8
Cognitive-Behavioral Therapy with Applied Relaxation
This chapter describes the method of applied relaxation, which forms an integral part of a cognitive-behavioral treatment protocol. The treatment also includes cognitive restructuring, sound enrichment, hearing tactics, sleep management, and relapse prevention. The rationale behind the treatment approach and the effects of protocol are reviewed. Practical advice on how to implement applied relaxation with tinnitus patients is given.
Applied Relaxation as Part of a Cognitive-Behavioral Approach to Tinnitus
Cognitive-behavioral therapy (CBT) is a relatively brief psychological treatment approach directed at identifying and modifying maladaptive behaviors and thoughts by means of behavior change and cognitive restructuring. The focus is on applying behavioral and cognitive techniques in real-life settings and testing out coping strategies for facing difficult situations. Hence CBT concerns not only thinking differently about experiences but also changing habits and finding ways to master difficult situations (like silence for some tinnitus sufferers). One coping strategy is applied relaxation. Applied relaxation, as presented in this chapter, is derived from various applications of relaxation, but it is more of a psychological than a physiotherapeutic treatment method. The use of relaxation in CBT has a long history, and its efficacy has been supported by experimental studies (Öst, 1987). Unlike relaxation done by physiotherapists, the patient must use the applied relaxation method outside the therapist’s office. In cases where there are clear problems with the neck and so on, then the referring physician and a physiotherapist should be consulted.
Applied relaxation is a method by which the patient is taught to relax quickly and to use self-control over bodily and mental sensations (e.g., stress). The purpose of this relaxation is not to reduce tinnitus but to deal with the consequences of it. The goal is to obtain a balanced and relaxed state of mind and to break a vicious cycle of tension, leading to more focus on tinnitus. Learning the applied relaxation technique is usually the first task that the patient is given in our treatment protocol, and the technique has been used successfully since the early 1980s (Lindberg et al, 1984). The technique is taught in stages over four to six sessions, and the last stage is practiced for the rest of the treatment once it is mastered. Normally, four components are included: (1) progressive relaxation (tense and release body parts), (2) release-only relaxation without tension, (3) cue-controlled relaxation (controlled breathing), and (4) rapid relaxation in everyday situations. Imagery techniques (e.g., imagining a beach) are taught in association with the relaxation training. Although there has been little tinnitus research to evaluate differences in effectiveness between different forms of relaxation in treating tinnitus, there are some indications that applied relaxation is slightly superior to other alternatives such as progressive relaxation (Davies et al, 1995).
Relaxation is relatively easy to learn, and it can be meaningful to learn this skill apart from the effects related to tinnitus. Thus applied relaxation can be helpful for dealing with stress and tension, working on other tinnitus-related issues such as insomnia, and confronting problems less related to tinnitus such as headache and back pain. However, although applied relaxation can be beneficial in many circumstances, there are some caveats. First, there are some people for which relaxation, at least initially, can be a very terrifying experience. Examples of relaxation-induced panic have been reported in the literature (Heide and Borcovec, 1983). Fortunately, this is very rare. We inform our patients about the potential adverse sensation they might experience, so that feelings of elevated anxiety will not come as a surprise. In addition, we know from the literature that it can be a bad idea to try to relax under severe stress because the opposite may occur: the patient may feel more tense than when he or she started (Wegner et al, 1997). The solution lies in gradually approaching difficult situations and learning first to relax under easier conditions. In this context the therapist needs to be attentive to motivating factors because the patient may find that there is no need to practice relaxation when he or she feels relaxed. Here, the therapist may find it useful to compare relaxation with the effects of exercise, where it is important to start gradually to build up physical strength, and where it s not useful to begin exercising by running a marathon.
There are, of course, indications when applied relaxation is more or less likely to lead to an improvement (Linton, 1982). For patients with signs of stress, muscular tension, and anxiety, applied relaxation is likely to be of help, but then resting and a change of environment also are beneficial. Also, some patients, despite being given a rationale for this treatment, may search for an alternative treatment, believing that tinnitus will disappear, and that applied relaxation is therefore not needed to make a difference.
One common misunderstanding of our approach is that relaxation is equivalent to doing nothing and resting. This has to be corrected when describing the rationale of the treatment. Applied relaxation is described as an active coping technique, and the patient is gradually taught to quickly relax and to use self-control over bodily and mental sensations (e.g., stress, irritation, worry, anger). The aim is not to reduce tinnitus but to control its effects. Metaphors used to illustrate this include the runner at the starting block. If she is too tense, she will jump the gun; if she is too relaxed, she will have a slow start. Ideally, being in control of mental and bodily sensations while still focused on the task at hand is what is needed. Another metaphor (provided by a patient) is the man who is aiming with his rifle with the intention to shoot. If he is too tense, he will miss, but if he is too relaxed, he may also miss the target. Therefore, contrary to what is usually meant by being relaxed (e.g., on the sofa in front of the television), applied relaxation is not something to do while lying down, although this form of relaxation can be useful as well. Another important aspect of applied relaxation is that it is important not to restrict relaxation to the person’s own physical and mental sensations but also to include environmental aspects. The environment where the patient applies relaxation greatly influences the outcome. In fact, many patients tell us that they are relaxed in some situations (e.g., while on vacation), and this information is used to encourage the patient to work for incorporating some “holiday atmosphere” into daily struggles to cope with tinnitus. Therefore, in applied relaxation the analysis of difficult situations and situations in which it is easier to relax is important.
This chapter presents an overview of our CBT program. There are several components to it, but the focus here is on applied relaxation.
Cognitive-Behavioral Approach to Tinnitus
The cognitive-behavioral approach to tinnitus management is based on certain premises derived from CBT for other conditions, such as anxiety and depression (Persons et al, 2001), as well as research conducted with patients afflicted with somatic conditions, such as chronic pain (Philips and Rachman, 1996) and insomnia (Morin, 1993).
The following basic assumptions guide our practice and the treatment protocol described in this chapter.
Tinnitus can be viewed, at least partly, in terms borrowed from learning theory. Hallam et al’s (1984) psychological model of tinnitus suggested that the natural history of tinnitus is characterized by the process of habituation (a learning theory term). Hence factors that impede habituation (e.g., arousal and novelty) are important to investigate to understand tinnitus. More recently, Jastreboff (2000) developed a theory that relies on classical conditioning, (the notion being that tinnitus can be conditioned (associated) with fear (and other negative emotions), and that this conditioning does not necessarily need to occur on a conscious level.
