7 Complications of Sinusitis
Indications
• Perifocal inflammation of facial soft tissues
• Chemosis, nasolacrimal stenosis
• Orbital abscess or phlegmon, optic nerve neuritis
• Mucopyocele
• Osteitis, osteomyelitis
• Meningitis, brain abscess
• Focal spread
Principles
Inflammatory invasions of soft tissues and bone beyond the borders of the paranasal sinuses are termed complications. They may involve adjacent structures or remote areas by superficial or hematogenous dissemination. In the past, radical eradications, mostly with external approaches, exposing the starting point at a paranasal sinus together with the healthy neighborhood were regarded as mandatory. Modern endoscopic surgery has changed the strategy: Sanitation of the focus by one of the standard operations described in Chapter 6 in facultative combination with an eventual neurosurgical or ophthalmological intervention supported by high-dosage antibiosis has proved successful. It must be stressed that early perifocal edema and phlegmon during childhood should only reluctantly be treated with surgery Fig. 7.1).

Fig. 7.1 Initial orbital complication from rhinitis in an infant showing a swollen and reddened upper lid and chemosis.
Operative Technique
Orbital Complications
Orbital complications are most frequently due to an aggressive infection of the ethmoid. Blockade of the maxillary and frontal sinuses gives rise to tailback of secretions, thus provoking mucoceles with diplopia or pain as presenting symptoms.
Chronic conjunctivitis, blepharitis, and epiphora can be caused by chronic rhinosinusitis with or without stenosis of the nasolacrimal duct. Ophthalmological examination including probing and irrigation of the duct and radiological diagnosis will then indicate conservative or eventually rhinosurgical treatment of the underlying disease, which means an endoscopic revision of the adjacent sinuses, and a microscopic dacryocstorhinostomy if necessary (see Chapter 6).
Rhinogenous orbital cellulitis and subperiostal abscess are regularly caused by invasive inflammation from the ethmoid through the lamina papyracea into the orbit. This proliferation is especially easy during childhood. The alarming symptoms of chemosis and orbital protrusion Fig. 7.2) are, therefore, generally addressed in infants by an initially conservative treatment under ophthalmological supervision over 24–36 hours before ethmoidectomy should become necessary.
In adults, this decision is facilitated by the evidence of chronic ethmoiditis (Fig. 7.3a–c) . Endoscopic total ethmoidectomy is carried out according to the technique described in Chapter 6. A limited resection of the lamina papyracea is added, and the localized abscess is opened by a vertical incision of the periosteum with a sickle knife. A mild and careful spreading with a small Blakesley forceps will completely empty the abscess cavity, which should be monitored, and if necessary this manipulation process should be repeated the next day under local anesthesia and endoscopic visualization. Mann et al. (1997) had to repeat the maneuver in 6 of 26 children with a periorbital abscess. The healing process may be supported by insertion of a soft strap of cotton for 1–2 days.

Fig. 7.2 Orbital complication from rhinosinusitis with periocular venous congestion, edema, and slight protrusio bulbi.
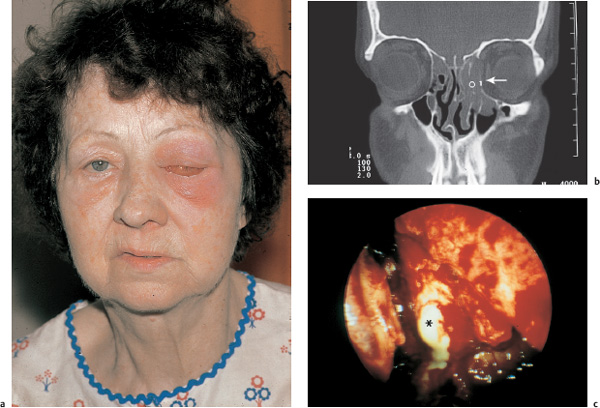
Fig. 7.3 a–c Advanced sinugenic orbital complication.
a The facial aspect with periocular inflammation, chemosis, and protrusio bulbi.
b Necrotizing maxilloethmoiditis (<) in the CT scan. The medial orbital wall (arrow) is eroded and deflected by a subperiosteal abscess.
c Incision of the prominent periorbita after ethmoidectomy releases the abscess (*).

