15 Complications of Otitis Media
The use of antimicrobial drugs in the management of otitis media has significantly decreased the incidence of complications from ear disease. Some studies demonstrate that antibiotic use has decreased the incidence between 0.13 and 2.3%, with variance likely because of the differences in access to care.1–4 While there has been progress made in eradicating these problems, the clinician needs to be familiar with the presentation and management of these complications.
Complications of otitis media and chronic ear disease are generally categorized as one of the following:
• Extratemporal extracranial,
• Intratemporal, and
• Intracranial (extradural, intradural).
Predisposing Factors
Complications can occur owing to several factors, some occurring simultaneously. Most commonly, complications occur in the setting of cholesteatoma but can also occur with otitis media. Several factors that lend to the development of complications are as following5:
• Virulence of the infecting organism.
• Antimicrobial therapy.
• Host resistance modulators (i.e., age, immune status, chronic disease).
• Anatomic barriers to spread.
• Drainage pathways, both natural and surgical.
Bacteriology
The microbiology differs when looking at complications related to acute and chronic infections. In acute infections, Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis are more common pathogens. In chronic infections, Proteus mirabilis, Pseudomonas aeruginosa, and Enterococcus are often seen. Proteus is cultured more frequently in cases of intratemporal and intracranial involvement, and notably in brain abscesses.3,6,7 For complicated clinical pictures, particularly with intracranial involvement, multiple drug regimens are used. As many as 50% of the patients will show no bacterial growth in culture and as a result empiric therapy needs to be instituted. Immunocompromised individuals are at a higher risk of developing complications in the setting of otitis media, given the reduced ability to defend against infection; this should direct interventions toward the sequelae and toward improving immune function whenever possible (e.g., diabetes control). Intratemporal and intracranial complications are more often seen in the presence of chronic otitis media and cholesteatoma compared with acute otitis media in a ratio of 9:1. The bacteriology is reflective of this chronic process, and often with multiple organisms isolated in culture.3,6,8 Factors that have been studied and increase the virulence of bacteria include:
• Biofilm formation9
• Beta-lactamase production
• Metalloprotease production (e.g., Pseudomonas)
• Colony swarming (e.g., Proteus)
• Lipopolysaccharide (e.g., Proteus)
• Motility (e.g., Pseudomonas)
• Capsule formation (e.g., bacteroides, S. pneumoniae)
Anatomic Factors and Pathways of Spread
The possible routes of spread of infection are as follows:
• Direct extension through bone.
• Traversing the venous channels between bone and dura mater, including those of the haversian system.
• Variations in normal anatomic pathways.
• Traumatic defects.
• Periarteriolar spaces of Virchow-Robin to access brain parenchyma.
Signs and Symptoms
Concerning signs and symptoms suggesting a complication include the following in the setting of otologic disease:
• Constitutional symptoms (fever, generalized malaise, and irritability).
• Postauricular edema and erythema.
• Ear pain out of proportion to physical findings.
• Persistence of purulent otorrhea despite treatment beyond 2 weeks.
• Fetid purulence suggestive of an anaerobic process.
• Meningismus.
• Papilledema.
• Vertigo.
• Altered sensorium.
Diagnostic Imaging
Diagnostic imaging should be directed toward the most appropriate means of looking at the extent of disease based on clinical suspicions. In the setting of suspected or identified complications from otitis media, high-resolution computed tomography (CT) scanning of the temporal bone, neck, and/or brain may be used with or without contrast as indicated. The need for bony detail is important from a diagnostic and planning standpoint in complicated clinical pictures. The use of contrast may be needed in looking at vascular structures, signs of abscess, involvement of the dura mater, and involvement of the brain parenchyma. Magnetic resonance imaging (MRI) can give complementary and important imaging as well; soft-tissue detail and magnetic resonance venography (MRV) imaging can increase the ability to detect the primary and concomitant complications. Given that 60% of the patients can present with multiple complications and that the overall postantibiotic era mortality ranges from 7 to 25%, a thorough investigation should be used.3,10
Extratemporal Extracranial Complications
Postauricular Mastoid Abscess
The postauricular abscess is a common extratemporal complication of mastoiditis. The infection extends from the mastoid to the subperiosteal space, either by direct extension subsequent to bone destruction or by phlebitis and periphlebitis of mastoid veins. It is most often seen accompanying acute or coalescent mastoiditis in very young children. The cribriform area of mastoid exists as a series of open channels between the interior of the mastoid and the cortex in the new born. Until these channels have closed, infection can pass directly from the mastoid to the subperiosteal space in these very young children.
Diagnosis
The diagnosis can be made when seeing a protruding auricle that is downward and laterally displaced, and the presence of a fluctuant, erythematous, tender area below the ear (Fig. 15.1). In the early stages, if fluctuation is not obvious, the clinician should consider imaging studies, such as a contrast-enhanced CT, to document the presence of air within the soft tissue or an abscess cavity with its capsule.
Management
Drainage of this abscess is recommended along with antibiotic therapy. The evacuation of middle ear disease and placement of pressure equalizing (PE) tubes are also recommended. If coalescent mastoiditis is present, mastoidectomy is usually performed as well to remove infected material seeding this area.
Bezold Abscess
A Bezold abscess is a condition caused by a perforation in the bony plate forming the inner surface of the tip of the mastoid. It occurs presumably in cases in which the tip cells are especially large, the bony plate forming the inner or medial wall of the tip is very thin, and the outer cortex is thick. Pus escaping through the thin bone medially traverses the neck downward beneath and deep to the sternomastoid or may be confined between layers of the deep cervical fascia.

Figure 15.1 Postauricular view of coalescent mastoiditis and abscess. Note the left pinna has been pushed laterally and inferiorly (arrow) as compared with the right pinna.
