Purpose
To quantitatively characterize the ultrasound biomicroscopy (UBM) configurations of the peripheral anterior chamber (AC) in primary angle closure (PAC) and its suspects and to evaluate the diagnostic performance of the UBM parameters to differentiate PAC/PAC suspects in a population-based setting.
Design
Cross-sectional study.
Methods
A random 461 of 4632 residents 40 years or older on a southwest island in Japan underwent UBM under light and dark conditions.
Results
Of the 374 eligible randomly sampled residents (after excluding 87 with a history of intraocular surgeries, ocular trauma, or iritis; a physical or mental disability making the UBM measurement difficult; or refusal to undergo UBM measurements), reliable UBM images were obtained in 301 right eyes (80.4%). In 45 eyes with PAC/PAC suspects compared to 256 with nonoccludable angles, the angle-opening distance (AOD), trabecular-iris angle (TIA), and trabecular-ciliary process distance (TCPD) under light and dark conditions were smaller ( P < .001), while the iris thickness was smaller only under dark conditions ( P = .040). Dark-light changes in the AOD and TIA were significantly smaller in the PAC/PAC suspects than in the nonoccludable angles ( P < .03); the iris thicknesses did not differ significantly between them. Areas under the receiver operating characteristic curves of the AOD at 500 μm from the scleral spur (AOD500) and TIA in light were 0.94, suggesting these parameters were good for differentiating PAC/PAC suspects. The ideal cutoff values for the AOD500 and TIA under light conditions were 0.17 mm (sensitivity, 0.82; specificity, 0.96) and 15.2 degrees (sensitivity, 0.83, specificity, 0.93), respectively.
Conclusions
Eyes with PAC/PAC suspects had shallow ACs, anteriorly located ciliary bodies, and smaller dark-light changes in the peripheral AC depth, while the iris thickness was similar to that in eyes with nonoccludable angles. The peripheral AC depth under light conditions could most clearly differentiate PAC/PAC suspects from nonoccludable angles.
Eyes with primary angle closure (PAC) tend to share certain biometric characteristics including a shallow central anterior chamber (AC), a thick and anteriorly positioned lens, a small corneal diameter with a small radius of curvature, and a short axial length. Since occlusion of the peripheral AC angle is the primary cause of PAC, the anatomic configurations around the peripheral AC including the iris root and the ciliary body should play an important role in the development of PAC.
Ultrasound biomicroscopy (UBM) allows observation of not only the peripheral AC angle but also the iris and ciliary body. Using UBM, hospital-based studies showed that eyes with PAC/PAC suspects (or occludable angle) had a shallow peripheral AC and anteriorly located ciliary body compared to eyes with open angles. However, it is conceivable that patients with PAC/PAC suspects in a hospital-based setting are more likely to have symptoms, more definitively shallow ACs, or a history of acute or subacute elevation of intraocular pressure (IOP). In previous population-based studies, UBM was performed only in participants selected according to predetermined conditions. No study has compared UBM findings between PAC/PAC suspects and open angles in the population-based settings.
We recently conducted the Kumejima Study, a population-based survey on a southwest Ryukyus (Okinawa) island of Japan. We performed UBM in a random sample (10%) of 4632 residents aged 40 years or older. The mean values and distribution of the UBM parameters were reported elsewhere. The aims of this study are to quantitatively characterize the peripheral AC configurations of eyes with PAC/PAC suspects and to evaluate the diagnostic performance of the UBM parameters to differentiate PAC/PAC suspects in a population-based setting.
Subjects and Methods
The Kumejima Study, conducted between May 2005 and August 2006, was a population-based epidemiologic survey and followed the tenets of the Declaration of Helsinki and regional regulations and was approved by the ethics board of the regional council. All participants provided written informed consent before the examinations. All eligible residents (4632 subjects) aged 40 years or older were encouraged to participate. Kumejima had 5249 residents aged 40 years or older in 2005 according to the official household registration database. After excluding 617 residents who died, moved, or could not be located during the study period, 4632 residents were eligible for the study. For the UBM study, 10% of the residents (461 subjects) were randomly sampled using the random number method because of limited examination time.
