Congenital Anomalies of the Optic Disc
Ophthalmologists and neurologists frequently are asked to evaluate patients with anomalous optic discs. A comprehensive evaluation requires an understanding of the ophthalmoscopic features, associated neuro-ophthalmologic findings, pathogenesis, and appropriate ancillary studies for each anomaly. Increased recognition of the ocular and systemic associations related to each anomaly has advanced our understanding of its pathogenesis. For instance, different forms of excavated optic disc anomalies that were previously lumped together as colobomatous defects are now subclassified. This has enhanced our ability to predict the likelihood of associated central nervous system (CNS) anomalies based solely on the appearance of the optic disc. In addition, the widespread clinical application of computed tomographic (CT) scans and magnetic resonance imaging (MRI) has enabled us to more accurately identify associated CNS anomalies and predict the likelihood of subsequent neurodevelopmental and endocrinologic problems.
Certain general principles are particularly useful in the evaluation and management of patients with anomalous optic discs.
Children with bilateral optic disc anomalies generally present in infancy with poor vision and nystagmus; those with unilateral optic disc anomalies generally present during their preschool years with sensory esotropia.
CNS malformations are common in patients with malformed optic discs. Small discs are associated with a variety of malformations of the cerebral hemispheres, pituitary infundibulum, and midline intracranial structures (septum pellucidum, corpus callosum). Large optic discs of the morning glory configuration are associated with the transsphenoidal form of basal encephalocele, whereas colobomatous optic discs may be associated with systemic anomalies and a variety of syndromes.
Any structural ocular abnormality that reduces visual acuity in infancy may lead to superimposed amblyopia. A trial of occlusion therapy may be warranted in young children with unilateral optic disc anomalies and decreased vision.
Anomalous Optic Disc Elevation (Pseudopapilledema)
Anomalous optic disc elevation (pseudopapilledema) may bear a striking resemblance to true optic disc swelling. As most patients with pseudopapilledema have no visual symptoms, this condition is often mistaken for papilledema. In most instances, a patient is noted to have elevated optic discs or blurred disc margins during the course of a routine examination. The diagnostic uncertainty and alarm created by this finding overshadows the fact that the patient has no other signs or symptoms of increased intracranial
pressure. Many patients with pseudopapilledema thus are referred for neuro-ophthalmologic evaluation only after being subjected to neuroimaging, lumbar puncture, and extensive laboratory studies.
pressure. Many patients with pseudopapilledema thus are referred for neuro-ophthalmologic evaluation only after being subjected to neuroimaging, lumbar puncture, and extensive laboratory studies.
Pseudopapilledema may be caused by underlying optic disc drusen that may be superficial and obvious on funduscopic examination or deep (“buried”) and identifiable only with ancillary studies such as optical coherence tomography, ultrasonography, or CT scanning. In other cases, no drusen are present. In such cases, the nerve may be smaller than normal (i.e., optic nerve hypoplasia) or tilted, resulting in general or focal elevation of the disc tissue.
Pseudopapilledema Associated with Optic Disc Drusen
The word drusen, of Germanic origin, originally meant tumor, swelling, or tumescence. The word was used in the mining industry approximately 500 years ago to indicate a crystal-filled space in a rock. Other terms for these lesions include hyaline bodies and colloid bodies of the optic disc. It is unfortunate that the term “drusen” is used both for these lesions and for the hypopigmented lesions of the retinal pigment epithelium that may precede the development of macular degeneration.
Drusen of the optic disc are homogeneous, globular concretions, often collected in larger, multilobulated agglomerations. They usually exhibit a concentrically laminated structure that is not encapsulated and contains no cells or cellular debris. Optic disc axons are atrophic adjacent to large accumulations of drusen, whereas axons not adjacent to the drusen are normal. Drusen take up calcium salts and must be decalcified before being cut into sections for histopathologic study. According to most investigators, drusen are composed predominantly of a mucoprotein matrix with significant quantities of acid mucopolysaccharides, small quantities of ribonucleic acid and, occasionally, iron. Drusen are insoluble in most of the common solvents.
