Staphylococcal infection, acne rosacea, seborrheic dermatitis
Symptoms
 Burning, itching, discomfort, foreign-body sensation, tearing, crusting, mild discharge, fluctuation in vision
Burning, itching, discomfort, foreign-body sensation, tearing, crusting, mild discharge, fluctuation in vision
Signs
 Associated atopic and seborrheic dermatitis, and ocular rosacea
Associated atopic and seborrheic dermatitis, and ocular rosacea
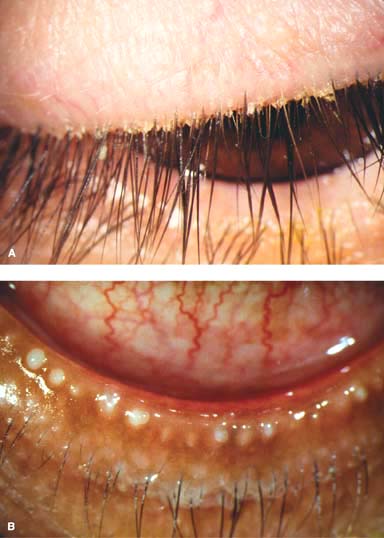
 Hyperemia, telangiectasias, crusting, scaling, formation of collarettes around bases of lashes (staphylococcal), sleeves along eyelashes (seborrheic), and pouting of meibomian gland orifices, which can be expressed to produce a thickened lipid secretion, sometimes of toothpaste-like consistency (Fig. 1-1)
Hyperemia, telangiectasias, crusting, scaling, formation of collarettes around bases of lashes (staphylococcal), sleeves along eyelashes (seborrheic), and pouting of meibomian gland orifices, which can be expressed to produce a thickened lipid secretion, sometimes of toothpaste-like consistency (Fig. 1-1)
 Frothy and foamy tear film, conjunctival injection, inferior superficial punctate keratopathy, phlyctenulosis, corneal infiltrates
Frothy and foamy tear film, conjunctival injection, inferior superficial punctate keratopathy, phlyctenulosis, corneal infiltrates
Treatment
 Warm compresses 5 to 10 minutes b.i.d., eyelid margin scrubs with mild commercially available cleansers (e.g., Ocusoft Lid Scrub, Advanced Vision Research Sterilid)
Warm compresses 5 to 10 minutes b.i.d., eyelid margin scrubs with mild commercially available cleansers (e.g., Ocusoft Lid Scrub, Advanced Vision Research Sterilid)
 Tear supplements while awake, topical azithromycin drops or erythromycin, bacitracin, or tetracycline ointment at bedtime
Tear supplements while awake, topical azithromycin drops or erythromycin, bacitracin, or tetracycline ointment at bedtime
 Oral tetracycline 250 mg b.i.d. to q.i.d. or doxycycline 100 mg q.d. to b.i.d. in severe or recurrent cases. These medications can often be tapered to a much lower dose for long-term use (e.g., doxycycline 20 mg b.i.d. or 50 mg q.d.). Oral erythromycin (approximately 200 mg/day) can be used for children.
Oral tetracycline 250 mg b.i.d. to q.i.d. or doxycycline 100 mg q.d. to b.i.d. in severe or recurrent cases. These medications can often be tapered to a much lower dose for long-term use (e.g., doxycycline 20 mg b.i.d. or 50 mg q.d.). Oral erythromycin (approximately 200 mg/day) can be used for children.
Judicious short-term use of topical corticosteroids for phlyctenulosis or infiltrates
Prognosis
 Good for significant improvement in symptoms over weeks, but patients need to understand that the condition is controlled rather than cured.
Good for significant improvement in symptoms over weeks, but patients need to understand that the condition is controlled rather than cured.
Figure 1-1. A. Blepharitis. Significant crusting at the base of the eyelashes is seen. A few collarettes are present. B. Meibomitis. Severe pouting of the meibomian glands of the inferior eyelid can be seen. The eyelid margin is thickened and inflamed, with some conjunctival injection visible.
CHALAZION (INTERNAL HORDEOLUM, STYE)
A chalazion is a tender eyelid mass, often with surrounding erythema and swelling. It may be small or large, and can cause significant eyelid inflammation when severe.
