Congenital Malformations of the Ear
Congenital malformations of the auricle, external ear canal, tympanic membrane, middle ear cleft, and ossicles may occur as isolated entities or in association with other deformities.
4-1 Preauricular Tags
Introduction
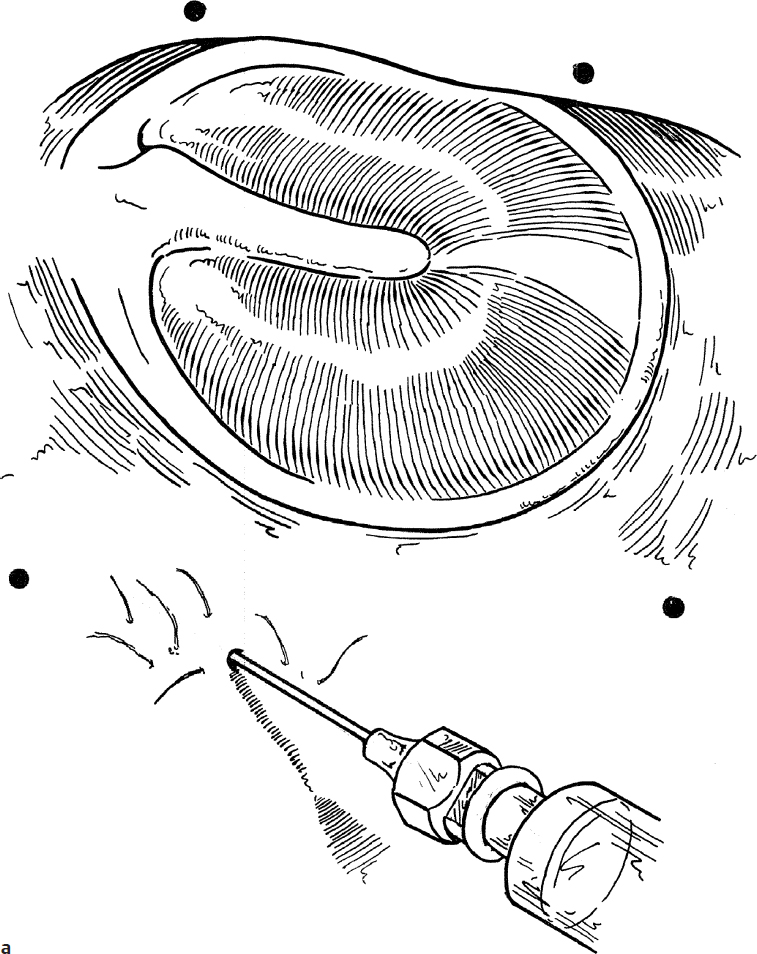
Preauricular tags are congenital malformations associated with incomplete migration and/or coalescence of the auricular hillocks. These are usually anterior to the tragus, and they may be single or multiple (Fig. 4.1a). They vary in shape but most often consist of skin and subcutaneous tissue. Occasionally, there is cartilage in the base of the tag.
Indications
Removal of the preauricular tags is performed to correct a congenital deformity.
Preoperative Evaluation
No special preoperative evaluation is required, except to recognize that any congenital outer ear anomaly may be associated with the presence of another ear (e.g., ossicular) malformation.
Operative Technique
1. A general anesthetic is usually required. Local infiltration of the base of the preauricular tag with 1% lidocaine containing 1:100,000 epinephrine will decrease bleeding.
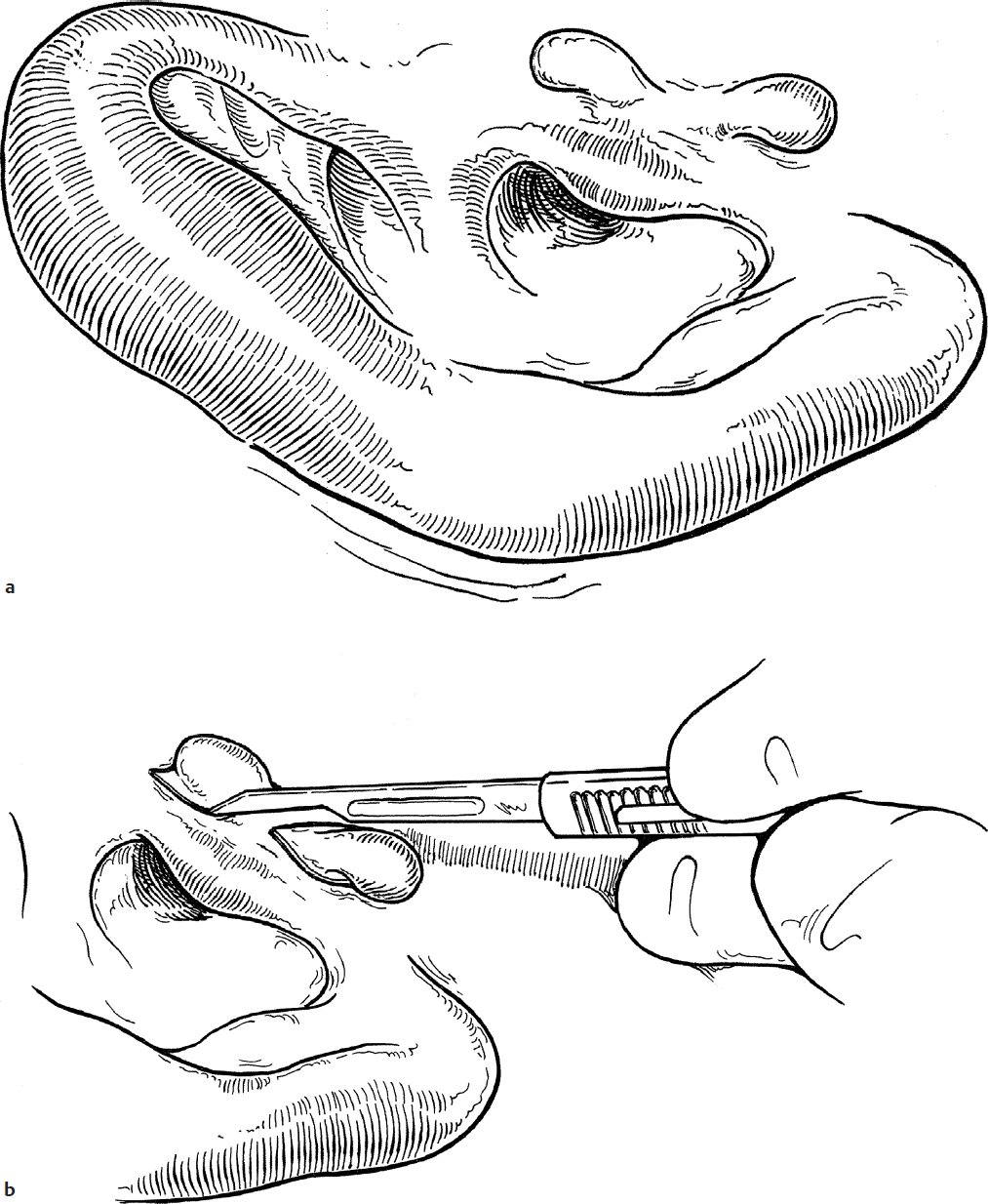