In the screening examination, refraction was measured using an autorefractometer (ARK-730, Topcon, Tokyo, Japan); IOP was measured 3 times using a Goldmann applanation tonometer and the median value was recorded. The peripheral anterior chamber depth (ACD) was scored according to the van Herick method and the gonioscopic findings were scored according to Shaffer’s grading system using a Goldmann 2-mirror lens by experienced ophthalmologists. Based on gonioscopic findings, PAC and PAC suspects were identified. If the posterior trabecular meshwork was not visible during static gonioscopy in at least three quarters of the angle circumference in primary gaze without manipulation or indentation, the angle was classified as occludable. An eye was classified with PAC when an eye with an occludable angle had 1 or more of the following: an IOP exceeding 21 mm Hg; peripheral anterior synechiae (PAS) reaching the scleral spur or beyond; a history of an acute IOP elevation, including the presence of iris atrophy, glaukomflecken, dilated nonreactive pupils, or a previous diagnosis of PAC according to the combination of the subject’s reliable statement and the objective signs in their eyes. In some of the cases, we could confirm the history in their medical records. If an eye that was not classified as having an occludable angle had PAS in an area of a narrow chamber angle of Shaffer grade 2 or less, the eye also was classified with PAC and secondarily added to occludable angle. When an eye with an occludable angle was not classified with PAC, the eye was classified as a PAC suspect.
UBM measurements were performed using UD-1000 (Tomey, Aichi, Japan) with a 40-MHz transducer probe at the 12-o’clock (superior), 3-o’clock (nasal), 6-o’clock (inferior), and 9-o’clock (temporal) positions of the right eye of each subject in the supine position by 1 of 2 experienced ophthalmologists (I.H., C.U.). After topical anesthesia was applied, an eye cup containing hydroxyethyl cellulose and physiologic saline was mounted on the globe, and the transducer was applied gently to the limbal area with care to avoid compression of the globe. UBM assessments were carried out in room light (about 1400 lux, measured with an illuminometer [IM-2D, Topcon]) and repeated in the same manner 3 minutes after the room was darkened to about 3 lux. Variations in accommodation were minimized by fixation to targets located on the ceiling with a standard distance. The lateral and axial resolutions were both 50 μm. A 9 × 6-mm field was imaged and transferred to a personal computer for analysis.
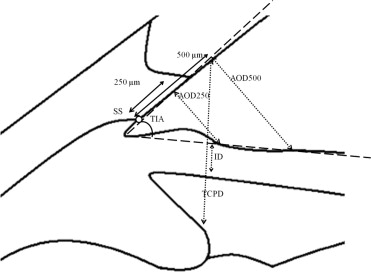
The UBM parameters evaluated in the current study had been defined by Pavlin and associates. The images transferred to a personal computer were analyzed using originally developed software for image analysis. UBM images were calibrated as 414 × 276 pixels and 9 × 6 mm in size. On a UBM image magnified on the monitor of a personal computer, the scleral spur was first identified by an examiner and the circular lines with the diameter of 250 and 500 μm centered on the scleral spur were automatically drawn. According to the circles, the following points were identified by the examiner and the distance and area were automatically determined by the software. Among the parameters described by Pavlin and associates, the angle-opening distance of 250 or 500 (AOD250, AOD500, respectively) was defined as the distance between the posterior corneal surface and the anterior iris surface measured on a line perpendicular to the trabecular meshwork 250 or 500 μm, respectively, from the scleral spur; the trabecular-iris angle (TIA) was defined as the angle measured with the apex in the iris recess and the arms of the angle passing through a point on the trabecular meshwork 500 μm from the scleral spur and the point on the iris perpendicularly opposite; and the trabecular-ciliary process distance (TCPD) was defined as the length of the line extending from the corneal endothelium 500 μm from the scleral spur perpendicularly through the iris to the ciliary process. The thickness of the iris was measured on the same line ( Figure 1 ). Reproducibility of the UBM parameters determined with this software was preliminarily evaluated: the coefficient variation of AOD250, AOD500, TIA, TCPD, and the iris thickness in the 5 UBM images serially obtained in 10 subjects averaged 12.5%, 8.9%, 9.5%, 8.6%, and 10.3%, respectively (unpublished data), which were almost comparable to that in a previous report in which the parameters were manually determined.