Etiology
 Blockage of meibomian gland orifices and stagnation of sebaceous secretions
Blockage of meibomian gland orifices and stagnation of sebaceous secretions
 Associated with blepharitis/meibomitis and acne rosacea
Associated with blepharitis/meibomitis and acne rosacea
Symptoms
 Eyelid swelling, pain, and redness
Eyelid swelling, pain, and redness
 Often a history of previous chalazia
Often a history of previous chalazia
 Rarely, large, central chalazia can cause corneal flattening, especially after refractive surgery, or induced astigmatism.
Rarely, large, central chalazia can cause corneal flattening, especially after refractive surgery, or induced astigmatism.
Signs
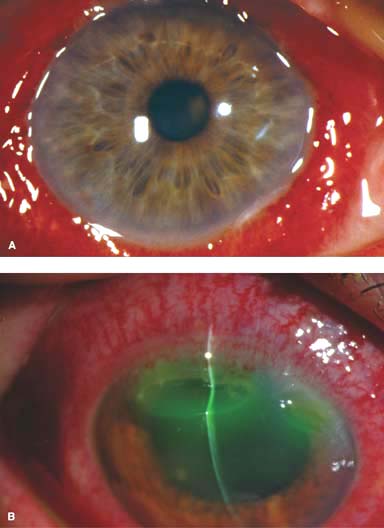
 Subcutaneous round, firm, swelling in the tarsal plate (Fig. 1-2)
Subcutaneous round, firm, swelling in the tarsal plate (Fig. 1-2)
 May have an associated pyogenic granuloma on eversion of eyelid
May have an associated pyogenic granuloma on eversion of eyelid
 Sometimes may be associated with significant eyelid inflammation (preseptal cellulitis)
Sometimes may be associated with significant eyelid inflammation (preseptal cellulitis)
Differential Diagnosis
 External hordeolum: an acute staphylococcal infection of a lash follicle and its associated gland of Zeis or Moll
External hordeolum: an acute staphylococcal infection of a lash follicle and its associated gland of Zeis or Moll
 Pyogenic granuloma: a vascularized mass protruding from the conjunctiva
Pyogenic granuloma: a vascularized mass protruding from the conjunctiva
 Sebaceous carcinoma: suspect in recurrent chalazia, eyelid margin excoriation, or loss of lashes, especially if unilateral
Sebaceous carcinoma: suspect in recurrent chalazia, eyelid margin excoriation, or loss of lashes, especially if unilateral
Diagnosis
 Eyelid biopsy if suspicious for sebaceous carcinoma
Eyelid biopsy if suspicious for sebaceous carcinoma
Treatment
 Warm compresses, eyelid massage, and hygiene (see Blepharitis/Meibomitis above)
Warm compresses, eyelid massage, and hygiene (see Blepharitis/Meibomitis above)
 Topical azithromycin drops or erythromycin, bacitracin, or tetracycline ointment for blepharitis/meibomitis
Topical azithromycin drops or erythromycin, bacitracin, or tetracycline ointment for blepharitis/meibomitis
 Oral tetracycline 250 mg b.i.d. to q.i.d. or doxycycline 100 mg q.d. to b.i.d. in inflamed, severe, or recurrent cases, to prevent recurrent chalazia
Oral tetracycline 250 mg b.i.d. to q.i.d. or doxycycline 100 mg q.d. to b.i.d. in inflamed, severe, or recurrent cases, to prevent recurrent chalazia
 Corticosteroid injection can be considered to reduce scarring in recalcitrant cases.
Corticosteroid injection can be considered to reduce scarring in recalcitrant cases.
 Incision and curettage if no improvement with medical treatment.
Incision and curettage if no improvement with medical treatment.
Prognosis
 Very good with medical treatment
Very good with medical treatment
 If medical treatment is unsuccessful, surgical treatment is quite effective.
If medical treatment is unsuccessful, surgical treatment is quite effective.
Figure 1-2. Chalazion. A. A large, inflamed chalazion of the upper eyelid. Severe blepharitis and crusting of the eyelid margin, predisposing factors for development of chalazia, are also present. B. Lower-eyelid eversion reveals a large indurated mass consistent with a chalazion.

BACTERIAL CONJUNCTIVITIS (NONGONOCOCCAL)
Bacterial conjunctivitis is a relatively uncommon, usually bilateral condition, characterized by a mucopurulent or purulent discharge.