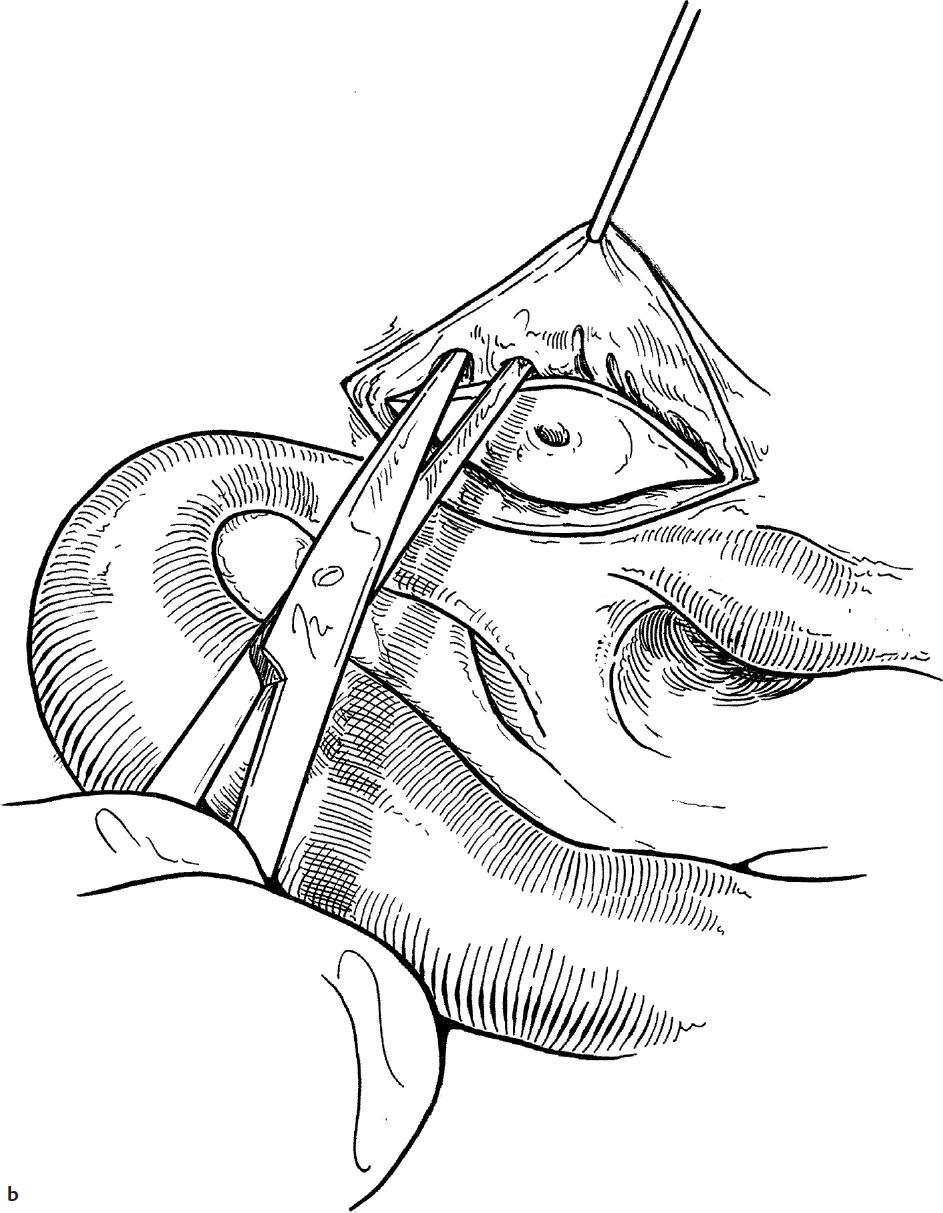
2. An elliptical skin incision is made in the lines of the facial creases in front of the ear (Fig. 4.1b).
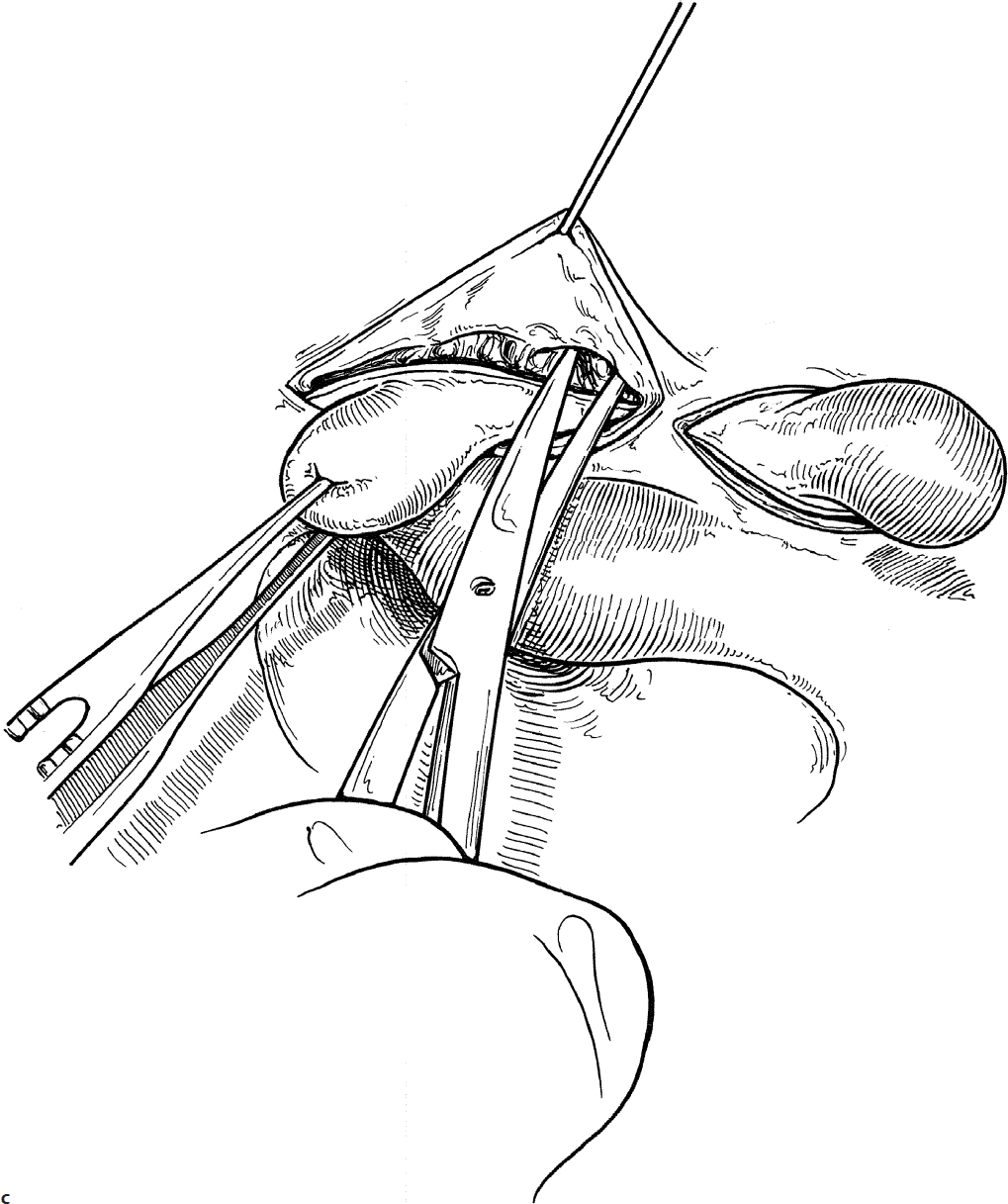
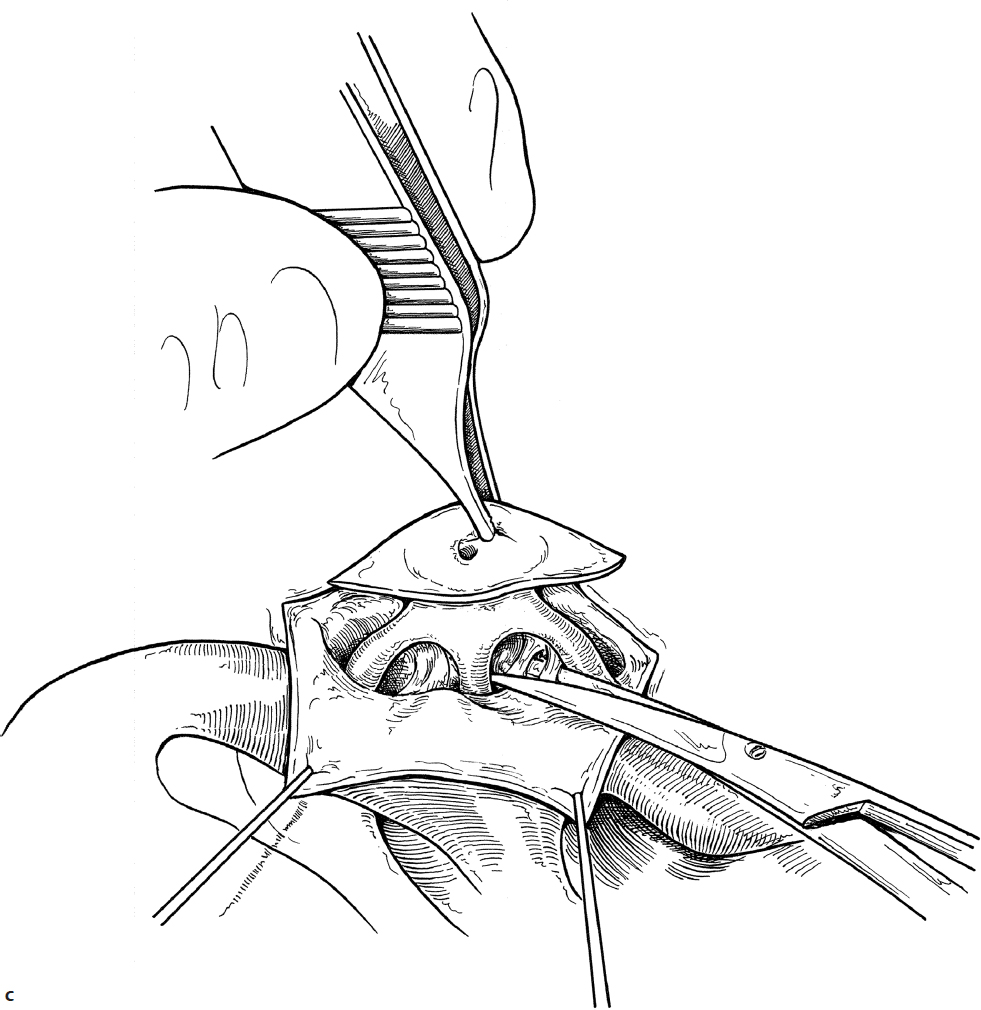
3. The tag can be grasped with a toothed forceps and placed on gentle traction while dissecting the underlying cartilage and subcutaneous tissue with sharp scissors (Fig. 4.1c).
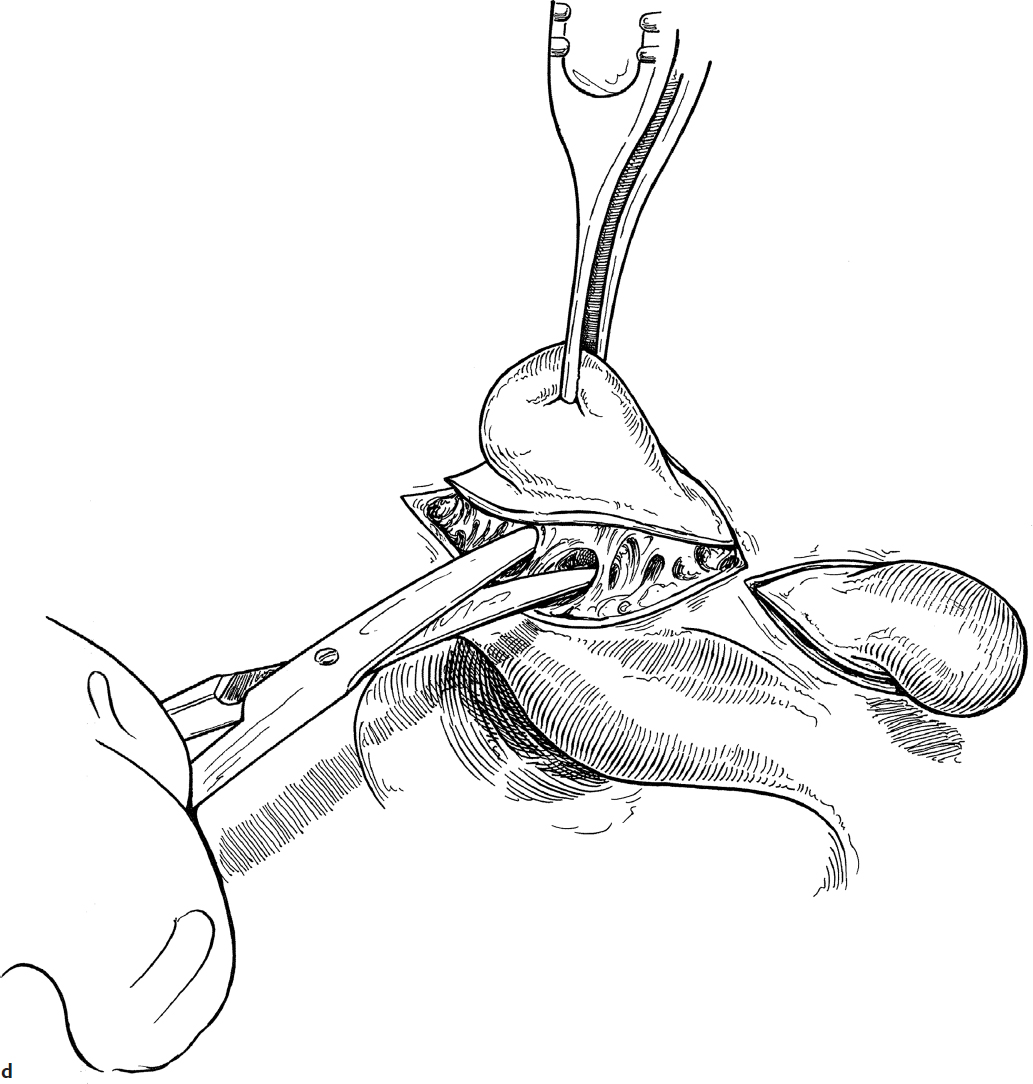
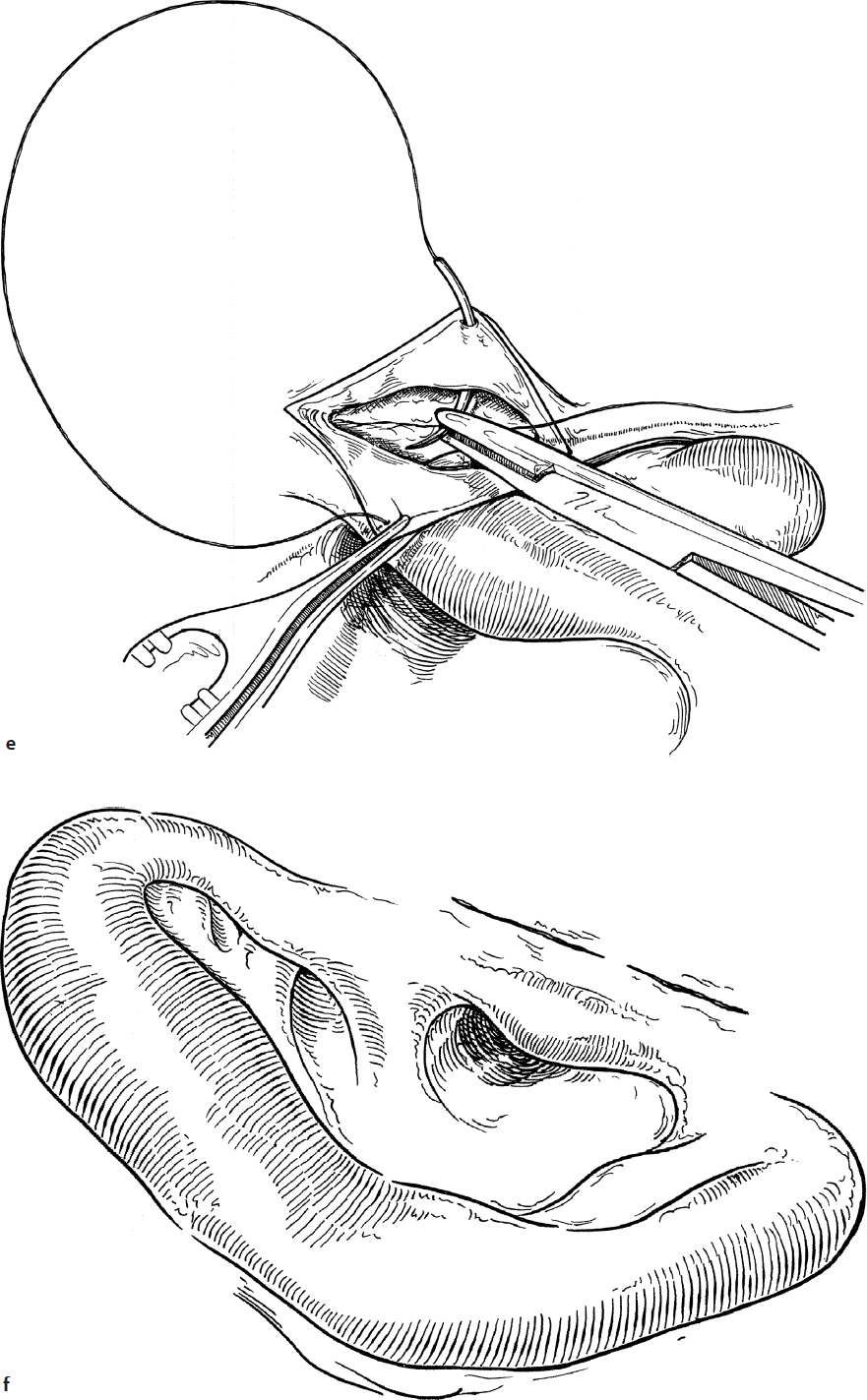
4. The subcutaneous stalk and cartilage are cut free with sharp scissors (Fig. 4.1d).
5. Hemostasis should be obtained with needlepoint cautery.
6. The wound is closed in two layers. The skin is closed with subcuticular absorbable suture, thus avoiding the need to remove skin sutures (Fig. 4.1e,f).
Complications
Hematoma.
4-2 Preauricular Sinuses
Introduction
Preauricular sinuses occur as a result of the trapping of epithelium between the developing ear hillocks. They usually present as a pit in the area just superior and anterior to the tragus. The lesions sometimes arborize in the subcutaneous tissues and often attach to the helical cartilage.
Indications