Fig. 7.4 Severe lateroinferior displacement of the left eye due to frontoethmoidal sinusitis with orbital phlegmon.
Orbital invasion from frontal sinusitis, clinically suggested by the lateroinferior displacement of the eyeball Fig. 7.4), will be detected on CT. It will be addressed by a frontal sinusotomy, if possible, endoscopically, combined with an anterior ethmoidectomy and medial orbitotomy.
A deep retrobulbar abscess Fig. 7.5) originating from the posterior ethmoid may be drained endonasally, but the risk of injuring the optic nerve must be balanced against the higher expense but greater safety of a transcranial approach. A modified endoscopic Lothrop procedure has been recommended for cases with extension of inflammation into the orbit or cranial cavity (Wormald et al. 2003). Figure 7.6 a, b shows a pertinent case.
| Stage | Pathology |
| I | Preseptal cellulitis |
| II | Orbital cellulitis |
| III | Subperiostal abscess |
| IV | Orbital abscess |
| V | Cavernous sinus thrombosis |
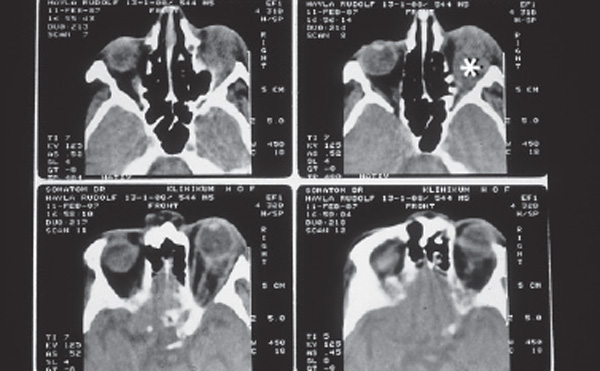
Fig. 7.5 Axial CT series showing a retrobulbar abscess (*) of dentogenic origin. The paranasal pneumatization appears unshadowed.
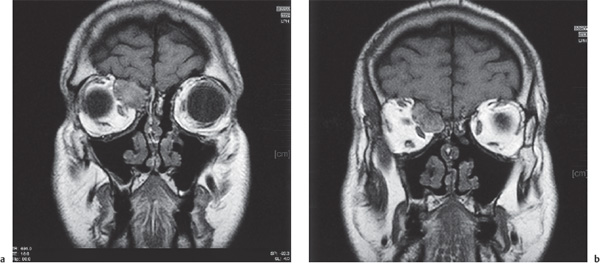
Fig. 7.6 a, b Sinugenic abscess starting from a deep supraorbital recess of the right frontal sinus, and invading the retrobulbar space and anterior cerebral fossa (MRI).
a Anterior coronal plane.
b Dorsal coronal plane behind the ocular plane. The patient had previous incomplete ethmoidectomy (T1-weighted MRI).
There are classifications of orbital complications (Chandler et al. 1970; Schramm et al. 1982; Kastenbauer 1992; Stammberger 1993) that assign gradual steps of therapy to certain entities. Table 7.1 shows the classification of Chandler. In the author’s experience, however, severe functional injury can occur unexpectedly from apparently innocent lesions. Too restrictive an attitude toward ESS, which is occasionally advocated by pediatricians who are not convinced of the safety of endoscopic interventions, can have, and in our experience has had, disastrous consequences. Rare bilateral orbital complications have been observed by Mitchell et al. 2002.
Isolated empyema of the sphenoid cavity is not rare–parietal headache is a leading symptom–but it often remains occult, thus masking optic nerve neuritis . The latter may be reversible (Postma et al. 1995), but can result in definite amblyopia. Figure 7.7 shows an example of an undiagnosed isolated bilateral sphenoiditis resulting in bilateral total blindness. Unfortunately, a complete endoscopic posterior ethmoidectomy and sphenoidectomy two days after an initial visual deficit did not help.
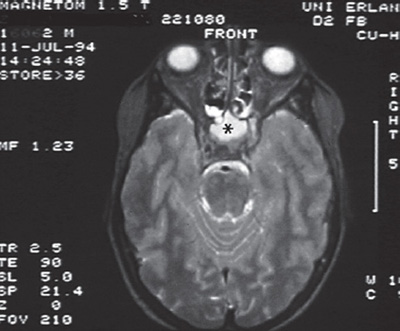
Fig. 7.7 T2-weighted MRI demonstrates an empyema of both sphenoid cavities (*) which caused bilateral amaurosis.

Fig. 7.8 Painless lateroinferior displacement of the right orbital contents due to a frontoethmoidal mucocele.
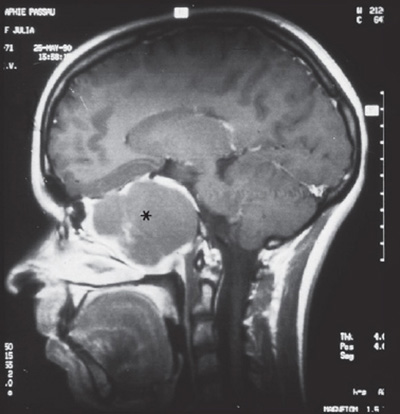
Fig. 7.9 Giant mucocele (*) of the sphenoid with displacement and arrosion of the anterior skull base in a CT scan before successful endoscopic marsupialization.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