Etiology
 Staphylococcus aureus, Staphylococcus epidermidis
Staphylococcus aureus, Staphylococcus epidermidis
 Streptococcus pneumoniae
Streptococcus pneumoniae
 Haemophilus influenzae (especially in children), others
Haemophilus influenzae (especially in children), others
Symptoms
 Redness, discharge, foreign-body sensation, burning, itchiness, photophobia
Redness, discharge, foreign-body sensation, burning, itchiness, photophobia
Signs
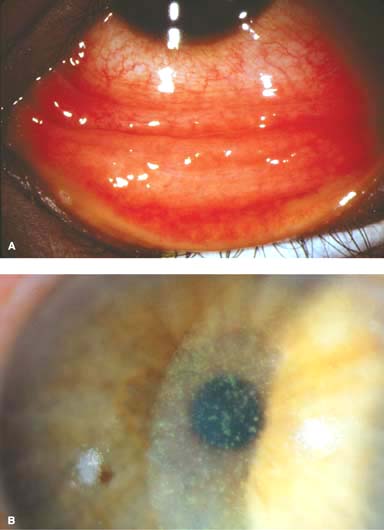
 Purulent or mucopurulent discharge (Fig. 1-3)
Purulent or mucopurulent discharge (Fig. 1-3)
 Conjunctival hyperemia, maximal in the fornices
Conjunctival hyperemia, maximal in the fornices
 Pseudomembranes may be present in severe infections.
Pseudomembranes may be present in severe infections.
 Corneal punctate epitheliopathy
Corneal punctate epitheliopathy
 Preauricular lymphadenopathy is usually absent.
Preauricular lymphadenopathy is usually absent.
Diagnostic Evaluation
 Conjunctival swab for Gram stain, cultures, and sensitivities if severe or recurrent
Conjunctival swab for Gram stain, cultures, and sensitivities if severe or recurrent
Treatment
 Spontaneous resolution in days to 1 to 2 weeks is usual.
Spontaneous resolution in days to 1 to 2 weeks is usual.
 Artificial tears to wash away discharge
Artificial tears to wash away discharge
 Empiric broad-spectrum topical antibiotic drops (e.g., polymyxin B/trimethoprim, fluoroquinolones, gentamicin, tobramycin, neomycin/gramicidin/bacitracin) q.i.d. for 1 week or azithromycin b.i.d. for 2 days then q.d. for 5 days
Empiric broad-spectrum topical antibiotic drops (e.g., polymyxin B/trimethoprim, fluoroquinolones, gentamicin, tobramycin, neomycin/gramicidin/bacitracin) q.i.d. for 1 week or azithromycin b.i.d. for 2 days then q.d. for 5 days
 Antibiotic ointments (e.g., ciprofloxacin, tobramycin, gentamicin, tetracycline, bacitracin, polymyxin B/bacitracin) can be used q.i.d. for 1 week in patients in whom the drops wash out very quickly, such as crying children.
Antibiotic ointments (e.g., ciprofloxacin, tobramycin, gentamicin, tetracycline, bacitracin, polymyxin B/bacitracin) can be used q.i.d. for 1 week in patients in whom the drops wash out very quickly, such as crying children.
Prognosis
 Very good
Very good
 Severe infections can cause permanent conjunctival scarring.
Severe infections can cause permanent conjunctival scarring.
Figure 1-3. Bacterial conjunctivitis. A. Diffuse conjunctival injection and a purulent discharge are present in this eye with bacterial conjunctivitis. B. A severe purulent discharge with crusting can be seen in this patient who has bacterial conjunctivitis. There is also moderate conjunctival injection.
GONOCOCCAL BACTERIAL CONJUNCTIVITIS
Gonococcal conjunctivitis is a rare, occasionally bilateral condition, characterized by acute onset of a severe purulent discharge.
Etiology
 Primarily Neisseria gonorrhoeae
Primarily Neisseria gonorrhoeae
 Occasionally Neisseria meningitidis
Occasionally Neisseria meningitidis
 It is typically sexually transmitted.
It is typically sexually transmitted.