Asymptomatic sinus tracts require no treatment. Excision is necessary if these skin-lined tracts become infected or form an obvious cyst.
Preoperative Evaluation
No special preoperative evaluation is required except to recognize that any congenital outer ear anomaly may be associated with the presence of another ear (e.g., ossicular) malformation.
Operative Technique
1. Preauricular sinuses are removed under a general anesthetic with local infiltration of 1% lidocaine with 1:100,000 epinephrine for hemostasis.
2. An elliptical incision is made around the skin defect in the preauricular area (Fig. 4.2a).
3. Skin flaps are elevated anteriorly and posteriorly (Fig. 4.2b).
4. Using blunt and sharp dissection, the subcutaneous tracts are followed, avoiding entry into the sinus (Fig. 4.2c). A lacrimal probe may be helpful to determine the direction and degree of arborization and the depth of the tract(s).
5. Preauricular sinuses usually attach to the perichondrium of the helical cartilage; thus the involved perichondrium should be excised in continuity with the cyst. Often perichondrium cannot be easily separated from the cartilage, so an ellipse of helical cartilage should also be excised (Fig. 4.2d).
6. The wound is closed in two layers after hemostasis is obtained. The skin is closed with subcuticular absorbable suture, avoiding the need to remove sutures (Fig. 4.2e).
Complications
Recurrence secondary to incomplete excision.
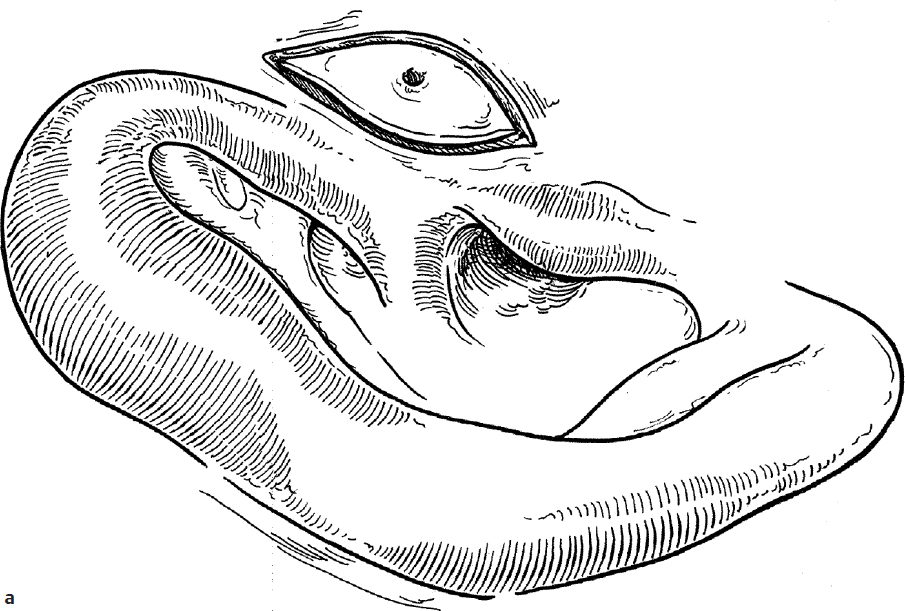
Fig. 4.2a
4-3 Otoplasty
Introduction
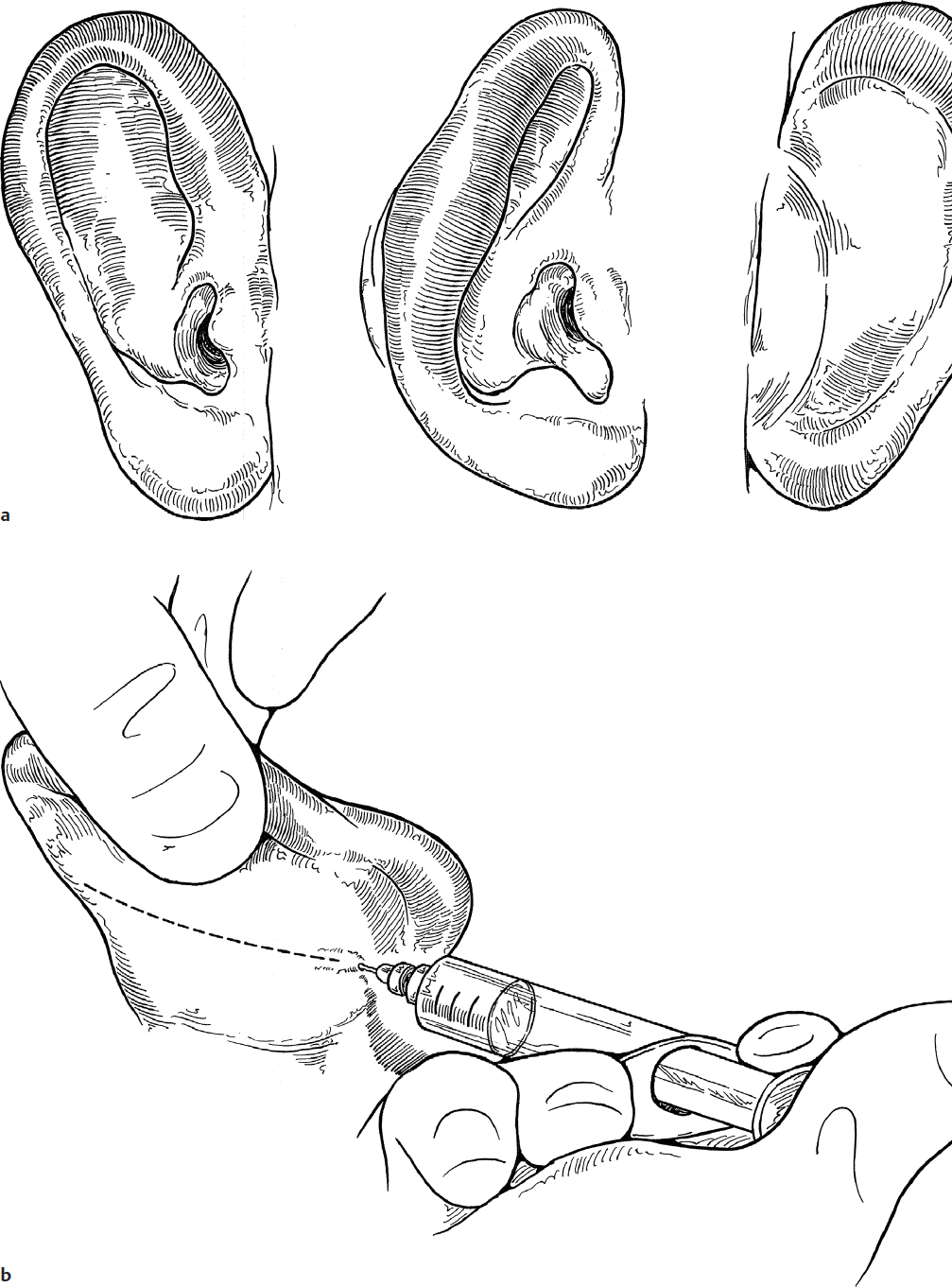
Protruding ear (prominotia) is a relatively common deformity that varies greatly in degree of severity (Fig. 4.3a). It is usually caused by a combination of the absence of the antihelical fold and a large conchal cartilage.
Indications
The indication for surgery is the desire of the child and parents to restore normal anatomy. The procedure is best performed between ages 4 and 5, when the child can cooperate with postoperative care and before the child is subjected to teasing by school-age peers.
Preoperative Evaluation
A complete examination of the ear and external canal is mandatory to determine the components of the deformity. Preoperative photographs are necessary to document the pre-operative condition and to compare to the results after surgery.
Operative Technique
1. General anesthesia is utilized for all children having otoplasty. Both ears should be prepped into the surgical field simultaneously to allow intraoperative comparison of the two ears.