The severity of tinnitus can be understood within a stress-diathesis model (Andersson and McKenna, 1998; Schulman, 1995). This model assumes that a “vulnerable” person may develop tinnitus distress following the onset of relatively soft tinnitus. A more stress-tolerant person may bear higher degrees of tinnitus before seeking help. It is necessary to point out that vulnerability does not necessarily connote “psychiatric disturbances.” In fact, in the clinic we sometimes meet highly successful individuals with remarkable achievements in life, and without any pretinnitus psychiatric or somatic problems, for whom tinnitus becomes the major stressor initiating problems at work and in the family.
Thoughts and beliefs about tinnitus are important and can strengthen the association between negative emotions and tinnitus. The meaning attached to tinnitus influences how annoying it is perceived to be. Sounds are perceived and processed by conscious and feeling individuals. In addition, from clinical reports we know that many tinnitus patients report difficulties with concentration. Hence it can be suspected that tinnitus demands attention. For example, in a recent experimental study we found that background sounds (white noise) were perceived as lower when attention was focused on tinnitus than when it was not (Andersson, 2002).
Finally, an important assumption is the simple notion that what is good for life in general is usually good for coping with tinnitus. This includes living a healthy life with respect to food, exercise, social contacts, and so on. One related aspect is that it may be important for the tinnitus patient to establish regular routines in life. Before the onset of tinnitus, it might have been possible to have irregular working hours and sleep patterns, but often adaptation to tinnitus requires regular habits, in particular when it comes to sleep.
In the context of changing beliefs and thoughts, it is important to work toward acceptance of tinnitus and to foster the idea that tinnitus is not worth all the attention it gets. The idea that acceptance of tinnitus is something to work for is not easy to convey. Some patients have had the bad experience of health care personnel telling them that tinnitus is something they have to learn to live with. For many patients this is true when it comes to the sensation of tinnitus, but it is not true when it comes to the accompanying annoyance and distress. What we tell our patients is that we want to give them tools to deal with the consequences of tinnitus and that this is a way to be able to accept that tinnitus seldom disappears by itself. We need to help our patients distinguish between useless attempts to try to control something that cannot be controlled (as often is the case with loud tinnitus), and successful ways of controlling their reactions and emotions when faced with difficulties (in this context, the consequences of tinnitus). So far, the notion of acceptance of tinnitus has received little attention in the literature, but in the day-to-day clinical practice this is something many of us work for. Some work has been done in the field of chronic pain, an area bearing several resemblances to tinnitus (Møller, 1997). For example, McCracken (1998) found that greater acceptance of pain was associated with reports of lower pain intensity, less pain-related anxiety and avoidance, and several other indicators of well-being in relation to chronic pain, and this was not a function of pain intensity. Experimental studies seem to support this notion (Hayes et al, 1999a). According to this way of thinking, acceptance of tinnitus can be defined as acknowledging that one has tinnitus, giving up unproductive attempts to control it, acting as if tinnitus does not necessarily imply disability, and being able to commit one’s effort toward living a satisfying life despite the problem (adapted from McCracken, 1998). According to Hayes et al (1999b), acceptance is often interpreted by the patient to mean tolerance, which is an entirely different thing, or resignation, in which the client accepts defeat. Acceptance has more to do with choosing the direction in one’s life.
Treatment Protocol
Basically, the application of CBT for tinnitus follows standard methods developed for other problems such as anxiety and pain (Hawton et al 1989; Philips and Rachman, 1996). Hence homework assignments between therapy sessions are scheduled, and a rationale is presented for each treatment component. In addition, the therapeutic relationship between therapist and patient is collaborative, in the sense that the outline of each session (agenda setting) and the treatment as a whole are negotiated. Motivation to change habits and to alter behavior is crucial, and it is made clear to the patient that work is required for the treatment to have any effect.
All sessions follow a common structure, including check-in, agenda setting, review of homework and feedback, presentation of new material, and scheduling of homework for the next appointment. An outline of the protocol is given in Table 8–1. The treatment is presented in 6 to 10 sessions, meaning that it is possible to devote more than one session to each component. However, the present limit of the number of sessions given should be adhered to because there otherwise may be a risk of less focused and unproductive sessions.
| Session | Activities |
|---|---|
| Assessment | |
| 1–2 | Structured interview of tinnitus problems, related problems such as hearing impairment and noise sensitivity, and history; check of previous treatments and consultations for tinnitus and other conditions; assessment of available time needed to take part in the treatment; questionnaires given as homework assignments, including daily diary ratings for at least 1 week; rationale for the treatment; goal setting and decision regarding type of treatment (i.e., group, individual, or Internet) |
| Treatment | |
| 1 | Feedback on functional analysis, home registrations, and questionnaires; repetition of treatment rationale and rationale for applied relaxation; in-session training of step 1, Progressive relaxation (tense and release body parts); progressive relaxation twice daily as homework for the next week; plan practice and prepare for problems; assessment of treatment credibility to bring back to next session |
| 2 | Review of homework and feedback; tinnitus and environmental sounds; use of environmental “sound enrichment” strategies for facilitation of habituation to tinnitus (this may include tapes or CDs, but more importantly advice and analysis of fluctuations in tinnitus and the risk associated with trying to mask, i.e., cover the tinnitus. Later on, the effect of using sounds to cope with tinnitus is discussed, and the cognitive aspects of masking are covered, e.g., how masking of tinnitus and attention may interact); in-session training of step 2, Release-only relaxation without tension; instruction on how to use imagery techniques and in vivo presentation; release-only relaxation including imagery given as homework for the next week (2 times per day); registration of environmental sounds as homework |
| 3 | Review of homework and feedback; advice regarding hearing loss and remedy of this as far as possible. This includes not only referral for the fitting of hearing aid(s), but also behavioral advice in the form of “hearing tactics” (Andersson, 2000). These are not only for the individual but also directed to the people close to the patient. Sleep management advice given when needed (may result in extra session; see McKenna, 2000); positive imagery; in-session training of step 3: Cue-controlled relaxation (controlled breathing). Cue-controlled relaxation as homework (2–5 times daily) and other components given when indicated |
| 4 | Review of homework and feedback; cognitive aspects of tinnitus; discussion of thoughts and beliefs associated with tinnitus and presentation of a model for changing maladaptive thoughts and beliefs when present. Emotional reactions are also focused, especially fear and avoidance in relation to tinnitus. In-session training of step 4: Rapid relaxation in everyday situations (5–10 times per day). Rapid relaxation given as homework |
| 5 | Review of homework and feedback; management of hyperacusis, including gradual exposure to everyday sounds; attention-diversion techniques and more on imagery techniques; reinterpretation of tinnitus; attention-shifting exercises; exposure to tinnitus/quiet environments; further practice of rapid relaxation in more difficult and stressful situations. Rapid relaxation, exposure, and cognitive tasks given as homework |
| 6 | Review of homework and feedback; rapid relaxation repetition; exercise (graded, e.g., walking); relapse prevention advice regarding likely lapses in resistance toward the intrusive effects of tinnitus, as well as to prevent more permanent relapses; rapid relaxation, exercise given as homework; questionnaires and scheduling of follow-up appointment |
| 7 | Follow-up visit |
Structured Interview and Questionnaires
At least one otolaryngology consultation and audiological tests precede the first meeting with the patient. The latter includes audiogram, tinnitus masking level, and matching. The psychologist interviews the patient using a structured interview, including questions on tinnitus history, characteristics, psychological and physical consequences (e.g., sleep disturbance), exacerbating and relieving factors, related symptoms, and previous treatments (Andersson, 2001; Andersson et al, 1999). The aim of the interview is to establish a good therapeutic contact and to collect enough information to be able to decide if the patient is suitable or not for psychological treatment. This is typically done in the format of a functional analysis. In this context, functional analysis is a term used for collecting information about factors that influence the tinnitus annoyance, and investigating causal links between what the patient does and experiences and how tinnitus is perceived. This includes health, audiological, and psychosocial factors. Typically, 1½ hours is needed to interview the patient. In this first session a rationale is presented that incorporates the idiosyncrasies of the patient and also gives some preliminary goals of the treatment (McKenna, 1987). Following the interview, it is decided whether treatment should begin or whether an alternative is more suitable.