The primary pathology of optic disc drusen appears to be an inherited dysplasia of the optic canal or of the optic disc and its vasculature, resulting in narrowing of the lamina cribrosa and, thus, of the exit space of optic nerve axons from the eye. The small optic disc size and absence of a central cup in eyes with disc drusen are consistent with the concept of axon crowding. The crowding, in turn, leads to abnormal axon metabolism, with deposition of calcium crystals in mitochondria of intact axons. The axons subsequently become disrupted, and the mitochondria are extruded into the extracellular space, where a higher concentration of calcium ions causes further calcium deposition into the mitochondria. Eventually, these calcified mitochondria coalesce to form drusen.
The prevalence of optic disc drusen depends on the method of analysis. For example, in a clinical series from Scandinavia, the prevalence of optic drusen was 0.3%, whereas the prevalence of drusen in autopsy series is, as might be expected, somewhat higher, varying between 0.4% and 2.0%. Men and women are equally affected, with bilateral drusen occurring in 67% to 85% of cases. The age at which visible drusen or pseudopapilledema caused by buried drusen is diagnosed varies widely, depending on the population studies. Familial drusen are transmitted as an autosomal-dominant trait. The prevalence of disc drusen in African Americans is low, possibly attributable to racial variation in optic disc size.
The evolution of disc drusen is a dynamic process that continues throughout life. It is rare to see visible drusen or significant optic disc elevation in an infant. During childhood, however, the affected optic disc begins to appear “full” and acquires a tan, yellow, or straw color (Fig. 3.1A). The buried drusen gradually impart a scalloped appearance to the margin of the disc and produce subtle excrescences on the disc surface that tend to predominate nasally (Fig. 3.1B). These later enlarge, calcify, and become more visible on the disc surface (Fig. 3.1C). As they enlarge, they sometimes deflect retinal vessels overlying the disc. In adulthood, the optic disc elevation diminishes, the disc gradually becomes pale, the nerve fiber layer thins, and discrete slits appear. This evolution reflects a slow attrition of optic axons over decades. Despite this progression, most patients remain asymptomatic and retain normal acuity.
Although all drusen are located anterior to the lamina cribrosa, drusen may be classified as superficial or buried. Superficial drusen can be identified easily by their ophthalmoscopic appearance. Buried drusen, however, can only be suspected by the general appearance of the optic disc and surrounding peripapillary retina but cannot be diagnosed with certainty without ancillary testing such as OCT or CT scanning.
Superficial drusen appear as round, slightly irregular excrescences that are present within and occasionally around the disc (Figs. 3.1B and C and 3.2). They may be scattered or form conglomerates that cover the disc, reflect whitish yellow light, are globular, and vary in size from minute dots to granules 2 or 3 times the diameter of a retinal vessel. In some cases, drusen located just below the disc surface may be illuminated when indirect lighting is used.
Drusen buried within the tissue of the disc produce moderate elevation of the surface of the disc, as well as blurring of its margins (Figs. 3.1A and B and 3.3). It is this appearance that mimics true disc swelling; however, the anomalously elevated disc is not hyperemic, and there are no dilated capillaries on its surface. In addition, despite obvious elevation of the disc, the surface vessels, even small ones, are not obscured, the physiologic cup is absent, and the peripapillary
retinal nerve fiber layer retains its normal linear pattern unless there are abnormalities indicative of nerve fiber layer atrophy. Anomalously elevated discs are smaller than normal and sometimes have an irregular border with pigment epithelial defects being present. The most elevated portion of the disc is usually the central area from which the vessels emerge. In a large percentage of cases, there are anomalous vascular patterns on the disc surface, including an increased number of otherwise normal vessels, abnormal arterial and venous branchings, increased tortuosity, vascular loops, and cilioretinal arteries.
retinal nerve fiber layer retains its normal linear pattern unless there are abnormalities indicative of nerve fiber layer atrophy. Anomalously elevated discs are smaller than normal and sometimes have an irregular border with pigment epithelial defects being present. The most elevated portion of the disc is usually the central area from which the vessels emerge. In a large percentage of cases, there are anomalous vascular patterns on the disc surface, including an increased number of otherwise normal vessels, abnormal arterial and venous branchings, increased tortuosity, vascular loops, and cilioretinal arteries.