2. The desired degree of correction is determined by manipulating the auricle to create the missing fold in the antihelix and by depressing the concha against the mastoid bone. A marking pen is used to mark the line of the new fold to be created.
3. The posterior surface of the auricle is injected with 1% lidocaine with 1:100,000 epinephrine to aid in hemostasis. The line of injection is the full length of the ear and is halfway between the postauricular fold and the edge of the helix (Fig. 4.3b).
4. An incision is made along the line of injection down to the perichondrium.
5. Skin flaps are elevated on both sides of the incision, in a plane just superficial to the perichondrium, which is left attached to the cartilage.
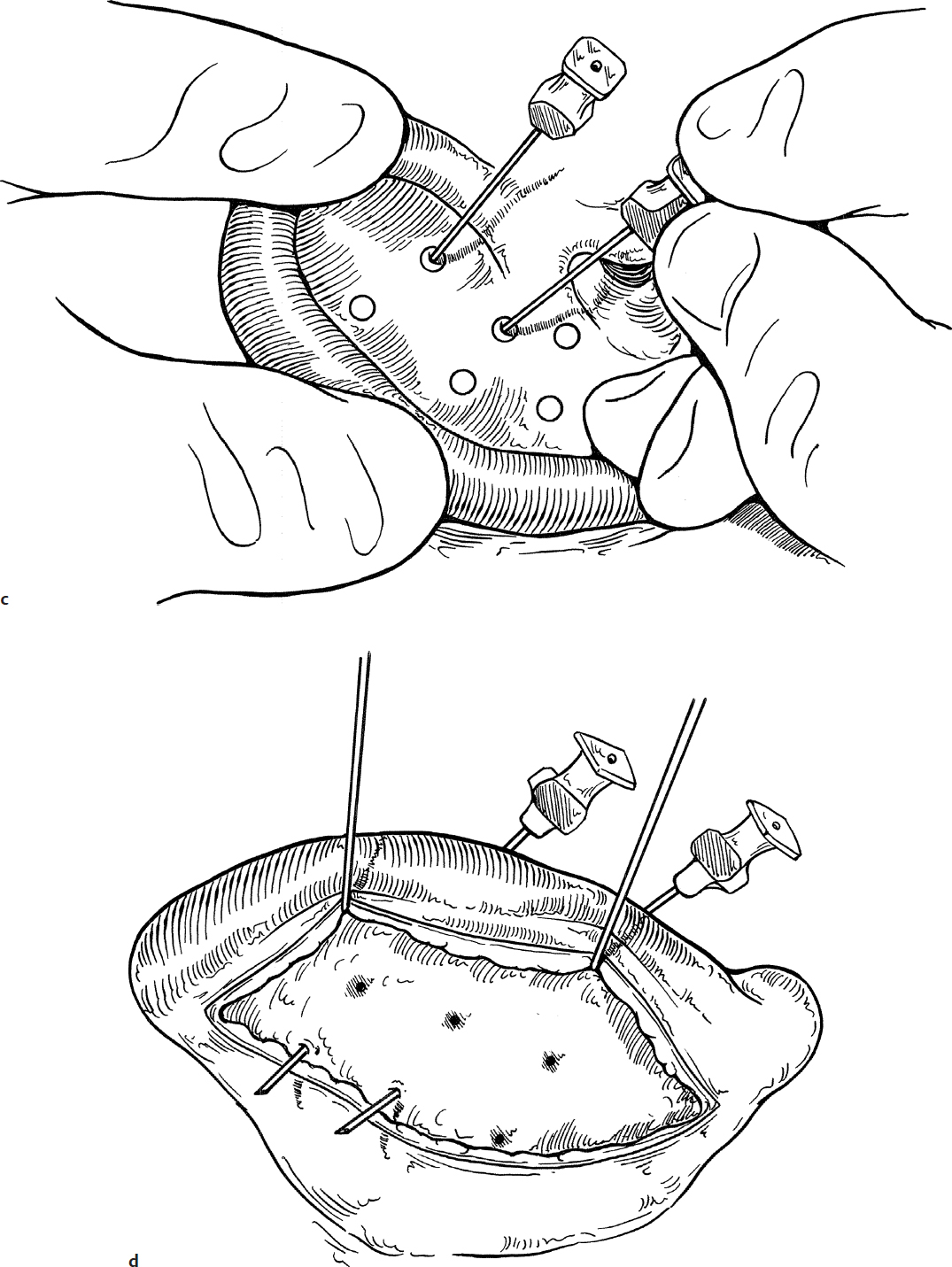
6. The ear is folded along the line drawn in step 2, and three or four locations for mattress suturing are selected, close enough to produce an even contour of the new antihelical fold (Fig. 4.3c). These points (indicated by small circles) should be at least 5 mm from the top of the proposed antihelical fold so that the sutures will create a rounded, and not a sharp, fold.