Data Analysis
Demographic data and the UBM parameters were compared between eyes with PAC/PAC suspect and nonoccludable angle eyes or between eyes with PAC and those that were PAC suspect using the unpaired t test and Fisher exact test. Changes in the UBM parameters between light and dark conditions were compared using the paired t test. A P value less than .05 after the Bonferroni correction for multiple comparisons was supposed to be significant. The performance of the UBM parameters in differentiating PAC/PAC suspect from nonoccludable angle eyes was evaluated based on the receiver operating characteristic (ROC) curve and the area under the curve (AUC). Data analyses were performed using SPSS 15.0J for Windows (SPSS Japan Inc, Tokyo, Japan).
Results
Reliable UBM images were obtained in 301 right eyes (80.4%) of the 374 eligible subjects after excluding 87 with a history of intraocular surgeries (cataract surgery in 59 eyes, laser iridotomy in 1 eye, and trabeculectomy in 1 eye), ocular trauma (4 eyes), or iritis (1 eye); a physical or mental disability making the UBM measurement difficult (15 eyes); or refusal to undergo UBM measurements (4 before and 2 during the UBM measurements) from the randomly sampled 461 subjects ( Figure 2 ). Of the 301 eyes, 8 (2.7%), 37 (12.3%), and 256 (85.0%) eyes were diagnosed with PAC, as PAC suspects, and with nonoccludable angles, respectively. The diagnosis of 8 eyes with PAC was made based on the presence of PAS (7 eyes) and the combination of PAS and IOP exceeding 21 mm Hg (1 eye). No eye had a history of an acute episode of PAC or laser iridotomy, because eyes with history of surgery or laser procedures had been excluded from the current study.
Mean values of the UBM parameters in different age groups are shown in Table 1 . All parameters were significantly negatively correlated with age ( P < .001, Pearson’s correlation coefficient), suggesting that older subjects had narrow peripheral angle, anteriorly located ciliary body, and thin iris. In Table 2 , the comparisons of the UBM parameters between the PAC/PAC suspects and nonoccludable eyes are summarized. Subjects with PAC/PAC suspect were older ( P < .001, unpaired t test) and had more hyperopic refractive error ( P < .001) than nonoccludable angle eyes, and women tended to be more prevalent ( P = .052), while IOP did not differ significantly ( P = .560). Between 45 eyes with PAC/PAC suspect and 256 with nonoccludable angles, the AOD250, AOD500, TIA, and TCPD under light and dark conditions were significantly smaller in PAC/PAC suspect than in nonoccludable angles ( P < .001 for all comparisons by the unpaired t test), while the iris thickness showed no significant intergroup difference ( Tables 3 and 4 ). Between 8 eyes with PAC and 37 eyes of patients who were PAC suspects, no UBM parameters differed significantly ( P > .1 for all comparisons), with the exception that the AOD250 under light conditions was significantly greater in PAC suspects than in those with PAC ( P = .001).
| Age (Years) | AOD250 (mm) | AOD500 (mm) | TIA (Degrees) | TCPD (mm) | ID (mm) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Light | Dark | Light | Dark | Light | Dark | Light | Dark | Light | Dark | |
