Congenital subglottic stenosis is rare and as a consequence may not be considered in children experiencing respiratory difficulty at birth. Diagnosis after a child already is intubated complicates the recognition and blurs the boundary between congenital and acquired lesions. This article discusses the anatomy of the larynx, its common anatomic variations, and its response to trauma, a thorough understanding of which is required for the accurate diagnosis and treatment of this complicated problem. The authors discuss evaluation and assessment options to guide treatment.
Subglottic stenosis is one of the most common causes of airway obstruction in infants and children. It is the second most common cause of stridor in infants and the most common laryngotracheal anomaly requiring tracheostomy in children younger than age 1 year . An accurate understanding of the anatomy of the larynx, its common anatomic variations, and its response to trauma are required for the accurate diagnosis and treatment of this complicated problem.
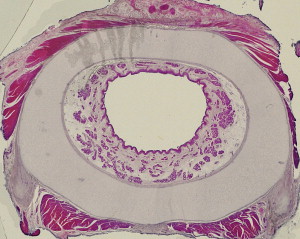
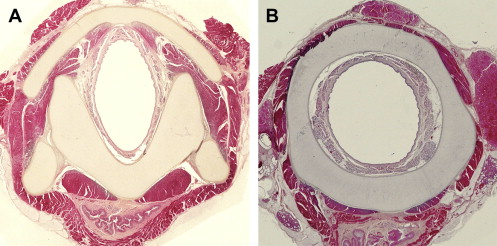
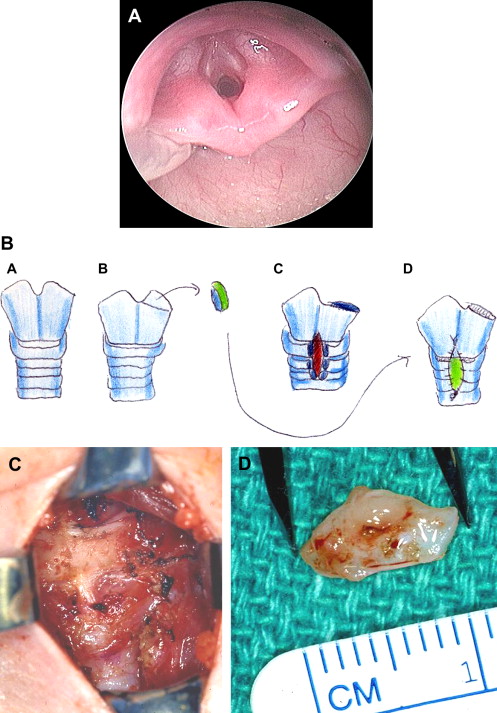
Precise descriptive terms are especially important for laryngotracheal stenosis. The subglottis is defined as the region extending from the insertion of the conus elasticus into the vocal folds to the inferior margin of the cricoid cartilage . The diameter of the normal subglottic lumen is 4.5 to 5.5 mm in a full-term neonate and approximately 3.5 mm in a preterm baby. A subglottic airway diameter of 4 mm or less in a full-term infant or 3 mm or less in a premature infant is considered narrow and consistent with a diagnosis of subglottic stenosis . In their description of serial sections of the larynx, Tucker and colleagues characterized the upper- and midposterior lamina of the normal cricoid cartilage as V-shaped and midcricoid level and lumen as elliptic in shape ( Fig. 1 A). Only at its inferior portion does the cricoid cartilage assume the shape of a smooth, round ring (see Fig. 1 B).
Subglottic stenosis may be categorized in many ways ( Table 1 ). These can be classified broadly by cause (congenital or acquired), by clinical or anatomic characteristics (hard or soft, degree or percentage of stenosis, and precise location), and by histopathology . Most treatment decisions are based on the severity of a stenosis, the clinical anatomic characteristics of a stenosis, and the degree of inflammation rather than on etiology (congenital versus acquired).
| 1. Cartilaginous stenosis (usually congenital) |
| a. Cricoid cartilage deformity |
| i. Normal shape, small size |
| ii. Abnormal shape |
| 1. Elliptic |
| 2. Cleft (partial, submucosal, incomplete) |
| 3. Flattened |
| 4. Other (including acquired lesions) |
| a. Fragmented, distorted cricoid |
| b. Cricoid ossification |
| c. Thickened cricoid |
| b. Trapped first tracheal ring |
| 2. Soft tissue stenosis (usually acquired) |
| a. Submucosal mucous gland hyperplasia |
| b. Ductal cysts |
| c. Submucosal fibrosis (fibrous connective tissue) |
| d. Granulation tissue |
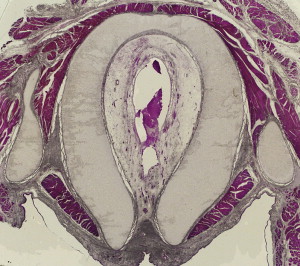
A review of serial sections of 129 whole organ larynges catalogs common congenital cricoid abnormalities . The elliptic cricoid, first described by Tucker and colleagues in 1979, is the most frequently diagnosed abnormal shape that causes congenital subglottic stenosis. At the inferior border of the normal larynx, the transverse and anterioposterior diameters should be equal. In the elliptic cricoid, the transverse diameter is less than the anterioposterior diameter ( Fig. 2 ). This results in a loss of cross-sectional area. The elliptic cricoid often is found in association with other congenital laryngeal anomalies, such as posterior laryngeal cleft . In the flattened cricoid, the transverse diameter is greater than the anterioposterior diameter ( Figs. 3–5 ). This flattened shape also may be associated with a trapped first tracheal ring . The trapped first ring rides up inside the cricoid cartilage where it reduces the size of the lumen. A thickened cricoid has been observed clinically and histopathologicaly (see Fig. 3 ).

Understanding the various cricoid anomalies is important to clinical otolaryngologists–head and neck surgeons for two reasons:
- 1.
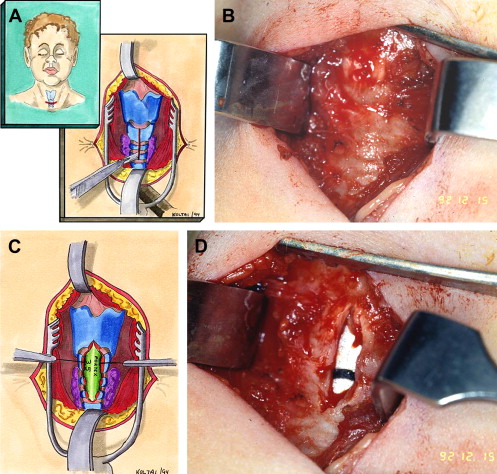
Rational therapy of laryngotracheal stenosis cannot be planned without defining the precise extent and nature of each lesion . For, example, cartilaginous stenoses are not responsive to dilation or laser vaporization, but these modalities often can be used to treat soft tissue subglottic stenosis ( Fig. 6 ).