Diagnosis
A CT scan with contrast is often used to identify or rule out a mastoid source when faced with an abscess in this location.
Management
The recommended treatment is PE tube placement, mastoidectomy, removal of any associated granulation tissue, and drainage of the abscess. Open incision and drainage of the abscess is done through a transcervical approach. Culture-directed antibiotics are also used to address the disease.
Other Abscesses
Temporal root abscesses may form and manifest in the soft tissues above and even anterior to the auricle. These can become infected and form an abscess from suppuration that involves the cells of the zygomatic root of the mastoid (temporal root of the zygoma).
Less common abscesses may also be seen. These include meatal abscesses (Luc), behind the mastoid (Citelli), parapharyngeal, and retropharyngeal abscess. Treatment of these abscesses generally requires surgical drainage and antibiotic therapy depending on the manifestation and extent of disease.
Intratemporal Extracranial Complications
Mastoiditis
The temporal bone is intimately associated with the middle ear space by its connection through the aditus ad antrum. Because of the continuity, all patients with otitis media exhibit some degree of mastoid inflammation. Fluid collection or thickening of the mucosa lining the air cells is diagnostic of mastoiditis.
The progression of otitis media to coalescent mastoiditis follows a sequence. Otitis media leads to inflammation of the mastoid and reduced aeration. This leads to venous stasis, local acidosis, and dissolution of calcium from the bony septae. Osteoclastic activity in the inflamed periosteum softens and removes the bony partitions, causing the small air cells to coalesce into a larger cavity and forming coalescent mastoiditis.
Histologic examination shows that areas of coalescent bone erosion are combined with adjacent areas of bone deposition. As the acute inflammation subsides, the healing processes replace the mucoperiosteum with maturing granulation tissue. Fibrosing osteitis occurs in the areas of bone destruction, which, owing to healing, results in the production of dense, compact bone. Hence, chronic mastoiditis results in a sclerotic, poorly aerated mastoid cavity.
Acute Coalescent Mastoiditis
Classically, acute coalescent mastoiditis forms approximately 2 weeks after the onset of otorrhea. The hallmark symptom triad of acute mastoiditis is otalgia, postauricular pain, and fever. Erythema, edema, and tenderness over the mastoid may be seen. Sagging of the posterosuperior deep meatal wall can result from thickening of the periosteum adjacent to the antrum. In adults, mastoid tenderness is over the tip of the mastoid process, but in children with incomplete pneumatization, the tenderness is more over the fossa mastoidea near the antrum.
Diagnosis
Temporal bone CT (Fig. 15.2) is the diagnostic test of choice to detect coalescent mastoiditis. Depending on the clinical presentation, other diagnostic tests to rule out other complications such as intracranial complications may be needed.
Treatment
Placement of PE tubes, antibiotics, and mastoidectomy are generally accepted forms of treatment. Treatment with postauricular puncture drainage has also been recommended in lieu of mastoidectomy11 or to forego mastoid surgery in selected patients (older than 6 months and without intracranial complication). However, delaying mastoidectomy or other mastoid drainage may extend hospitalization.12 This continues to be an area of debate.
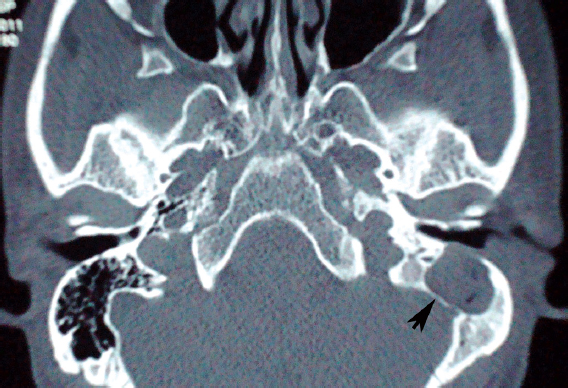
Figure 15.2 Axial computed tomography scan without contrast showing left coalescent mastoiditis. In the left mastoid, there is inflammation and loss of normal bony structure, consistent with coalescent mastoiditis (arrowhead).
Acute Mastoiditis
Acute mastoiditis can occur rarely in a well-aerated tympanic cavity and normal appearing tympanic membrane. This has been termed masked mastoiditis and is attributed to inadequate antibiotic management of acute otitis media. The clinical course is more insidious than that of classical coalescent mastoiditis. The presenting otologic symptoms can be vague and atypical; however, intracranial complications may occur with relatively high frequency.13
Diagnosis
CT can demonstrate mastoid inflammation, which may be focal in nature.
Management
PE tube placement, culture-directed antibiotics, and mastoidectomy should be considered. The goal of surgery is to evacuate any purulent material, debride necrotic bone, and thus prevent further progression of disease. Any concomitant complications should also be addressed.
Apicitis
Petrous apicitis is inflammation of the petrous temporal bone. It occurs generally in pneumatized petrous bone, with the exception of the acute fulminant osteomyelitis seen in infants.
Deep-seated pain and aural discharge are the two most constant symptoms of this condition. Involvement of a posterior group of cells causes the pain to be in the occipital, temporal, or parietal areas, whereas anterior petrositis causes pain to be localized to frontal and retro-orbital regions. Gradenigo syndrome (the triad of diplopia, retrobulbar pain, and persistent otorrhea) is associated with this disease. Involvement of cranial nerve VI passing through Dorello canal leads to diplopia from an abducens palsy. Other less common symptoms are facial nerve paresis, recurrent vertigo, and low-grade fever.
Diagnosis
The diagnosis is based on a high index of clinical suspicion and confirmed by CT of the temporal bone.
Management
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