7. At each of these points, a 25-gauge needle is passed through both skin and cartilage from the anterior surface of the ear. On the wound side, a small dab of methylene blue is then placed on the bevel of the needle, and the needle is removed, marking the cartilage (Fig. 4.3d).
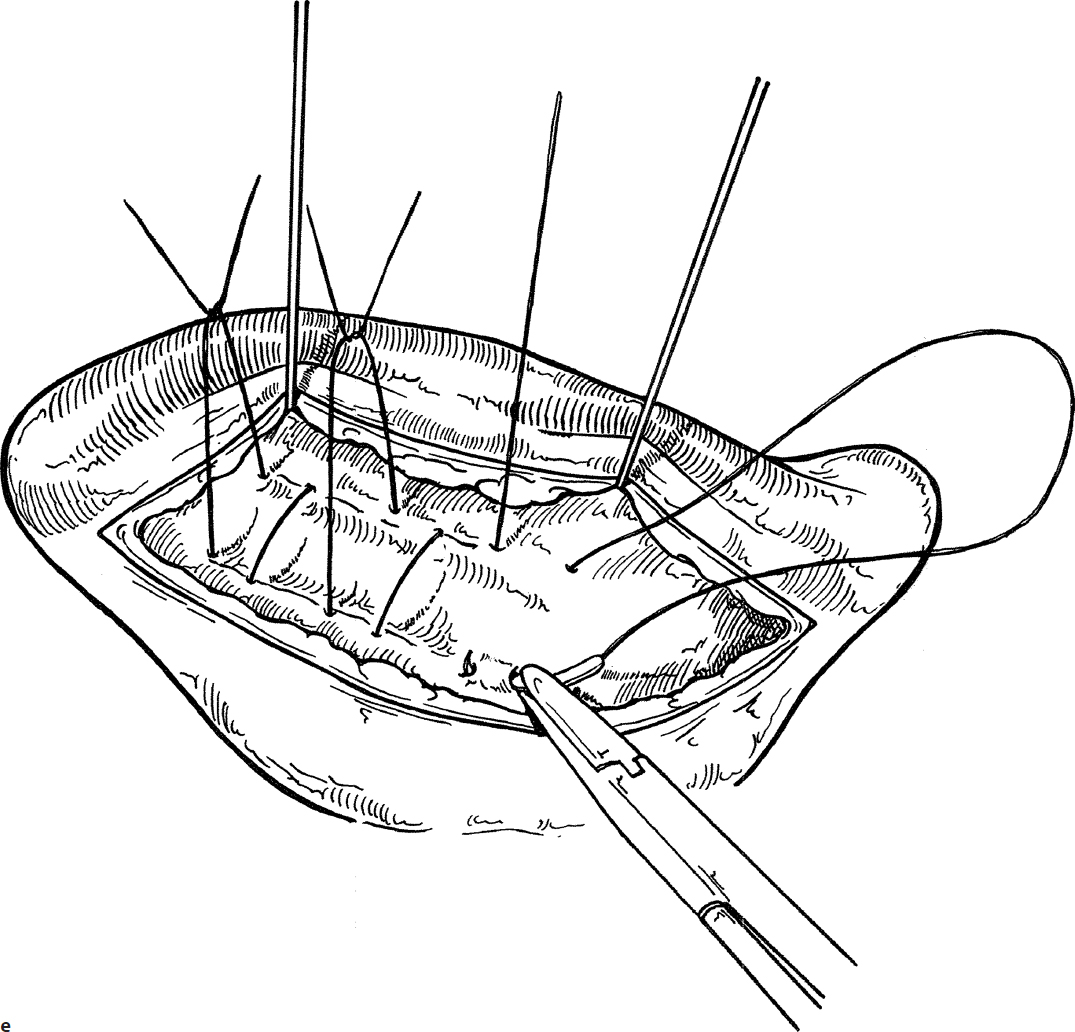
8. Horizontal mattress sutures with 4-0 white Mersilene (Ethicon) are placed at the methylene blue marks to recreate the antihelical fold (Fig. 4.3e). The suture should go through the cartilage and anterior and posterior perichondrium. Care is taken to avoid perforation of the lateral (anterior) skin surface of the ear while placing the sutures.
9. The sutures are tied just tight enough to create the desired effect of a rounded fold (Fig. 4.3f).
10. If it is felt that the concha is prominent, a setback suture of 2-0 or 3-0 Vicryl (Ethicon) can be placed between the concha and the mastoid periosteum to rotate the ear posteriorly against the mastoid cortex (Fig. 4.3g). Care is taken to avoid overcorrection, which results in a “telephone ear” deformity. Degree of setback is carefully matched between left and right ears.
11. If desired, the excess postauricular skin can be removed, but this step is optional.
12. The incision is then closed with 5-0 subcuticular absorbable sutures. No drain is used.
13. The effect of the sutures to create the desired result is demonstrated in Fig. 4.3h.
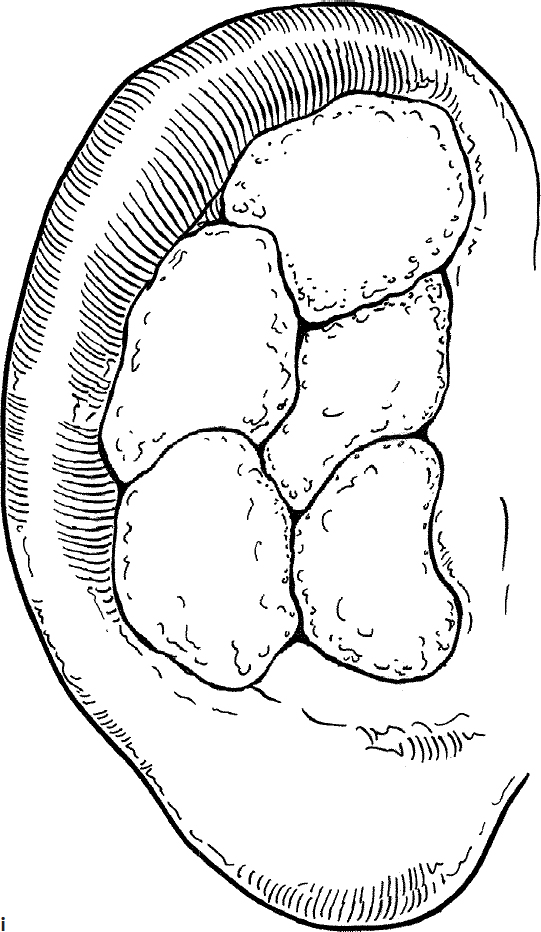
14. Strands of cotton moistened with mineral oil are molded to the anterior surface of the auricle conforming to the auricular folds (Fig. 4.3i).