Symptoms
 Redness, severe purulent discharge, foreign-body sensation, burning, photophobia
Redness, severe purulent discharge, foreign-body sensation, burning, photophobia
 Hyperacute onset (within 12 to 24 hours)
Hyperacute onset (within 12 to 24 hours)
Signs
 Severe purulent discharge; pseudomembranes may be present
Severe purulent discharge; pseudomembranes may be present
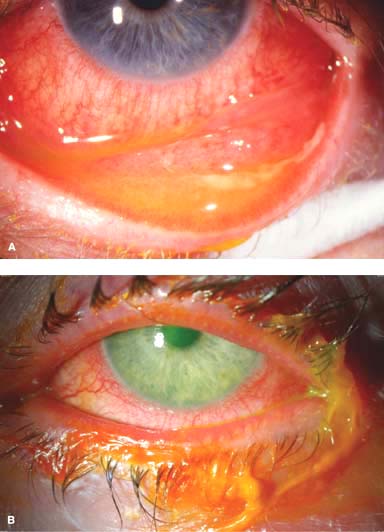
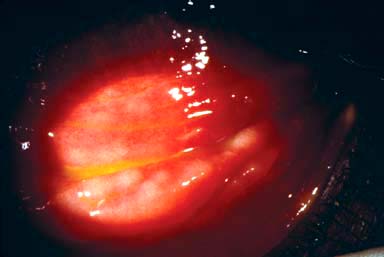
 Marked conjunctival inflammation and chemosis (Fig. 1-4A)
Marked conjunctival inflammation and chemosis (Fig. 1-4A)
 Eyelid swelling
Eyelid swelling
 Preauricular lymphadenopathy often present
Preauricular lymphadenopathy often present
 Corneal punctate epitheliopathy, epithelial defect, infiltrate, ulcer, or perforation (Fig. 1-4B)
Corneal punctate epitheliopathy, epithelial defect, infiltrate, ulcer, or perforation (Fig. 1-4B)
Diagnostic Evaluation
 Conjunctival scraping for immediate Gram stain, cultures, and sensitivities. The diagnosis is confirmed if the Gram stain demonstrates gram-negative intracellular diplococci.
Conjunctival scraping for immediate Gram stain, cultures, and sensitivities. The diagnosis is confirmed if the Gram stain demonstrates gram-negative intracellular diplococci.
Treatment
 Systemic ceftriaxone 1 g IM in a single dose if there is no corneal involvement. If the patient is allergic to cephalosporins, fluoroquinolones are the drugs of choice.
Systemic ceftriaxone 1 g IM in a single dose if there is no corneal involvement. If the patient is allergic to cephalosporins, fluoroquinolones are the drugs of choice.
 If there is corneal involvement or corneal involvement cannot be excluded because of a limited slit-lamp examination, the patient should be treated with ceftriaxone 1 g IV q12h to q24h for 3 days.
If there is corneal involvement or corneal involvement cannot be excluded because of a limited slit-lamp examination, the patient should be treated with ceftriaxone 1 g IV q12h to q24h for 3 days.
 Topical fluoroquinolone (e.g., ciprofloxacin) drops q2h, or q1h if the cornea is involved.
Topical fluoroquinolone (e.g., ciprofloxacin) drops q2h, or q1h if the cornea is involved.
 Ocular irrigation with saline q.i.d. to q2h to eliminate the discharge.
Ocular irrigation with saline q.i.d. to q2h to eliminate the discharge.
 Evaluate and treat for possible coinfection with Chlamydia (e.g., azithromycin 1 g PO once).
Evaluate and treat for possible coinfection with Chlamydia (e.g., azithromycin 1 g PO once).
 Evaluate sexual partners for sexually transmitted infections.
Evaluate sexual partners for sexually transmitted infections.
Prognosis
 Very good if diagnosed and treated appropriately before corneal involvement occurs. If the cornea is involved, the prognosis is guarded.
Very good if diagnosed and treated appropriately before corneal involvement occurs. If the cornea is involved, the prognosis is guarded.
Figure 1-4. Gonococcal conjunctivitis. A. Severe inflammation and chemosis are present throughout the conjunctiva in this right eye. Some purulent discharge is present on the eyelid and conjunctiva nasally. The cornea is not involved. B. A large corneal ulcer with significant tissue loss is found in the superior cornea; it is critical to examine the entire cornea in eyes with gonococcal conjunctivitis to determine whether there is corneal involvement.
VIRAL CONJUNCTIVITIS (TYPICALLY ADENOVIRUS)
Viral conjunctivitis is a common, highly contagious, usually bilateral condition, characterized by the rapid onset of redness, itchiness, and tearing, first in one eye and then the other.
