to the TORS procedure [7, 11]. Whether or not such methods are used, intimate knowledge of the vasculature and anatomic variations is needed to avoid complications. In addition, advanced TORS approaches are currently under investigation including dissection of the parapharyngeal space and infratemporal fossa which require knowledge of vascular aberrations.
The ascending palatine artery contributes to the blood supply of the tonsil and lateral pharyngeal wall. This artery branches from the facial artery and crosses the styloglossus muscle prior to entering the prestyloid parapharyngeal space. In one described variant, the ascending palatine courses between the styloglossus and stylopharyngeus [9]. If encountered, this artery can be controlled with clips or cautery. The ascending pharyngeal artery is a more robust artery providing blood supply to the same region. This originates from the medial surface of the ECA near the carotid bifurcation, but has been known to originate from the ICA or the occipital artery [9]. The artery ascends vertically lateral to the pharyngeal wall towards the skull base. A mean distance of between 5- and 8-mm was noted between the ascending pharyngeal artery, as well as other ECA branches, and the styloglossus muscle [12]. Control of this artery with appropriate clipping from a transoral approach or ligation from a cervical approach is critical.
The ECA has a fairly consistent relationship with the lateral pharyngeal wall. When measured at the C2–C3 vertebral interspace, the ECA lies approximately 1.8 cm lateral to the lateral pharyngeal wall [12]. This distance may of course be altered by the mass effect of tumor and should be noted preoperatively. In cadaveric studies, Wang and colleagues noted the presence of an aberrant ECA in a minority of specimens [9]. In 92 % of cases, the ECA ran deep to and was protected by the styloglossus muscle. Thus, the main trunk of ECA was exposed to injury when dissection proceeded deep to the styloglossus and stylopharyngeus muscle slings. However, in the remaining 8 %, the ECA perforates a dehiscence in the fascial plane between the styloglossus and stylopharyngeus, and thus lies in close relationship to the constrictor musculature (Fig. 5). This creates a situation of potential injury during TORS radical tonsillectomy as well as parapharyngeal space dissection (Fig. 5). In addition, as seen in cadaveric dissection, completion of TORS radical tonsillectomy in a patient with this variation may leave the ECA exposed through the pharyngeal defect and require reconstruction for coverage.
Fig. 5
Depicted in the left column is the normal arrangement of the external carotid artery in relation to the stylopharyngeus and styloglossus muscles. In the right column, the external carotid is coursing medially through a dehiscence between the two muscle bellies. S styloid process, g glossopharyngeal nerve, I internal carotid artery, ECA external carotid artery, SGM styloglossus muscle, SPM stylopharyngeus muscle, P medial pterygoid muscle, U uvula, IJV internal jugular vein, D digastric muscle. From Wang, C, et al. A description of arterial variants in the transoral approach to the parapharyngeal space. Clinical Anatomy. 2014. Reprinted with permission [9]
A potentially catastrophic complication of TORS radical tonsillectomy may be ICA injury and this should be avoided at all costs. The cervical ICA normally runs vertically through the neck to the skull base without branching. As one reaches adulthood, the distance between the ICA and the tonsillar fossa approaches 25 mm [14]. Thus, dissection lateral to the constrictor muscle, especially in a blunt manner, can be performed safely under normal circumstances. The styloglossus and styloparyngeus muscles serve as landmarks for the location and therefore protection of the ICA. Although the styloglossus originates lateral to the ICA, it courses medially and, along with the stylopharyngeus, is medial to the ICA at the level of the oropharynx. Thus, transection of these muscles can be performed, if needed, in the presence of a known parapharyngeal fat pad that can be bluntly dissected away to protect the ICA.
However, between 10 and 40 % of the general population may have some aberration of the cervical ICA that alters this course and relation to the oropharynx [15]. Tortuosity, kinking, or coiling of the ICA must be assessed with preoperative imaging. These variants are associated with decreased distance between the ICA and tonsil fossa as well as loss of integrity in the tunica media and adventitia [16]. In addition, the presence of a submucosal or retropharyngeal carotid artery must be ruled out. This is a contraindication to TORS radical tonsillectomy due to a high risk of catastrophic vascular injury.
The remaining steps of TORS radical tonsil resection include a soft palate incision, and floor of mouth and base of tongue resection depending on the extent of the tumor, as well as an incision through the superior constrictor muscle and overlying mucosa posteriorly. At the completion of the procedure, the wound bed is comprised of the buccopharyngeal fascia and the styloglossus and stylopharyngeus muscles. Thus, care is taken to preserve the buccopharyngeal fascia if possible while the lateral surface of the constrictor muscle is dissected away during the surgery. The presence of these structures prevents communication into the neck via the parapharyngeal space and protects the carotid vasculature from exposure into the neck. If this barrier is excised for oncologic purposes, reconstruction can be performed for protection of the parapharyngeal contents, such as suturing of the fascial edges or use of a mucosal advancement flap for coverage of the defect [7].
Lymphatic drainage of the tonsillar region involves levels IIa, IIb, III, and IV of the neck as well as the retropharyngeal nodes. Classically defined by Rouviere and described in modern literature, the retropharyngeal nodes are divided into the poorly defined medial nodes that are often absent in adults, and the lateral nodes which are more pertinent to tumors of the oropharynx [13, 17]. Although there is generally one lateral retropharyngeal node on each side, up to three may be present. The location of the lateral nodes is fairly consistent and is anterior to the prevertebral fascia at the level of C1 and medial to the ICA and cervical sympathetic chain. The surgical resection of the lateral retropharyngeal nodes via the TORS approach has been described, and is performed after completion of robotic oropharyngectomy [18].
Although the data continue to evolve, it does not appear that lateral retropharyngeal nodal resection is universally required in tonsillar squamous cell carcinoma. Data have shown that when patients with early stage disease (T1 or T2 and N0-N2a) and no retropharyngeal involvement on preoperative imaging undergo routine retropharyngeal dissection, the rates of histologically confirmed metastasis are zero [17]. High quality multi-modality imaging is required for this purpose: either fine-cut computed tomography or magnetic resonance imaging combined with positron emission tomography. Thus surgery of the pharynx and tonsil alone may be sufficient in the appropriate patient.
Base of Tongue
The tongue is divided by the circumvallate papilla into two major units, the base of tongue and the oral tongue. The dorsal and posterior aspect of the tongue base comprises the anterior wall of the oropharynx. Like the lateral oropharyngeal wall, transoral robotic surgery greatly facilitates surgical access to the tongue base. Successful robotic surgery of the tongue base, as with other regions, is contingent on knowledge of the neurovascular anatomy. Preservation of at least one tongue base neurovascular bundle is necessary for survival and function of the remaining tongue.
Posterior to the tongue base lies the epiglottis. A median and two lateral glossoepiglottic folds connect these two structures. The valleculae represent the depression between the median and lateral folds. Even further laterally are the glossotonsillar folds, created by the palatoglossus muscle, which are continuous with the palatoglossal arch that runs anterior to the palatine tonsils.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