15. A mastoid dressing consisting of fluff gauze and elastic netting is used to apply gentle pressure. The family is instructed to lift this dressing 24 hours later, remove the oil-soaked cotton, replace the ball of gauze if needed, and wear it again for 24 additional hours of gentle pressure. After that, the dressing is removed, and an elastic terrycloth sports headband is worn for 1 week to keep the ear in place. It is used day and night for 1 week, and then just at night for another week.
Complications
1. Incomplete correction of deformity, or asymmetry of the two ears
2. Overcorrection (“telephone ear” deformity)
3. Delayed recurrence of the deformity due to relaxation or failure of the sutures
4. Unnatural appearance of auricle
5. Infection (chondritis)
4-4 Middle Ear Exploration—Exploratory Tympanotomy
Introduction
Middle ear exploration is performed to examine the contents and condition of the middle ear. Middle ear exploration should permit adequate visualization of the ossicular chain to assess mobility, as well as inspection of the region of the oval and round windows. If there is suspected pathology in the epitympanum, the bone of the posterosuperior ear canal wall can be removed (atticotomy) to explore the area of the ossicular heads.
Indications
Middle ear exploration is indicated to determine the causes of and to correct a conductive hearing deficit, to biopsy or remove middle ear masses such as congenital cholesteatoma, to rule out persistent or recurrent disease following prior cholesteatoma excision, or to identify and repair a perilymph fistula.
Preoperative Evaluation
The preoperative evaluation of conditions affecting the middle ear includes pneumatic otoscopy, complete audiometry, and usually computed tomography (CT). Magnetic resonance imaging (MRI) is rarely helpful in the evaluation of the middle ear.
Binocular microscopy provides better assessment of the tympanic membrane and middle ear than simple otoscopy and is used when possible. Pneumatic insufflation while under microscopy can be helpful. Careful inspection for movement of the malleus handle during insufflation may reveal malleus fixation, which can help guide surgical planning.
Operative Technique
Middle ear exploration in children is performed under general anesthesia. Adequate exposure may be possible in older children using a transcanal approach, but most often a postauricular approach as described for tympanoplasty (see Section 3-2) provides better exposure (especially anteriorly).
1. If the transcanal approach is selected, local anesthetic (1% lidocaine with 1:100,000 epinephrine) is injected into the skin of the ear canal (refer to dots, Fig. 4.4a) and in the posterior cartilaginous ear canal just lateral to the bony–cartilaginous junction (Fig. 4.4a).
2. If a postauricular incision is used, the approach is identical to that used to enter the middle ear for tympanoplasty (see Section 3-2).
3. An incision is made from a spot above the short process of the malleus to the posteroinferior portion of the ear canal, at a distance approximately 5 to 7 mm from the annulus (Fig. 4.4b). The superior or inferior limb of the incision can be extended to provide access to the anterosuperior or inferior quadrants, respectively. If the heads of the ossicles need to be explored via atticotomy, the incision should be carried farther anteriorly, and the flap made longer at superior pole (at least 10 mm) to allow later coverage of the atticotomy defect.
4. The ear canal skin flap is elevated until the fibrous annulus of the tympanic membrane is identified (Fig. 4.4c).
5. The annulus is elevated with a knife or sulcus elevator along the full extent of the incision, and the middle ear is entered (Fig. 4.4d).
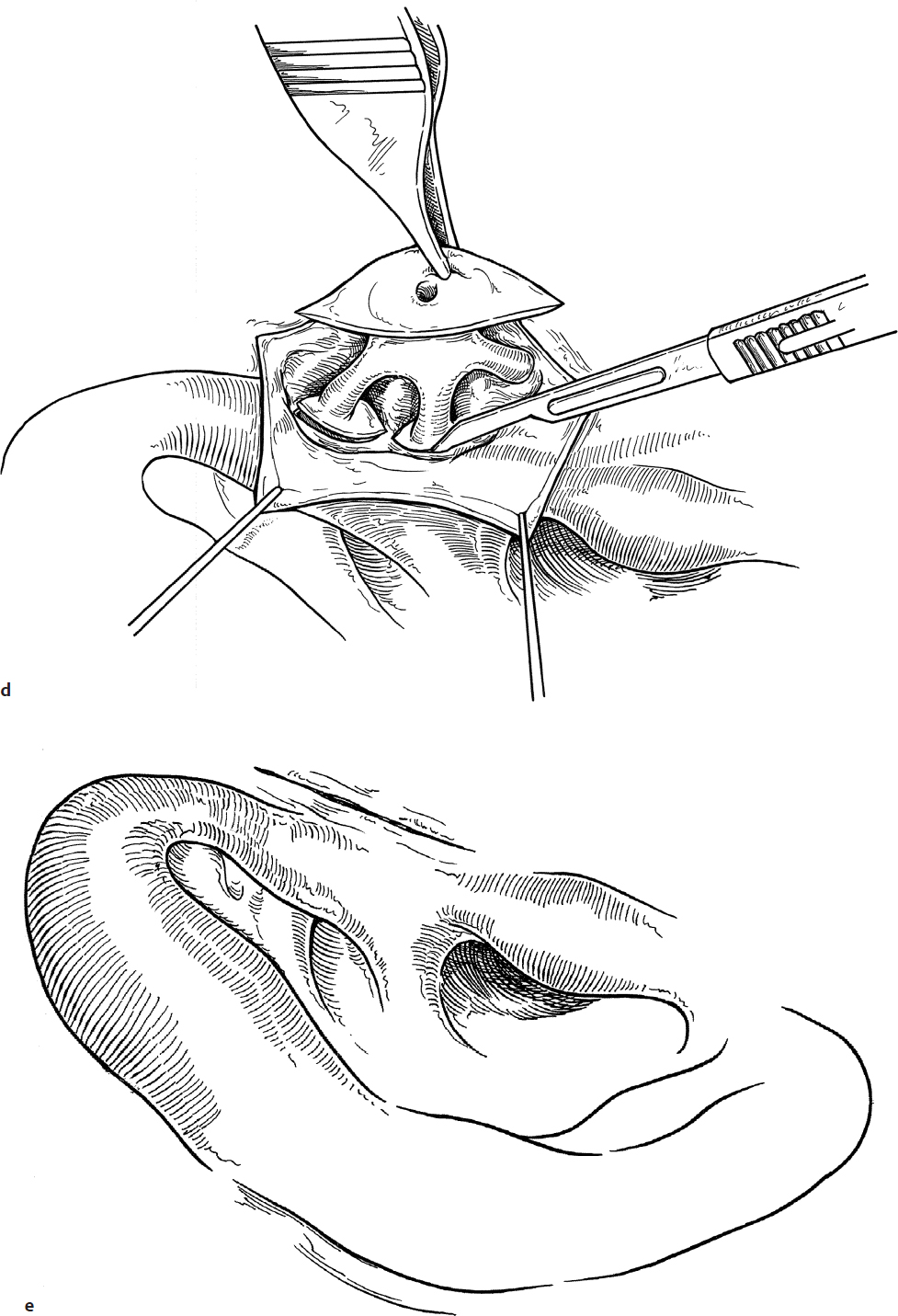
6. The tympanomeatal flap can then be folded anteriorly to expose the contents of the middle ear (Fig. 4.4e).
7. Bone of the posterosuperior canal wall may be removed with a curette or drill for full exposure of the stapes foot-plate, if necessary. Care is taken to avoid trauma to the chorda tympani nerve (Fig. 4.4e).