Once the decision has been made to start treatment, the patient is given a questionnaire as the first homework assignment for the next session. Questionnaires can be divided into tinnitus-specific or more global devices, including those aimed at assessing psychological well-being and cognitive functioning. In this context, it is important to be aware of the special needs and circumstances surrounding the tinnitus patient that may affect the ability to complete an assessment. The most obvious example is hearing impairment, but there are other less conspicuous problems, such as fatigue, lack of motivation, and litigation status, that may affect the result. The psychological dimensions of tinnitus complaints are usually measured with self-report instruments specifically developed for use with tinnitus patients (Noble, 2000; Tyler, 1993). Validated measures of depression and anxiety can be useful when one is planning and evaluating the treatment (e.g., Beck et al, 1961; Zigmond and Snaith, 1983).
Daily diaries can be used in clinical practice to collect data on the characteristics of tinnitus. Tinnitus often fluctuates, sometimes even within a day, and occasionally this aspect of tinnitus is not clear to the patient. Daily diaries need to be easily comprehended and unobtrusive while still providing usable data. One alternative is the Visual Analogue Scale (VAS), which is a straight line, the end anchors of which are labeled as the extreme boundaries of the sensation, feeling, or response being measured (Wewers and Lowe, 1990).
Tinnitus Education
Information about tinnitus and a proper examination of potential causes and moderating factors are crucial. This should be familiar to all clinicians dealing with tinnitus, but lately it has become even more relevant, given the abundance of information about tinnitus provided by mass media and the Internet. Hence patients sometimes do not need more information, but rather advice regarding what information they should trust. Unfortunately, given the lack of knowledge regarding tinnitus (e.g., regarding prognosis), it is often difficult to give the patient definite answers (and if there are no answers, none should be given). CBT for tinnitus includes presenting information to the patient in a gentle and pedagogic manner. Early in the treatment many patients need help to sort out the different problems they experience, which may require different solutions. For example, hearing impairment is not caused by tinnitus, and it needs separate attention.
Preferably, the patient should be able to find out things on his or her own, and the therapist should not present information as hypotheses to be tested together with the patient, rather than as facts. Although the clinician should be careful not to adopt too much of an expert role, which may lead to an endless question-and-answer feedback loop, it is crucial that the patient trust the clinician’s level of competence. As pointed out by Tyler et al (2001), it is important to nurture patient expectations and to instill hope, and the patient should get a sense of confidence that this is the right place to talk about tinnitus. However, at the same time, the patient should have realistic expectations, including that treatment is not likely to affect the loudness of tinnitus.
TREATMENT RATIONALE
A rationale, or explanation, of the aims of the treatment is given at the end of the first assessment session, but there is a need to continue to update and specify the rationale for each of the treatment components presented in Table 8–1. As mentioned previously, the therapeutic relationship is important, but so too is the structure of the sessions. The clinician needs to check previous knowledge because some patients may have extensive knowledge about tinnitus and, in some cases, psychology. Previous experience with psychotherapy is important to probe because may interfere with the treatment if unrecognized.
The rationale for the CBT treatment is put forward in an individualized manner, with sensitivity to each patient’s idiosyncrasies. First, feedback on the structured interview is given, then the obtained information is used to present a model, which is done with the patient’s input. This model can be represented as a cycle, with stress and other factors leading to increased awareness of tinnitus, which then causes more stress, and so on. In our presentation we have found it useful to distinguish between the actual tinnitus “sound” and the consequences of tinnitus. We explain how tinnitus can be conditioned to strong emotional reactions; however, we know from research that the interpretation of stimuli affects how they are processed. We explain this using metaphors (e.g., the reaction generated when hearing a sound outside the door at night). We then explain the role of selective attention and the attention-grabbing properties of tinnitus. For example, the ineffectiveness of masking the tinnitus is discussed in terms of selective attention and lack of habituation. Then the distinction between the tinnitus sound and the consequences of tinnitus is made. For example, tinnitus may sound like a loud, annoying horn; and this in turn may be associated with (i.e., lead to) increased tension, inactivity, and hopelessness. These are examples of consequences of tinnitus. Although the cause–effect relationship can be disputed, it is not appropriate at this point to dispute the patient’s belief about the effects of tinnitus. However, it is often the case that there are a host of other factors or problems that are causally related to the problems attributed to tinnitus (e.g., lowered mood because of problems at work). Instead of pointing that out, in our presentation we use a model of tinnitus symbolized as two circles (Fig. 8–1). The “tinnitus today” circle is larger and illustrates the consequences or effects of tinnitus. The second circle, “what we want to achieve,” is smaller and represents the treatment ingredients put forward as possible ways to shrink the tinnitus effects circle. The point is to illustrate that the “core” tinnitus may remain the same, whereas the consequences and the area in life devoted to tinnitus may decrease.
This is a very simple heuristic model, but it has the advantage that it can be constructed together with the patient and that both the worsening and the alleviating factors can be focused simultaneously. For example, in the “tinnitus today” circle, factors influencing tinnitus positively (represented by arrows pointing toward the circle) can be added, such as, “being on vacation.” Instead of focusing on things that are difficult to change, then, the influencing factors can be seen as easier to alter.