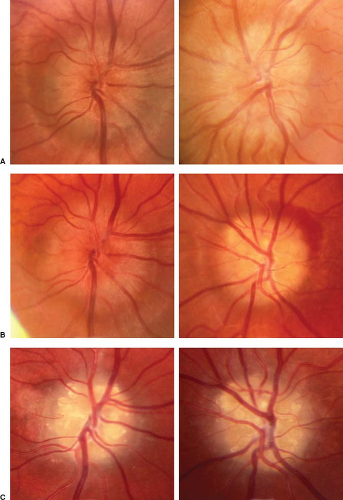 Figure 3.1 Evolution from buried to visible optic disc drusen over 20 years. A: At initial diagnosis. B: 5 years later. C: 10 years later. |
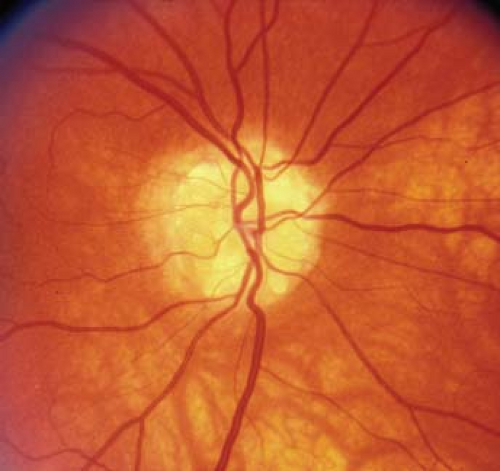 Figure 3.2 Visible optic disc drusen. Note globular glistening appearance with elevation of vessels overlying the optic disc. |
The distinction between pseudopapilledema associated with buried drusen and papilledema (or other forms of optic disc swelling) can be difficult, but several clinical signs are particularly helpful (Table 3.1).
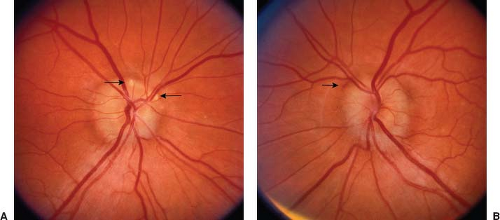 Figure 3.3 Buried optic disc drusen. A: The right optic disc is elevated. Two druse are visible (arrows). B: The left optic disc is diffusely elevated, but it is not hyperemic and the vessels crossing its surface, even the smallest, are easily seen. A small subretinal peripapillary hemorrhage is present (arrow). |
The differentiation between papilledema and pseudopapilledema caused by buried drusen is frequently aided by ancillary studies. Special photographic techniques may be useful in identifying superficial or buried optic disc drusen. Monochromatic (red-free) photography may highlight the glistening drusen against the intact or atrophic nerve fiber layer. Photographs taken with the filters normally used for fluorescein photography in place, but without injection of fluorescein, show that superficial disc drusen often demonstrate the phenomenon of autofluorescence (Fig. 3.4B). Fluorescein angiography also can facilitate the differentiation between true papilledema and pseudopapilledema. After intravenous fluorescein injection, drusen exhibit a true nodular hyperfluorescence corresponding to the location of the visible drusen (Fig. 3.4C). The late phases may be characterized by minimal blurring of the drusen that either fade or maintain fluorescence (i.e., stain). Unlike in papilledema, however, there is no visible leakage along the major vessels. Fluorescein angiography also may disclose venous anomalies (venous stasis, venous convolutions, and retinociliary venous communications) and staining of the peripapillary vein walls in eyes with optic disc drusen. In addition to the above photographic techniques, CT scanning (often obtained when papilledema is suspected), OCT (particularly using enhanced depth imaging), and ultrasonography will
all demonstrate calcifications within the elevated optic disc associated with optic disc drusen (Fig. 3.5).
all demonstrate calcifications within the elevated optic disc associated with optic disc drusen (Fig. 3.5).