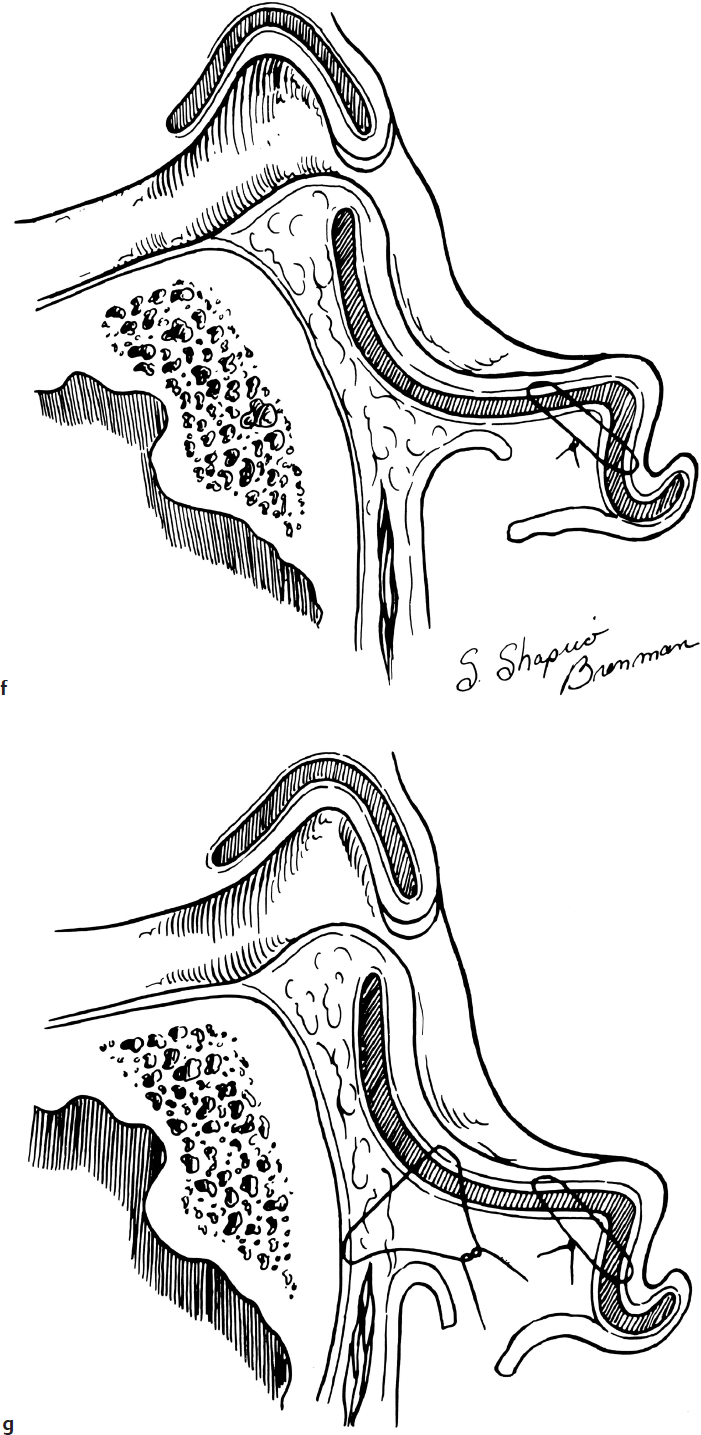
8. If anterosuperior exposure is desired for excision of a congenital cholesteatoma, an incision is made in the periosteum along the full length of the posterior surface of the malleus with a micro-Tabb knife by scraping against the bone (Fig. 4.4f).
9. The mucoperiosteum is then released from the malleus by dissection with a micro-Tabb knife until the anterosuperior quadrant is visualized (Fig. 4.4g).
10. If needed, the tympanic membrane can be released from its attachment to the malleus at the umbo by cutting the fibrous bands with a sharp blade or microscissors. However, if possible, the flap should be left attached here to help prevent lateralization of the tympanic membrane postoperatively.
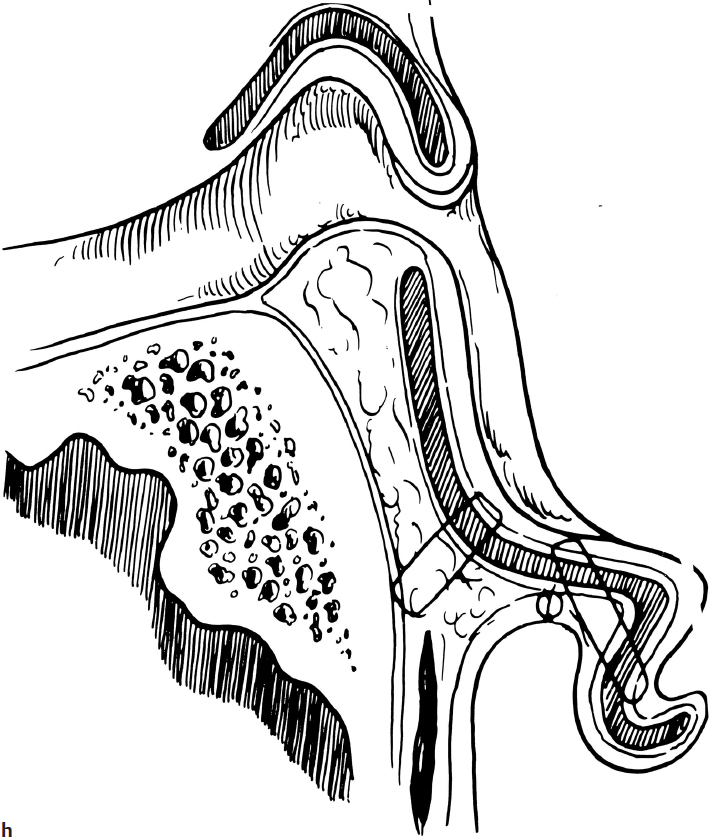
11. If pathology around the ossicular heads is suspected, an atticotomy is performed. This is done with an otologic drill and a 1.5- to 2-mm diamond bur at slow speed (Fig. 4.4h). Care is taken to avoid direct drilling onto the ossicular heads, especially upon removal of the innermost bone layer. A safe approach is to thin this bone with the drill until almost transparent and then remove the remainder with a curette.
12. Inspection of the round window region can help in assessment of ossicular chain mobility. Normally a brisk movement (round window reflex) is seen upon gentle ossicular palpation. If the round window cannot be directly visualized, a drop of saline can be placed in the round window niche, and movement of its meniscus/light reflection can be elicited.
13. If an atticotomy was performed, this ear canal defect should be reconstructed with a cartilage graft, laid across the defect and supported by its bony edges, prior to replacement of the skin flap and TM (Fig. 4.4i).
14. When the middle ear surgery is complete, the tympanomeatal flap is replaced, and a single large piece of Gelfoam (Pfizer) is placed across the incision line (Fig. 4.4j).
Complications
1. Failure to improve conductive hearing loss
2. Sensorineural hearing loss due to ossicular trauma
3. Ossicular disruption
4. Chorda tympani trauma
5. Perforation of the tympanic membrane