Yet another part of the presentation is to point out to the patient that CBT for tinnitus requires some relatively hard work, and that the person will need to work on registrations, exercises, and so on, for the whole treatment period, which includes daily homework assignments. Some patients at this stage may be reluctant and question whether it is realistic for them to add another activity (i.e., the treatment) to their already busy schedule. It is best to be frank when this question comes up. First, we say that it is unlikely that they would have come here if tinnitus was not a problem that needed to be addressed. Second, we point out that tinnitus at the beginning of treatment may become more noticeable, which indicates we are tapping the right processes that are influencing the distress associated with tinnitus. An example is working with stress problems, including monitoring the stress and testing problem-solving strategies. This at first may be perceived as increasing the stress, but it is very likely to decrease the stress in the long run. The parallel to exercise can be useful here. Effects will be noticeable in the long run. The treatment is not a quick fix. Tinnitus can be viewed as a signal to start doing other things in life, and some good things may come out of it all, although it is always crucial to acknowledge that tinnitus is something real and a hard challenge.
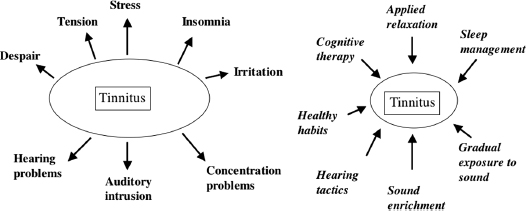
Figure 8–1 Heuristic model of the consequences of tinnitus (tinnitus today) and the way treatment may decrease the area in life devoted to tinnitus (what we want to achieve). The actual tinnitus sound is illustrated as being of similar proportions (same size of the boxes) before and after treatment.
A mountain metaphor can be used to describe how the treatment comes into the patient’s life: At first, treatment is like climbing up a mountain, with all the patient’s problems, seemingly insurmountable, ahead, but perhaps this is the only way to leave the mountain behind. Or perhaps the patient could try an alternative strategy and walk around the mountain. The point, though, is, whether it is scaled or walked around, the mountain is there.
It is important to return to the original treatment rationale as more specific information is given regarding each component. Be sure the patient understands the rationale. For example, already in the structured interview we ask: What did you think when the doctor suggested you should see a psychologist? The patient needs to see that thoughts, emotional state, and behaviors influence how tinnitus is tackled, and if there is a strong disease conviction, psychological treatment is not likely to work.
Applied Relaxation
TREATMENT RATIONALE
The rationale for applied relaxation includes, but is not restricted to, the following information (adapted from Öst, 1987). The text that is set in italics can be used as a training manual or patient handout to introduce the patient to the treatment/training protocol and to guide the patient in practicing at home.
Tinnitus is often associated with increased bodily tension, not the least because of how one reacts to tinnitus. There are also studies suggesting that muscular tension can be associated with increased loudness of tinnitus. Relaxation can make tinnitus more tolerable, decrease tension, and increase general well-being. Moreover, it can be a way to handle some of the consequences of tinnitus (e.g., irritation) and lead to increased control. Applied relaxation is a self-control technique in four steps, with each step building on previous skills obtained. The aim of the technique is to learn the skill of relaxation, which can be applied very rapidly and in practically any situation. This skill can be compared with any other learned skill (e.g., learning to swim, ride a bike, or drive a car), in that it takes time and practice to learn, but once you have mastered it, you can use it anywhere. You should not become restricted to the calm and nonstressful situation in this office or your own home.
The goal is to be able to relax in 20 to 30 seconds and to use this skill to counteract the physiological and mental reactions you may have in relation to tinnitus and other stressors in life. To achieve this goal, we will go through a step-by-step process, starting with tensing and relaxing different muscle groups. This will take about 15 minutes, and you will practice this twice a day. Next, we reduce the time by taking the tensing exercise away, just relaxing, which will take about 5 to 7 minutes, but we will add an exercise involving imagery techniques, which will take about 2 to 3 minutes. The next step teaches you to connect a self-instruction to the bodily and mental state of relaxation. We will then introduce rapid relaxation, which you will practice many times in nonstressful situations. In the last step, you will learn to apply the relaxation skill in more difficult situations related to your tinnitus.
The aim is not to reduce tinnitus per se, but to control its effects. However, you should not be surprised if you come to perceive your tinnitus as decreased. The goal of applied relaxation is to obtain a balanced state of mind. It is the average level of tension during the day that is important to decrease, not only those occasions when you feel especially tense. In fact, individuals who do not feel particularly tense also benefit from applied relaxation. In association with the relaxation training imagery, techniques will be introduced (e.g., imagining a beach) that are useful for coping with tinnitus. Numerous research studies have found that applied relaxation has positive effects on medical conditions (e.g., pain), but it’s also beneficial for healthy individuals who come to feel less stressed and more efficient in their daily life. Moreover, applied relaxation is a skill that most people can acquire with the right instructions and a lot of practice. It is a portable skill that can be used in almost any situation, not only directly linked to tinnitus, but also for problems like falling asleep.
It usually takes a while for the positive effects of relaxation to show, sometimes even weeks. In the beginning you may become more aware of your tinnitus and of tension in your body. This is a sign that we are dealing with something important. Applied relaxation does not make tinnitus worse.
Rarely, relaxation may feel strange and odd, and even cause anxiety If so, stop and try again later. Do not expect immediate effects. Leave time during the day for practicing relaxation. Do not practice when you are short of time or tired.
Finally, applied relaxation is not something you use to get rid of tinnitus, but rather something you apply to make you stronger to deal with tinnitus. The time you devote to applied relaxation is well spent.
INSTRUCTIONS FOR APPLIED RELAXATION
In the following, the instructions for applied relaxation will be presented. Preferably, the therapist should model some of the tensing-relaxing exercises, as modeling facilitates proper understanding. For example, we always point out that it is not good to tense the muscles too much. For some patients it can be necessary to start by using some background sound (e.g., a radio playing soft music). As we will return to later, it is always crucial not to mask the tinnitus, as this can interfere with our goal to habituate thepatient to the tinnitus.
Step 1. Progressive Relaxation The important thing here is to learn to feel the difference between tensed and relaxed muscles. To do this, we tense the muscle for 5 seconds, then relax it for 10 to 15 seconds and notice the difference. You also become aware of the location of different muscles. Many people regard it as easier to relax a muscle if they have tensed it first, as the contraction of the muscle automatically leads to resting. The point, again, is to become more aware of your body, and not to obtain a perfectly relaxed state.
The following guidelines are recommended:
• Practice twice daily, preferably the same time every day (e.g., at 10:00 A.M. and 6:00 P.M.).
• Practice alone and be sure that nobody interrupts you.
• Find a quiet place to do the relaxation exercises.
• Avoid being too stressed or tired when doing the relaxation exercises.
• Wear comfortable clothes.
• Sit comfortably, straight and symmetrical.
• Use a chair with neck support, but do not lean backward during the relaxation exercises.
• Place your feet on the floor without pressing them down (you may need to have something under your feet).
• Your head should not fall forward or backward. Hold it straight in relation to your shoulders.