Table 3.1 Ophthalmoscopic Features Useful in Differentiating Acquired Optic Disc Swelling from Pseudopapilledema Associated with Buried Drusen | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
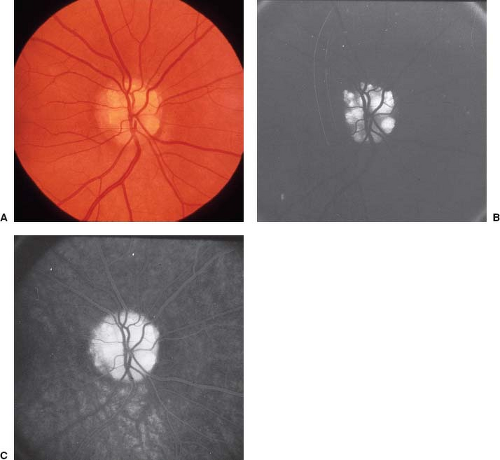 Figure 3.4 Fluorescent characteristics of optic disc drusen. A: Fundus photograph of optic disc drusen. B: Autofluorescence of drusen observed through a fluorescein filter but without injection of fluorescein dye. C: Late staining of drusen after fluorescein angiogram. |
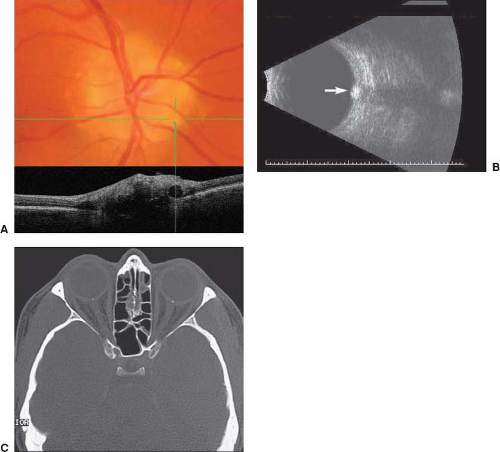 Figure 3.5 Methods of diagnosing buried optic disc drusen. A: Optical coherence tomography shows a circular appearance of a druse. B: B-scan ultrasonography in a patient with deep (buried) optic disc drusen. The area of disc elevation is clearly seen as is a focal area of brightness (arrow). C: Noncontrast axial computed tomographic scan (bone-window level) in a patient with bilateral buried drusen shows a focus of increased density at the site of each optic disc. |
Although patients with pseudopapilledema are not immune to the neurologic and ophthalmologic disorders of the general population, there is no significant relationship between drusen and neurologic disorders.
Most patients with optic disc drusen are asymptomatic and remain so throughout life. Nevertheless, such patients occasionally experience visual loss.
Acute visual loss is rare in patients with optic disc drusen (see below); however, peripheral visual field defects eventually develop in up to 75% of eyes with disc drusen. In most cases, the field defects are asymptomatic (at least initially) because they develop over decades, reflecting the insidious atrophy of optic nerve fibers. Nevertheless, a minority of patients experience episodes of sudden, step-like visual field loss. Visual field defects are much more common in eyes with visible drusen than in those with pseudopapilledema. The defects are of many types, including nasal steps, arcuate defects, sector defects, enlargement of the blind spot; and concentric visual field constriction (Fig. 3.6). A relative afferent pupillary defect may result from unilateral or asymmetric visual field loss in the absence of central acuity loss.
The pathogenesis of visual field loss in patients with optic disc drusen is unclear. In some cases, it is assumed that there is impaired axon transport in an eye with a small scleral canal, leading to gradual attrition of optic nerve fibers. In others, direct compression of prelaminar nerve fibers or of arterioles or capillaries supplying the anterior optic nerve are thought to be responsible.
At the heart of the controversy is whether or not drusen produce damage to nerve fibers through direct axon or vascular compression, or if they are merely an epiphenomenon of a chronic low-grade axon stasis that produces a slowly progressive diminution in optic axons. Several studies have been unable to correlate the location of visible disc drusen with the location of field defects.