| 40–49 | 0.203 ± 0.098 | 0.157 ± 0.090 | 0.349 ± 0.147 | 0.269 ± 0.131 | 28.1 ± 10.1 | 22.0 ± 9.4 | 0.838 ± 0.162 | 0.839 ± 0.145 | 0.418 ± 0.054 | 0.467 ± 0.059 |
| 50–59 | 0.173 ± 0.080 | 0.126 ± 0.069 | 0.287 ± 0.138 | 0.209 ± 0.107 | 23.7 ± 9.4 | 17.6 ± 8.3 | 0.777 ± 0.167 | 0.764 ± 0.151 | 0.422 ± 0.055 | 0.470 ± 0.058 |
| 60–69 | 0.145 ± 0.071 | 0.107 ± 0.056 | 0.215 ± 0.100 | 0.157 ± 0.085 | 18.4 ± 8.0 | 13.5 ± 7.1 | 0.703 ± 0.156 | 0.688 ± 0.134 | 0.404 ± 0.048 | 0.456 ± 0.058 |
| 70–79 | 0.141 ± 0.067 | 0.107 ± 0.071 | 0.198 ± 0.098 | 0.154 ± 0.093 | 17.2 ± 8.2 | 13.4 ± 7.7 | 0.682 ± 0.134 | 0.673 ± 0.109 | 0.406 ± 0.051 | 0.438 ± 0.065 |
| 80- | 0.136 ± 0.054 | 0.130 ± 0.070 | 0.193 ± 0.067 | 0.168 ± 0.080 | 16.7 ± 5.6 | 14.4 ± 6.4 | 0.677 ± 0.096 | 0.702 ± 0.128 | 0.387 ± 0.053 | 0.421 ± 0.071 |
| Total | 0.167 ± 0.084 | 0.127 ± 0.076 | 0.267 ± 0.138 | 0.202 ± 0.116 | 22.2 ± 10.0 | 17.0 ± 8.9 | 0.755 ± 0.165 | 0.748 ± 0.152 | 0.412 ± 0.053 | 0.457 ± 0.062 |
| Occludable Angle | Nonoccludable Angle | P Value a | |||
|---|---|---|---|---|---|
| PAC | PACS | PAC+PACS | |||
| No. eyes | 8 | 37 | 45 | 256 | |
| Men/women | 6/2 | 10/27 | 16/29 | 133/123 | .052 b |
| Age (years) d | 64.0 ± 13.5 | 70.5 ± 8.2 | 69.3 ± 0.5 | 57.3 ± 12.4 | <.001 c |
| Refractive error (diopters) d | 1.7 ± 0.8 | 1.0 ± 1.5 | 1.1 ± 1.4 | 0.0 ± 1.9 | <.001 c |
| Intraocular pressure (mm Hg) d | 15.6 ± 3.2 | 15.0 ± 3.0 | 15.1 ± 3.0 | 14.8 ± 2.8 | .560 c |
a P value for comparison between 45 eyes with occludable angles and 256 eyes with nonoccludable angles.
| Occludable Angle | Nonoccludable | P Value b | ||||
|---|---|---|---|---|---|---|
| P Value a | PAC+PACS | |||||
| AOD250 (mm) | PAC | 0.043 ± 0.025 | .001 | 0.087 ± 0.037 | 0.181 ± 0.082 | <.001 |
| PACS | 0.095 ± 0.033 | |||||
| AOD500 (mm) | PAC | 0.106 ± 0.047 | .58 | 0.116 ± 0.045 | 0.293 ± 0.132 | <.001 |
| PACS | 0.118 ± 0.045 | |||||
| TIA (degrees) | PAC | 9.6 ± 4.2 | .633 | 10.3 ± 3.9 | 24.2 ± 9.3 | <.001 |
| PACS | 10.4 ± 3.9 | |||||
| TCPD (mm) | PAC | 0.582 ± 0.059 | .111 | 0.622 ± 0.112 | 0.777 ± 0.163 | <.001 |
| PACS | 0.632 ± 0.119 | |||||
| ID (mm) | PAC | 0.421 ± 0.056 | .519 | 0.407 ± 0.052 | 0.413 ± 0.053 | .525 |
| PACS | 0.406 ± 0.052 | |||||
a P value for comparison between 8 eyes with PAC and 37 eyes with PACS (unpaired t test).
b P value for comparison between 45 eyes with occludable angles (ie, PAC and PACS) and 256 eyes with nonoccludable angles (unpaired t test).
| Occludable Angle | Nonoccludable | P Value b | ||||
|---|---|---|---|---|---|---|
| P Value a | PAC+PACS | |||||
| AOD250 (mm) | PAC | 0.056 ± 0.035 | .435 | 0.065 ± 0.036 | 0.138 ± 0.076 | <.001 |
| PACS | 0.067 ± 0.036 | |||||
| AOD500 (mm) | PAC | 0.094 ± 0.029 | .38 | 0.085 ± 0.041 | 0.223 ± 0.113 | <.001 |
| PACS | 0.083 ± 0.043 | |||||
| TIA (degrees) | PAC | 8.4 ± 2.4 | .343 | 7.6 ± 3.5 | 18.7 ± 8.5 | <.001 |
| PACS | 7.4 ± 3.7 | |||||
| TCPD (mm) | PAC | 0.645 ± 0.115 | .828 | 0.636 ± 0.117 | 0.768 ± 0.149 | <.001 |
| PACS | 0.635 ± 0.119 | |||||
| ID (mm) | PAC | 0.426 ± 0.046 | .407 | 0.440 ± 0.059 | 0.460 ± 0.062 | .040 |
| PACS | 0.443 ± 0.061 | |||||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