• Place your hands in your lap. Do not clutch them.
Write down the time you start the exercises, and rate your level of tension on a scale of 0 to 100. Do the same thing once you have finished the exercises.
Start by sitting comfortably and close your eyes. Tense (5 seconds) and relax (10 seconds) in this order:
• Right hand (make a fist)
• Left hand
• Both hands
• Upper arm (press your elbows toward your body)
• Forehead (wrinkle your forehead)
• Eyebrows (raise and lower your eyebrows)
• Eyelids
• Jaws (gently open and close your mouth)
• Tongue (press your tongue up then down)
• Lips (press your lips together)
• Neck front (lower your chin toward your chest, but do not bend your head forward)
• Neck back (press your head against the neck support)
• Shoulders (raise your shoulders upward)
• Take a deep breath, then release the air slowly.
Do these exercises twice day. I will ask you to register in a daily diary each time you do these relaxation exercises. Each occasion will take about 10 to 15 minutes to complete. It is important that you can practice these exercises undisturbed by the telephone, family members, work, or anything else. If you feel that you do not have enough time, it is better to postpone the exercises than to do them in a hurry. A good idea is to have set times and places where you do the applied relaxation training (e.g., 9:00 A.M. at work in your office). In addition, it is preferable that you space the exercise sessions so that you have at least 1 to 2 hours between them. Keep in mind that it is better to practice regularly than to be perfect each time you practice. In fact, 14 moderate exercises during a week are better than 3 perfect ones.
Step 2. Short Progressive Relaxation The purpose of this step is to reduce the time it takes to become relaxed and to introduce some imagery techniques. In this step you will learn to relax without first tensing the muscles. This will reduce the time needed for doing the relaxation training (5–7 minutes), and you will become more relaxed, as the tensing exercises can interfere with the relaxation. Again, you will need to practice at least twice daily over the next week. The idea is to focus on the same muscles as in the first step and to relax as much as possible. You will also be asked to focus on your breathing. Again, the positive effect of applied relaxation may not be immediately noticeable, and you need to be persistent in your training. Remember that applied relaxation training is most time consuming during the early stages of the treatment. If you should forget the order of relaxing the muscles or how you should do the exercises exactly, do not stop, but continue the exercises. You could always repeat the order before the next session. If you should experience any adverse effects, remember that these are of a temporary nature. Actually, negative reactions can be better than no reactions at all, as it tells us that the relaxation is tapping the processes involved in your problems. Practice will solve this. Do not practice if you are tired, do not have enough time, or are feeling particularly stressed. Also, make sure that you are undisturbed. If you have a problem relaxing any particular muscle, do not give up. Instead, stay focused for a while. Try to visualize the muscle as soft and loose. Continue with the exercise after you have done this. If you still feel that the muscle is not relaxed, you can tense it briefly or move it a bit and then relax. It is common in the beginning of this step to have some problems relaxing muscles without tensing them first. One way to solve this is to shift between steps 1 and 2 for a period.
Although the recommended time for doing this exercise is 5 to 7 minutes, it is up to you to set the pace. If you do not feel sufficiently relaxed, repeat the exercises when you have the time. You can also choose to go over the rest of the muscles in the body.
Instructions The order of relaxing the muscles is slightly different from step 1. From now on it is the “top to bottom” principle; that is, you begin by relaxing your forehead, then continue by checking each part of the rest of your body down to your feet. To increase relaxation, it is important to breathe correctly. To ensure that you are breathing properly, you need to breathe deeply from your abdomen.
Write down the time you start the exercises, and rate your level of tension on a scale from 0 to 100. Do the same thing once you have finished the exercises.
In association with the relaxation training, imagery techniques are introduced (e.g., imagining a beach; see section on cognitive techniques).
First, make sure you breathe deeply from your abdomen. You can check for this by holding one hand on your chest and the other on your abdomen. Then place your hands in your lap, close your eyes, and follow these instructions.
You will relax now. Concentrate and relax all your muscles. Let your body rest. … Begin by checking that your forehead is relaxed … your eyebrows … your eyelids. … Continue with your temples … tongue … lips … and jaw …
Relax your neck and throat… shoulders … down the arms and out your hands … to your fingertips …
Let the relaxation spread to your stomach … your back … now the lower parts of your body … your legs … your feet… out to your toes. Feel relaxed all over your body.
Continue to relax in your whole body. Monitor your breathing… only your breathing.
Take a deep breath, hold it, and release. RELAX. Think “RELAX” each time you breathe, so that the word becomes a cue for deeper and deeper relaxation. Feel how easy it is to breathe and that you have become relaxed. End by taking a deep breath. Go back to breathing normally. Check that you are relaxed. If not, go back and try again.
If you find the word relax unsuitable as an instruction, you can switch to another word or a short sentence, for example, “Calm down.” However, it is a good idea to stick with the word or phrase you start practicing with now.
Step 3. Cue-Controlled Relaxation (Controlled Breathing) The purpose of cue-controlled relaxation is to link your cue word to a calm, smooth breathing pattern. Controlled breathing is an easy way to become relaxed, and the cue word relax serves as an instruction to you and your body. Given proper practice, the process of relaxing to the cue word will become automatic. The controlled breathing and your cue word will make you able to relax within 2 to 4 minutes, which is faster than that achieved in the earlier exercises. However, when starting these exercises, you may need some more time to become fully relaxed. When you have completed these exercises, I will ask you to use your positive image (see Instructions for Positive Imagery). It is good if you can practice 2 to 5 times daily for the next week.
Common Problems Most people are not used to breathing from their abdomen, and they have devoted little or no thought to their breathing. Usually we breathe more rapidly and from the chest, so it takes some concentration to adjust your breathing so that you are filling your lungs fully. To do these exercises, make sure your clothes are comfortable. It is a challenge to relax in such a short time. If you find it too hard, go back to step 2; that is, review each of your muscles, and when you feel sufficiently relaxed, you can begin doing step 3 exercises.
Write down the time you start the exercises, and rate your level of tension on a scale from 0 to 100. Do the same thing once you have finished these exercises, and comment on the use of the positive image.
Sit in a comfortable position. You can check your breathing by placing one hand on your chest and the other on your abdomen. You are free to use an alternative cue word instead of relax.
1. Close your eyes. Take a deep breath. Release the air slowly and think “RELAX.” Do not push your breath.
2. Breathe with calm, regular breaths. Do not overdo it. Think “RELAX” each time you breathe out. Breathe in at your own pace. Feel that your body is becoming more and more relaxed. Keep this up for 1or 2 minutes. (One way to do this exercise is to count when you breathe in: 1-relax, 2-relax, 3-relax, etc.)
3. Take a deep breath, release the air slowly, and think “RELAX,” then go back to breathing normally.
Check your body for signs of tension from the head downward, and feel that you are relaxed properly. If not, go back to step 2.