Central visual loss is a rare but well-documented complication of disc drusen that should be considered only when no other causes can be identified. In these cases, the visual loss usually follows a series of
episodic, step-like events that progressively diminish the peripheral visual field. In other cases, the decreased acuity is associated with a new field defect and true optic disc swelling associated with peripapillary retinal hemorrhages; that is, the picture of anterior ischemic optic neuropathy.
episodic, step-like events that progressively diminish the peripheral visual field. In other cases, the decreased acuity is associated with a new field defect and true optic disc swelling associated with peripapillary retinal hemorrhages; that is, the picture of anterior ischemic optic neuropathy.
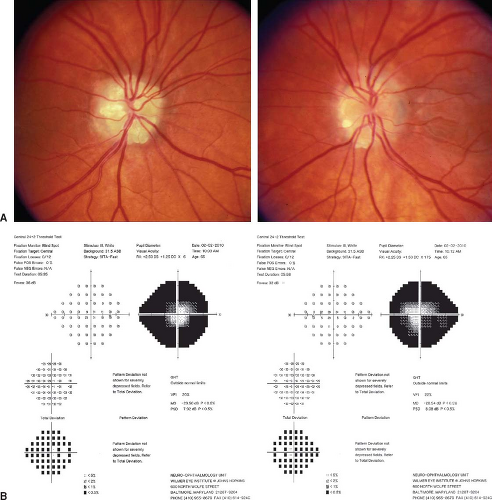 Figure 3.6 Visual fields in a patient with bilateral extensive optic disc drusen. A: Both optic discs are filled with drusen. B: There is marked constriction of the fields of both eyes. |
Prepapillary or peripapillary hemorrhages may develop in eyes with disc drusen. Such hemorrhages may be small, superficial, and located on the optic disc, in which case they tend to be single and prepapillary in location, in contrast to the multiple nerve fiber layer hemorrhages that characterize papilledema. In other cases, there may be a large, superficial hemorrhage overlying the optic disc and, on occasion, extending into the vitreous. Most often, however, the hemorrhages associated with optic disc drusen are peripapillary, subretinal, or subepithelial, and circumferentially oriented around the disc (Figs. 3.3 and 3.7). Most patients with optic disc drusen and hemorrhages have a good visual prognosis.
Retinal vascular occlusions, both arterial and venous, can occur in patients with optic disc drusen. They tend to occur in young adults but rarely may be seen in children. Retinal vascular occlusions that occur in eyes with disc drusen could result from vascular crowding secondary to the small scleral canal size in eyes with drusen, anomalous
optic disc vasculature that may make it more susceptible to the effects of disrupted hemodynamics, or mechanical displacement of the prelaminar vasculature by the calcified fixed drusen.
optic disc vasculature that may make it more susceptible to the effects of disrupted hemodynamics, or mechanical displacement of the prelaminar vasculature by the calcified fixed drusen.
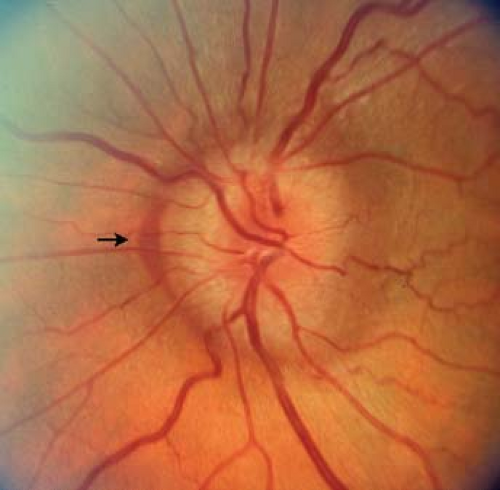 Figure 3.7 Peripapillary subretinal hemorrhage (arrow) in a patient with buried drusen. |
Transient visual loss occurred in 8.6% of the patients with disc drusen in one large study. This phenomenon may occur because of anomalous elevation of the optic disc. Like papilledema, optic disc drusen produce increased interstitial pressure and decreased perfusion pressure in the intraocular portion of the optic nerve. Thus, minor fluctuations in arterial, venous, or cerebrospinal fluid pressure may result in brief but critical decrements in perfusion, leading to transient obscurations of vision. Rarely, transient visual loss is a harbinger of retinal vascular occlusion in patients with disc drusen.