Etiology
 Adenovirus serotypes 8, 19, 37: epidemic keratoconjunctivitis
Adenovirus serotypes 8, 19, 37: epidemic keratoconjunctivitis
 Adenovirus serotypes 3, 7: pharyngoconjunctival fever, usually in children
Adenovirus serotypes 3, 7: pharyngoconjunctival fever, usually in children
 Others: herpes simplex virus, enteroviruses, Newcastle disease virus, Epstein-Barr virus
Others: herpes simplex virus, enteroviruses, Newcastle disease virus, Epstein-Barr virus
Symptoms
 Tearing, itching, burning, redness, foreign-body sensation, photophobia
Tearing, itching, burning, redness, foreign-body sensation, photophobia
 History of contact with someone with a red eye, recent upper respiratory tract infection, or recent eye examination
History of contact with someone with a red eye, recent upper respiratory tract infection, or recent eye examination
Signs
 Eyelid edema
Eyelid edema
 Watery discharge
Watery discharge
 Generalized conjunctival hyperemia, subconjunctival hemorrhages
Generalized conjunctival hyperemia, subconjunctival hemorrhages
 Conjunctival follicles, which are frequently most apparent in the inferior fornices (Fig. 1-5A)
Conjunctival follicles, which are frequently most apparent in the inferior fornices (Fig. 1-5A)
 Membranes or pseudomembranes in severe cases
Membranes or pseudomembranes in severe cases
 Conjunctival membranes consist of coagulated exudate adherent to inflamed conjunctival epithelium. Clinically, a true membrane causes bleeding on attempted removal and a pseudomembrane does not, but this rule is not universal. The causes of true membranes and pseudomembranes are similar.
Conjunctival membranes consist of coagulated exudate adherent to inflamed conjunctival epithelium. Clinically, a true membrane causes bleeding on attempted removal and a pseudomembrane does not, but this rule is not universal. The causes of true membranes and pseudomembranes are similar.
 Central punctate epithelial keratitis, and occasionally an epithelial defect (Fig. 1-5B).
Central punctate epithelial keratitis, and occasionally an epithelial defect (Fig. 1-5B).
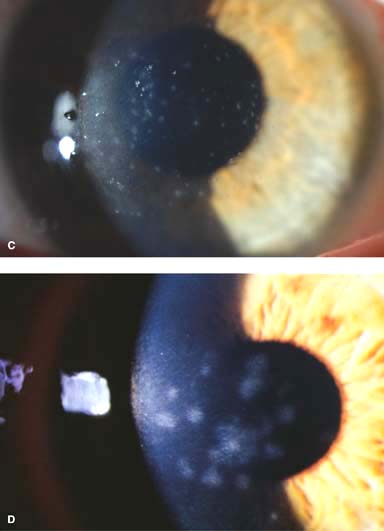
 Multiple small corneal infiltrates with overlying punctate staining may also be seen in the acute phase of severe infections (Fig. 1-5C).
Multiple small corneal infiltrates with overlying punctate staining may also be seen in the acute phase of severe infections (Fig. 1-5C).
 Preauricular lymphadenopathy is often present.
Preauricular lymphadenopathy is often present.
 Subepithelial infiltrates (SEIs) can occur weeks after the onset of the acute infection and may persist for months to years (Fig. 1-5D)
Subepithelial infiltrates (SEIs) can occur weeks after the onset of the acute infection and may persist for months to years (Fig. 1-5D)
Treatment
 Artificial tears and cool compresses four to eight times a day
Artificial tears and cool compresses four to eight times a day
 Antihistamines (e.g., antazoline, naphazoline) q.i.d. for itching
Antihistamines (e.g., antazoline, naphazoline) q.i.d. for itching
 Removal of membranes or pseudomembranes
Removal of membranes or pseudomembranes
 Corticosteroid drops in severe cases with membranes or pseudomembranes or erosions. A long, slow taper of mild corticosteroid drops can be used in eyes with SEIs that affect visual function.
Corticosteroid drops in severe cases with membranes or pseudomembranes or erosions. A long, slow taper of mild corticosteroid drops can be used in eyes with SEIs that affect visual function.
 Strict observation of hygienic measures is needed to avoid spreading the infection.
Strict observation of hygienic measures is needed to avoid spreading the infection.
Prognosis
 Very good. If clinically significant subepithelial infiltrates develop, the treatment course can be prolonged. Severe infections with membranes or pseudomembranes can cause permanent conjunctival scarring (Fig. 1-5E).