4. Use a positive image in which you are not disturbed by anything. Visualize the seashore, a garden—anything that gives you a sense of ease and peace. Investigate this image with all your senses: sights, odors, sounds, any sensations. Concentrate on this image for a few minutes.
Step 4. Rapid Relaxation—First Session This exercise has two purposes: to be able to relax in natural nonstressful situations and to further reduce the time it takes to get relaxed, with the goal of being able to relax in 30 to 60 seconds. The exercise can be described as a mini-break or micro-pause from your ongoing activities and thoughts. Let the first exercises take longer, then gradually reduce the time. You need to do this exercise 10 to 20 times each day for it to have a good effect. The reason you keep your eyes open is to learn to use relaxation in everyday settings when it is not possible to keep your eyes closed. Because you will need to do this exercise often and regularly, it can be helpful to plan in advance the situations and places when you can practice. Preferably, these situations will work as cues for you to do the rapid relaxation. Moreover, when you start practice you need to begin with easy situations in which you do not feel tense or nervous. To achieve this, you can think over how your day usually goes and from that plan the situations in which you can do the rapid relaxation. Examples can be in the car, when talking on the phone, when you look at your watch, when you turn on your computer, before eating and coffee breaks, and so on. Write down a list of all the situations and read it through to facilitate remembering the situations. Another method is to write notes to yourself and place them so that you will be reminded (e.g., on the refrigerator). Yet another way is to use small colored stickers and place them where you want to be reminded to do the rapid relaxation. Follow these instructions:
1. Focus your attention on your breathing. Fixate on one point in space and look at it for the whole exercise.
2. Take a deep breath from your abdomen. Release the air slowly and think “RELAX” (or your own cue word).
3. Relax in all of your muscles, throughout your body, from your forehead down to your toes. Feel the relaxation spread in your body.
4. Continue to breathe from your abdomen at your own pace, without exaggerating your breathing. Scan your body for tension.
5. Continue with what you did before the exercise and stop fixating on the point in space.
If you find this too difficult, try taking another deep breath, but avoid taking too many deep breaths in a row, as this may lead to overbreathing, or hyperventilating, which can result in some dizziness and shortness of breath. This is not dangerous, but you should avoid it. You also could try relaxing for a longer period. The relaxation training is more effective if you stay in a relaxed state long enough. Once you feel that you have mastered the technique, the time to do the exercises can be shortened. Pay extra attention to scanning your body for tension. Concentrate on any body part that feels tense and try to relax that part.
Step 5. Rapid Relaxation—Second Session The exercise for this week is identical to the rapid relaxation you did last week, but this week you will use rapid relaxation in stressful situations and when you are disturbed by your tinnitus. Examples can be when you concentrate on something, when you are attempting to sleep, in noisy environments, when you are problem solving, when you face obstacles, and when your tinnitus sounds loud. It is advisable to apply the relaxation techniques as soon as you feel any tension, as it is more difficult, even impossible, to relax if you are too stressed. Keep in mind that you use these relaxation techniques to feel well overall, and not to ward off tinnitus. Therefore, it is crucial that you apply rapid relaxation in different situations so that it is not linked in your mind to bad experiences. If that happens, rapid relaxation may be a reminder that you have problems, and this is not want we want to achieve.
Cognitive Techniques
There are two main cognitive components in the program. The first deals with attention-diversion techniques, use of “inner picture” imagery, and exercises directly aimed at reinterpreting tinnitus as something less painful (see Hallam, 1989; Henry and Wilson, 2001), then applying those skills in real-life settings. The latter involves exposure techniques inspired by the principles used in the treatment of phobias. These techniques are beginning to be applied with chronic pain patients (Vlaeyen et al, 2001), and our experience is that they are applicable for a proportion of tinnitus patients.
The second major cognitive component concerns cognitive restructuring of thoughts and beliefs associated with tinnitus. The patient is helped to identify the content of his or her thoughts and is taught ways to challenge or control those thoughts that are unhelpful or inaccurate. It is important to note that this is not equal to “positive thinking.” In the context of changing beliefs and thoughts, it is important to work toward acceptance of tinnitus and to foster the idea that tinnitus is not worth all the attention it gets. We present the idea that thoughts and emotions related to tinnitus sometimes are the main source of the problems. During later stages of the treatment it can be valuable to work for reinterpretation of tinnitus into something less threatening. Fear and beliefs that tinnitus will lead to something harmful in the long run are not uncommon and should be dealt with in the treatment. Problems with concentration are often a source of great distress for the tinnitus sufferer and are targeted in the treatment. Although not well developed for tinnitus, methods for improving concentration and memory training can be used. Strong emotional reactions, particularly involving fear and avoidance, are commonly associated with tinnitus. They can lead to a negative view of tinnitus and can occasionally develop into panic-like attacks when the patient seeks to escape from tinnitus. Apart from advice regarding sound enrichment, the program deals with adverse reactions to silence (when this is a problem).
The following is an example of the use of positive imagery. Occasionally, the therapist can skip aspects relating to sounds in the instruction (at least the first time), and ask patients afterward if they were aware of tinnitus during the exercise. Often, patients report that they forgot their tinnitus while focusing on the image.
INSTRUCTIONS FOR POSITIVE IMAGERY
There are many advantages to being able to use positive imagery: (1) it can help you maintain a relaxed state; (2) the positive image can become the mental equivalent of your bodily relaxation; (3) your mental abilities and focusing skills are maintained; (4) it can increase general well-being. The following suggestions are given.
1. Choose a mental image unrelated to your tinnitus. It can be something from nature or wildlife. One example is picturing yourself standing on the beach and looking out at the sea. You can choose something you have seen in real life, but it is better not to include other people in your image. Also, your image should not be associated with any problem solving, work, or other effort. It is good to involve several senses, includ ing vision, hearing, and smell.
2. Use your relaxation exercises from steps 1 through 4, then start focusing on your positive image.
3. Imagine that you are exploring that image. For example, you can look out over the sea, to the right, to the left, perhaps see a boat… look at the beach … smell the salty air and feel the sand under your feet … feel the wind blowing … hear the waves … notice other details.
4. Let go of your positive image and slowly open your eyes. Do not stay too long with your image so that tinnitus takes over. If that happens, focus again on your positive image. Stop if you lose your concentration. Start by doing small exercises, so as not to overdo it.