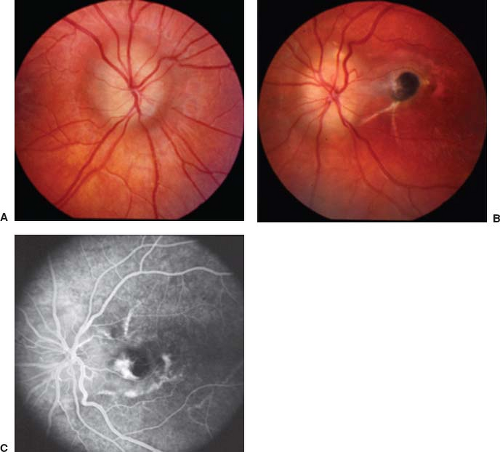 Figure 3.8 Subretinal neovascularization in a child with intrapapillary drusen. A: The right optic disc is moderately elevated and has blurred disc margins, but there is no hyperemia, there is no obscuration of the vessels crossing its surface, and the peripapillary retinal nerve fiber layer is not distorted. These features are consistent with anomalous elevation of the disc caused by buried drusen. B: The left optic disc also is elevated and several drusen can be seen within it. Temporal to the disc there is a large hyperpigmented area of subretinal neovascularization. C: In the arteriovenous phase of the fluorescein angiogram, there is diffuse staining of the left optic disc and there is both staining and leakage of dye from the area of subretinal neovascularization. (Courtesy of Drs. Sandra Brown and Monte del Monte.) |
Peripapillary subretinal neovascularization is a rare but well-documented complication in eyes with disc drusen that can cause temporary or permanent visual loss when it occurs in the macular region (Fig. 3.8). This phenomenon appears to occur more often in children than
in adults. Optimum management of this complication remains unclear. Both observation and photocoagulation of the area of neovascularization have been used.
in adults. Optimum management of this complication remains unclear. Both observation and photocoagulation of the area of neovascularization have been used.
 Figure 3.9 Optic disc drusen in a patient with retinitis pigmentosa. A: The optic disc is pale and there are drusen within the substance of the disc and at its margins. Note marked thinning of the retinal arteries. B: There is extensive pigment spicule formation in the mid-peripheral retina. |
Optic nerve head drusen usually are unassociated with any systemic, ocular, or neurologic conditions. They were once thought to be more common in patients with brain tumors and in patients with migraine headaches; however, the concurrence of brain tumors or migraine and optic disc drusen probably reflects the frequent and often expedited referral of patients with headaches and optic disc elevation. On the other hand, drusen occasionally occur in patients with retinitis pigmentosa, in which cases the drusen often are located at the disc margin in the superficial retina and the disc is neither elevated nor anomalous but is flat and waxy yellow (Fig. 3.9).
There is an association between disc drusen and angioid streaks. Using ultrasonography or OCT, disc drusen can be detected in about 20% of patients with pseudoxanthoma elasticum and in 25% of patients with angioid streaks with no pseudoxanthoma elasticum.
Optic disc drusen also may occur as part of the Riley–Smith syndrome of macrocephaly, multiple hemangiomata, and pseudopapilledema.
Anomalous Disc Elevation without Drusen
Not all anomalously elevated optic discs are associated with superficial or buried drusen. For example, the morning glory syndrome is associated with disc elevation, the superotemporal portion of a tilted optic disc usually is elevated, dysplastic discs may show some degree of elevation, and hypoplastic discs often have generalized elevation that may seem out of proportion to the size of the disc (Fig. 3.10). Thus it is essential that patients with elevated optic discs but with no clinical or imaging evidence of drusen not be automatically assumed to have true optic disc swelling.
Optic Nerve Hypoplasia
Optic nerve hypoplasia is the most common optic disc anomaly encountered in ophthalmologic practice. According to one study, it occurs in 1 in 2,287 live births. In another study from Sweden, it was present in 17.3/100,000 children and adolescents younger than 18 years of age. It may be unilateral or bilateral.