Very good. If clinically significant subepithelial infiltrates develop, the treatment course can be prolonged. Severe infections with membranes or pseudomembranes can cause permanent conjunctival scarring (Fig. 1-5E).
Figure 1-5. Viral conjunctivitis. A. Diffuse conjunctival injection with a severe follicular reaction, greatest inferiorly, is present in this eye with viral conjunctivitis. B. A central punctate epithelial keratitis as seen in this eye is often found early in the course of viral conjunctivitis, most commonly caused by adenovirus. Viral conjunctivitis. C. In the acute phase, small superfi\cial corneal infiltrates with overlying punctate staining can develop. Note the irregular light reflex. D. Multiple subepithelial infiltrates (SEIs) of the cornea can be seen 2 months after resolution of adenoviral keratoconjunctivitis. These SEIs tend to resolve on their own. If they are severe, they can affect visual acuity and cause glare symptoms. SEIs generally respond to low-dose topical corticosteroid drops; however, if they are started, these drops need to be tapered very slowly, over months. Viral conjunctivitis. E. Inferior conjunctival scarring is seen in this eye several months after adenoviral conjunctivitis.

CHLAMYDIAL CONJUNCTIVITIS (ADULT INCLUSION CONJUNCTIVITIS)
Adult chlamydial conjunctivitis is a relatively common, usually unilateral condition that is typically transmitted sexually and generally affects young adults.
Etiology
 Chlamydia trachomatis serotypes D through K
Chlamydia trachomatis serotypes D through K
 Typically sexually transmitted
Typically sexually transmitted
Symptoms
 Tearing, itching, burning, redness, foreign-body sensation, photophobia, discharge of longer than 3 to 4 weeks in duration
Tearing, itching, burning, redness, foreign-body sensation, photophobia, discharge of longer than 3 to 4 weeks in duration
 May be associated with urethritis, vaginitis, or cervicitis
May be associated with urethritis, vaginitis, or cervicitis
Signs
 Stringy, white mucopurulent discharge
Stringy, white mucopurulent discharge
 Large follicles in the inferior fornices (Fig. 1-6)
Large follicles in the inferior fornices (Fig. 1-6)
 Superior tarsal follicles, occasionally follicles at the limbus
Superior tarsal follicles, occasionally follicles at the limbus
 Superior limbal or peripheral nummular corneal infiltrates and pannus
Superior limbal or peripheral nummular corneal infiltrates and pannus
 Mild preauricular lymphadenopathy may be present.
Mild preauricular lymphadenopathy may be present.
Diagnosis
 History of sexual exposure; patient may have concomitant genitourinary symptoms
History of sexual exposure; patient may have concomitant genitourinary symptoms
 Direct immunofluorescent antibody test of conjunctival smears
Direct immunofluorescent antibody test of conjunctival smears
 Giemsa stain cytology for basophilic cytoplasmic inclusion bodies of Halberstaedter-Prowazek; more common in newborns than adults
Giemsa stain cytology for basophilic cytoplasmic inclusion bodies of Halberstaedter-Prowazek; more common in newborns than adults
 McCoy chlamydial cell culture
McCoy chlamydial cell culture
Treatment
 Azithromycin 1 g PO once, doxycycline 100 mg PO b.i.d., or tetracycline, erythromycin or clarithromycin 250 mg q.i.d. for 2 to 6 weeks
Azithromycin 1 g PO once, doxycycline 100 mg PO b.i.d., or tetracycline, erythromycin or clarithromycin 250 mg q.i.d. for 2 to 6 weeks
 Topical azithromycin drops b.i.d. for 2 days, then q.i.d. for 1 to 6 weeks, or tetracycline or erythromycin ointment q.i.d. for 4 to 6 weeks
Topical azithromycin drops b.i.d. for 2 days, then q.i.d. for 1 to 6 weeks, or tetracycline or erythromycin ointment q.i.d. for 4 to 6 weeks
 Referral for treatment of sexual partners and other sexually transmitted infections should be done.
Referral for treatment of sexual partners and other sexually transmitted infections should be done.
Prognosis
 Very good
Very good
FIGURE 1-6. Chlamydial conjunctivitis. A severe inferior conjunctival follicular reaction can be seen in this eye with chronic chlamydial conjunctivitis. There were similar conjunctival follicles superiorly. There is also diff use bulbar conjunctival injection.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