Hearing Tactics
Because many tinnitus patients also suffer from hearing loss, advice regarding hearing rehabilitation is given. Hearing tactics were defined by van der Lieth (1973) as “those methods used by someone suffering [with] a hearing impairment to solve the problems of his daily life—the practical, technical, and psychological problems caused by the handicap” (p. 209). Hearing tactics often deal with different ways of facilitating communication, such as optimizing signals and using conversational strategies. A cognitive-behavioral adaptation of hearing tactics has been developed by our research group (Andersson, 2000; Andersson et al, 1995b). In the tinnitus program a condensed version is used based on individual needs. Training in behavioral hearing tactics involves communication skills training, in which the participant is encouraged to focus on one person and concentrate on the communication with him or her. This includes proper positioning in relation to the other person, moderately expressive body language, and being active in the conversation. When hearing fails, repair strategies are practiced, which include ways of handling missing information and asking for confirmation if the participant has understood things correctly. This necessitates active listening and focusing on the meaning instead of the details of the message. Assertive responses are practiced, such as telling others about the hearing loss and anticipating their reactions. Also covered are waiting for your turn, reinforcing the behavior of the communication partner, and the advantages of talking on a topic about which you have knowledge. In our practice we distribute a leaflet that includes advice on communication with hearing-impaired people, which patients are to present to their closest relatives or friends as a homework assignment. We then discuss the supporting role of relatives and friends and the ways they can help. Homework includes distribution of the leaflet and of individualized applications of the skills taught earlier.
Sleep Management
Sleep hygiene, bedtime and worry-time restriction, relaxation, and cognitive restructuring can be helpful for patients with sleep problems (McKenna, 2000). These methods are tailored according to the special needs of the tinnitus patient.
Relapse Prevention
In brief, this includes a proper discussion of risk factors for developing more severe tinnitus and hearing loss, then devising a plan for what to do should the tinnitus become worse (Henry and Wilson, 2001). This can include returning to the relaxation training and to the sound-enrichment strategies.
As part of the secondary prevention part, the importance of regular exercise is covered. The word exercise is usually associated with hard work, sweat, and muscles. The exercise we often forget is the one we can get naturally, for example, by cycling or walking instead of taking the car or bus for short distances. Taking the stairs instead of the elevator is another example. Instead of a coffee break, a walk in the park could be beneficial. Several research studies show that exercise can alleviate and even prevent depression, insomnia, and stress (Gullette and Blumenthal, 1996), and some preliminary evidence suggests that exercise is good for tinnitus too. The effects of exercise are similar to the effects of relaxation; that is, physical and mental balance, but the approach is different. A combination of the two is likely to have beneficial effects.
During exercise or immediately after, tinnitus can become temporarily louder and more noticeable. However, this is often temporary, and the beneficial effects of exercise always outweigh the small fluctuation in loudness the patient may perceive. On the contrary, most people find that tinnitus disturbs them less when they exercise. The patient is instructed not to be too ambitious and to gradually extend the time he or she devotes to exercise. Almost all activity can be regarded as exercise.
Cautions for the Cognitive-Behavioral Approach
Psychopathology and Tinnitus
Although preexisting psychological characteristics most likely affect the way a person reacts to tinnitus (Stouffer and Tyler, 1992), there is little evidence that psychiatric disturbance directly causes tinnitus. However, signs of moderate depression are common in patients with tinnitus, but this does not usually call for a different treatment approach from that described earlier. When a patient fulfills the criteria for major depression according to the classification system provided by the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 1994), a clinician should consider referral to a psychiatrist. Even as CBT-oriented psychologists, we make sure that major depression is handled first because it is a serious condition that often impedes tinnitus rehabilitation if the depression is not handled properly. In addition, clinically depressed tinnitus patients should be informed about the treatment options and the studies showing improvement following the use of antidepressants (Sullivan et al, 1993). Because cognitive-behavioral therapy is also a helpful treatment for depression (Dobson, 1989), it can sometimes be advisable to combine treatments for depression and tinnitus (for a similar discussion involving the field of chronic pain treatment, see Williams, 1998). Studies investigating the effects of such a strategy have not been conducted.
When Applied Relaxation Should Not Be Used
The first example of when relaxation should not be used is when a patient is clinically depressed and shows clear signs of psychomotor retardation. It is evident that a patient who can hardly stand up because of fatigue and malaise should not be instructed to relax more. Instead, behavioral activation should be recommended. There are other precautions to consider when a patient is on medication or is suffering from a medical condition when the effects of relaxation should be specifically targeted for that condition. An example is asthma. It is not that relaxation is counterproductive in the case of the asthma patient; rather, it is that it cannot be presented in isolation. As already mentioned, applied relaxation can be used as an avoidant strategy instead of an approaching strategy, and that is why the reasons for doing relaxation always should be discussed and monitored.
Groups versus Individual Treatment
Although there are similarities, there are also differences between individual work and group treatment. Clearly, some individualization is sacrificed in group treatment, but on the other hand the group provides an interpersonal context in which patients can learn new ways of dealing with tinnitus, and they can also benefit directly from each other’s experiences. Group treatment is also cost effective, can help cut waiting lists, and can therefore be made available to patients more quickly. Positive experiences from cognitive-behavioral therapy in small group settings have been reported (Henry and Wilson, 2000; Kröner-Herwig et al, 1995) and a majority of published controlled trials on CBT for tinnitus have been in the form of group treatment (Andersson and Lyttkens, 1999). A distinguishing feature about the Uppsala studies (e.g., Scott et al, 1985), in which applied relaxation has been used, is that treatment has been conducted individually. Preliminary outcome data suggest that the results of the protocol can be extended to group treatment, which probably is the most common treatment format in clinical practice for tinnitus patients. Also, there were no clear differences in efficacy between individual and group treatments when the two formats were compared in a meta-analysis (Andersson and Lyttkens, 1999). To our knowledge, there has been no direct comparison between the two formats in the same research study.
Conclusion
The protocol described in this chapter has been evaluated in a series of studies conducted in Uppsala (for a review, see Andersson et al, 1995a). The effects of psychological treatment have been reviewed, most recently in a meta-analysis (Andersson and Lyttkens, 1999). Overall, the effects are well established, and although the strongest effects have been found immediately following treatment, there is evidence that positive treatment effects are maintained at follow-up. However, the effects are mostly seen with regard to tinnitus annoyance and to a lesser extent the perceived loudness of tinnitus. In a majority of studies on the effects of cognitive-behavioral therapy for tinnitus, psychologists have served as therapists, and it is now appropriate that the methods are adapted for use by a broader range of professionals such as hearing therapists and audiologists.
Applied relaxation, used in conjunction with other CBT techniques, represents a useful treatment for tinnitus. The method is easy to learn and has beneficial effects overall, not just on tinnitus distress.
Acknowledgments
Berit Scott, Per Lindberg, Lennart Melin, and Leif Lyttkens are gratefully acknowledged for their work in developing an earlier version of this program and for evaluating it in controlled studies.