Clinical Features
Ophthalmoscopically, the hypoplastic disc appears as an abnormally small optic nerve head (Fig. 3.11). It may appear gray or pale and is often surrounded by a yellowish mottled peripapillary halo, bordered by a ring of increased or decreased pigmentation (“double-ring” sign), which facilitates recognition of the anomaly (Fig. 3.12). Optic nerve hypoplasia often is associated with tortuosity of the retinal veins.
Optic nerve hypoplasia is characterized histopathologically by a subnormal number of optic nerve axons with normal mesodermal elements and glial supporting tissue. The double-ring sign correlates to a normal junction between the sclera and lamina cribrosa, which corresponds to the outer ring, and the termination of an abnormal extension of retina and pigment epithelium over the lamina cribrosa, which corresponds to the inner ring.
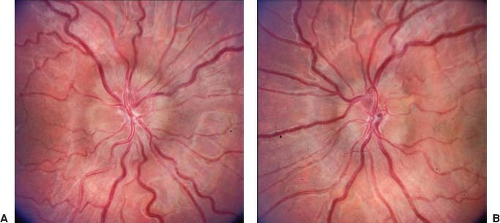 Figure 3.10 Anomalous optic disc elevation without drusen. The patient had no visual or systemic symptoms and a normal examination. A: The right optic disc is elevated, but it is not hyperemic nor is there any obscuration of the vessels crossing the disc surface. B: The left optic disc is also elevated. It also is smaller than normal. There were no drusen by either optical coherence tomography or B-scan ultrasonography. |
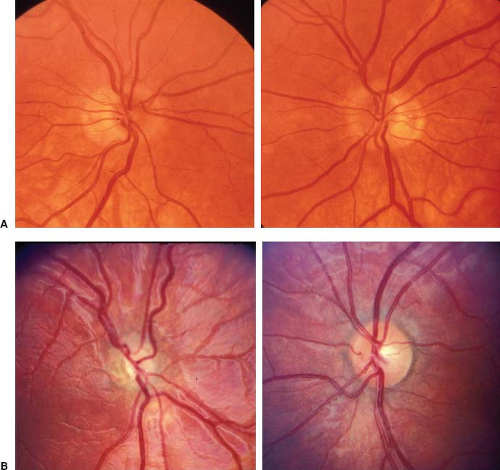 Figure 3.11 Optic nerve hypoplasia. A: Bilateral hypoplasia. Note classic double-ring sign. B: Unilateral hypoplasia. The right optic disc (left) is about half normal size and there is a prominent double-ring sign. The left disc (right) is normal in size and configuration. |
 Figure 3.12 Optic nerve hypoplasia. The optic disc is small and surrounded by a rim of variably pigmented tissue. |
Visual acuity in optic nerve hypoplasia ranges from 20/20 to no light perception, and affected eyes show localized visual field defects, often combined with generalized constriction. Because visual acuity is determined primarily by the integrity of the papillomacular nerve fiber bundle, it does not necessarily correlate with the overall size of the disc. The strong association of astigmatism with optic nerve hypoplasia warrants careful attention to correction of refractive errors. In addition, unilateral optic nerve hypoplasia may be associated with amblyopia, in which case occlusion therapy may result in visual improvement. Decreased vision associated with optic nerve hypoplasia should remain stable throughout the patient’s life unless another process is superimposed such as cataract formation or retinal disease such as a traction retinal detachment or peripheral retinal nonperfusion as occur in some patients. Thus, any patient with progressive visual loss in the setting of optic nerve hypoplasia should be evaluated for some other underlying cause such as an intracranial mass compressing the anterior visual pathway.
It is often difficult to distinguish between a normal and a hypoplastic disc; indeed, large optic discs can be axonally deficient, and small optic discs do not preclude normal visual function. Other variables also must be considered, including the size of the central cup, the percentage of the nerve occupied by axons (as opposed to glial tissue and blood vessels), and the cross-sectional area and density of axons. Furthermore, segmental forms of optic nerve hypoplasia (see below) affect only one sector of the disc and, thus, not produce a diffuse diminution in the size of the disc. As such, it would seem prudent to reserve the diagnosis of optic nerve hypoplasia for patients with small optic discs who have reduced vision or visual field loss with corresponding nerve fiber bundle defects.
Associated Endocrinologic Deficiencies
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