References
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. Washington, DC: Author; 1994
Andersson G. A cognitive-affective theory for tinnitus: experiments and theoretical implications. In: Patuzzi R, ed. Proceedings of the Seventh International Tinnitus Seminar. Freemante, Australia: University of Western Australia; 2002:197–200
Andersson G. Hearing impairment. In: Radnitz C, eds. Cognitive-Behavioral Interventions for Persons with Disabilities. Northvale, NJ: Jason Aronson; 2000:183–204
Andersson G. The role of psychology in managing tinnitus: a cognitive behavioural approach. Semin Hear 2001;22:65–76
Andersson G, Lyttkens L. A meta-analytic review of psychological treatments for tinnitus. Br J Audiol 1999;33:201–210
Andersson G, Lyttkens L, Larsen HC. Distinguishing levels of tinnitus distress. Clin Otolaryngol 1999;24:404–410
Andersson G, McKenna L. Tinnitus masking and depression. Audiology 1998;37:174–182
Andersson G, Melin L, Hagnebo C, Scott B, Lindberg P. A review of psychological treatment approaches for patients suffering from tinnitus. Ann Behav Med 1995a;17:357–366
Andersson G, Melin L, Scott B, Lindberg P. An evaluation of a behavioural treatment approach to hearing impairment. Behav Res Ther 1995b;33:283–292
Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry 1961;4:561–571
Davies S, McKenna L, Hallam RS. Relaxation and cognitive therapy: a controlled trial in chronic tinnitus. Psychol Health 1995;10(2):129–143
Dobson KS. A meta-analysis of the efficacy of cognitive therapy for depression. J Consult Clin Psychol 1989;57:414–419
Gullette ECD, Blumenthal JA. Exercise therapy for the prevention and treatment of depression. J Pract Psychiatry Behav Health 1996;5:263–271
Hallam RS. Living with Tinnitus: Dealing with the Ringing in Your Ears. Wellingborough, UK: Thorsons; 1989
Hallam RS, Rachman S, Hinchcliffe R. Psychological aspects of tinnitus. In: Rachman S, eds. Contributions to Medical Psychology. Oxford: Pergamon; 1984:31–53
Hawton K, Salkovskis PM, Kirk J, Clark DM. Cognitive Behaviour Therapy for Psychiatric Problems. Oxford: Oxford University Press; 1989
Hayes SC, Bissett RT, Korn Z, et al. The impact of acceptance versus control rationales on pain tolerance. Psychol Rec 1999a;49:33–47
Hayes SC, Strosahl KD, Wilson KG. Acceptance and Commitment Therapy. New York: Guilford Press; 1999b
Heide FJ, Borkovec TD. Relaxation-induced anxiety: paradoxical anxiety enhancement due to relaxation training. J Consult Clin Psychol 1983;51:171–182
Henry J, Wilson P. Psychological management of tinnitus. In: Tyler RS, eds. Tinnitus Handbook. San Diego: Singular/Thomson Learning; 2000:263–279
Henry JL, Wilson PH. Psychological Management of Chronic Tinnitus: A Cognitive-Behavioral Approach. Boston: Allyn & Bacon; 2001
Jastreboff PJ. Tinnitus habituation therapy (THT) and tinnitus retraining therapy (TRT). In: Tyler RS, ed. Tinnitus Handbook. San Diego: Singular/Thomson Learning; 2000:357–376
Kröner-Herwig B, Hebing G, Van Rijn-Kalkmann U, Frenzel A, Schilkowsky G, Esser G. The management of chronic tinnitus: comparison of a cognitive-behavioural group training with yoga. J Psychosom Res 1995;39:153–165
Lindberg P, Lyttkens L, Melin L, Scott B. The use of a coping-technique in the treatment of tinnitus. Scand J Behav Ther 1984;13:117–121
Linton SJ. Applied relaxation as a method of coping with chronic pain: a therapist’s guide. Scand J Behav Ther 1982;11:161–174
McCracken LM. Learning to live with the pain: acceptance of pain predicts adjustment in persons with chronic pain. Pain 1998;74:21–27
McKenna L. Goal planning in audiological rehabilitation. Br J Audiol 1987;21:5–11
McKenna L. Tinnitus and insomnia. In: Tyler RS, ed. Tinnitus Handbook. San Diego: Singular/Thomson Learning; 2000:59–84
Møller AR. Similarities between chronic pain and tinnitus. Am J Otol 1997;18:577–585
Morin CM. Insomnia: Psychological Assessment and Management. New York: Guilford Press; 1993
Noble W. Self-reports about tinnitus and about cochlear implants. Ear Hear 2000;21:50S-59S
Öst L-G. Applied relaxation: description of a coping technique and review of controlled studies. Behav Res Ther 1987;25(5):379–409
Persons JB, Davidson J, Tompkins MA. Essential Components of Cognitive-Behavior Therapy for Depression. Washington, DC: American Psychological Association; 2001
Philips HC, Rachman S. The Psychological Management of Pain. New York: Springer; 1996
Schulman A. A final common pathway for tinnitus: the medial temporal lobe system. Int Tinnitus J 1995;1:115–126
Scott B, Lindberg P, Melin L, Lyttkens L. Psychological treatment of tinnitus: an experimental group study. Scand Audiol 1985;14:223–230
Stouffer JL, Tyler RS. Ratings of psychological changes pre-and post-tinnitus onset. In: Aran J-M, Dauman R, eds. Tinnitus 91: Proceedings of the Fourth International Tinnitus Seminar. Amsterdam/New York: Kugler Publications; 1992:449–452
Sullivan MD, Katon WJ, Russo JE, Dobie RA, Sakai C. A randomized trial of nortriptyline for severe chronic tinnitus. Arch Intern Med 1993;153:2251–2259
Tyler RS. Tinnitus disability and handicap questionnaires. Semin Hear 1993;14:377–383
Tyler R, Haskell G, Preece J, Bergan C. Nurturing patient expectations to enhance the treatment of tinnitus. Semin Hear 2001;22:15–21
Van der Lieth L. Hearing tactics II. Scand Audiol 1973;2:209–213
Vlaeyen J, De Jong J, Geilen M, Heuts PHTG, Van Breukelen G. Graded exposure in vivo in the treatment of pain-related fear: a replicated single-case experimental design in four patients with chronic low back fear. Behav Res Ther 2001;39:151–166
Wegner DM, Broome A, Blumberg SJ. Ironic effects of trying to relax under stress. Behav Res Ther 1997;35:11–21
Wewers ME, Lowe NK. A critical review of visual analogue scales in the measurement of clinical phenomena. Res Nurs Health 1990;13:227–236
Williams AC. de C. Depression in chronic pain: mistaken models, missed opportunities. Scand J Behav Ther 1998;27:61–80
Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand 1983;67:361–370
< div class='tao-gold-member'>



