Purpose
To evaluate clinicopathologically and immunohistochemically a spectrum of conjunctival squamous proliferations.
Design
Retrospective clinicopathologic study.
Methods
One large cell acanthoma, 7 epidermoid dysplasias, and 4 squamous papillomas were evaluated with microscopy and biomarkers Ki-67, p53, epithelial membrane antigen (EMA), Ber-EP4, AE1, AE3, and 8 individual cytokeratins. Normal associated conjunctiva served as a baseline for interpretation.
Results
The large cell acanthoma recurred 4 times but retained its benign histopathologic features. The cells were 2-3 times larger than the keratinocytes of the normal conjunctiva and did not display atypia. Immunohistochemistry revealed a low Ki-67 proliferation index (PI) in the large cell acanthoma compared with high indices in dysplasias and papillomas. p53 was negative in the nuclei of normal epithelium while positive in all neoplasms, most intensely in the dysplasias. Immunostaining showed similar staining patterns for cytokeratins in large cell acanthoma and normal conjunctiva, except for full-thickness CK14 positivity and CK7 negativity in the lesion. Dysplasias generally lost normal CK7 expression and frequently abnormally expressed CK17. The papillomas displayed a normal cytokeratin pattern but exhibited a higher than normal PI and weak p53 positivity.
Conclusions
Conjunctival large cell acanthoma is a morphologically distinctive clonal entity with clinical and immunohistochemical phenotypic characteristics denoting a dysplasia of minimal severity. Because of recurrences without invasion, it requires treatment. Dysplasias exhibited more deviant biomarker abnormalities including frequent aberrant full-thickness CK17 positivity and CK7 negativity. The absence of major cytokeratin derangements in the squamous papillomas may be of ancillary diagnostic value for lesions displaying borderline cytologic features.
Conjunctival intraepithelial neoplasia (CIN) or dysplasia (the term preferred in this article that also encompasses actinic lesions and carcinoma in situ) can lead to invasive carcinoma. CIN is recognized to have 2 major variants: a more common lesion composed of small, ovoid, eosinophilic, vaguely spindled, or atypical basosquamous cells, which may be admixed with larger epidermoid cells and may also occasionally be pigmented in patients with dark complexions ; and a less common and more aggressive mucoepidermoid variant, in which goblet cells or more subtle expressions of mucoid differentiation are present among the epidermoid elements. We generally prefer the term epidermoid (having eosinophilic cytoplasm) because squamous conveys a flattened rather than an oval shape although the two terms are commonly used interchangably. We have retained the term squamous for the papillomas. In this report, a rare example of conjunctival large cell acanthoma is contrasted histopathologically and immunohistochemically with more common forms of epidermoid (squamous) dysplasia and papillomas. Our overall objective is to evaluate the role of immunohistochemistry in refining diagnostic principles and in assessing the severity of atypicality for premalignant squamous conjunctival proliferations.
Methods
This retrospective clinicopathologic study was performed under the auspices of the Massachusetts Eye and Ear Infirmary Institutional Review Board (Protocol 12-132H) and conducted in compliance with the rules and regulations of the Health Insurance Portability and Accountability Act and in adherence to the Declaration of Helsinki and all federal and state laws.
After the diagnosis of a conjunctival large cell acanthoma was made, the diagnostic files of the David G. Cogan Laboratory of Ophthalmic Pathology at the Massachusetts Eye and Ear Infirmary were reviewed from July 1, 2008 to June 30, 2012 to identify lesions diagnosed as conjunctival squamous or epidermoid dysplasia, carcinoma in situ, conjunctival intraepithelial neoplasia, and papilloma. Among the cases retrieved was a pigmented dysplasia, which was nonetheless selected for inclusion. Blocks were evaluated for adequacy of remaining tissue to allow a battery of immunohistochemical tests. In addition to the large cell acanthoma, 7 routine dysplasias and 4 papillomas were deemed appropriate for this study. Normal conjunctiva present in 11 out of the 12 tissue specimens that were selected served as a baseline for comparison and analysis of the data assembled from the lesions.
Only the conjunctival aspects of the lesions were systematically evaluated immunohistochemically, inasmuch as these portions constituted the majority of the specimens and only a few had small associated strips of what appeared to be corneal epithelium. In most dysplastic lesions, the corneal component had been scraped off, supplemented with an alcohol scrub of the denuded Bowman membrane; the scrapings were not submitted for microscopic examination. Clinical and hospital records as well as clinical photographs were renewed to glean demographic data and other pertinent information on the clinical history and examination findings. In addition to hematoxylin-eosin staining and periodic acid–Schiff (PAS) staining with and without diastase, 4- to 5-μm paraffin-embedded histopathologic sections were prepared that employed the immunoperoxidase method using the chromogen diaminobenzidine with hematoxylin counterstaining. Table 1 lists the immunohistochemical probes that were available for this investigation in the Diagnostic Immunopathology Division of the Department of Pathology at the Massachusetts General Hospital.
| Probe | Characterization | Some Cell Specificities | Staining Pattern | Source | Dilution |
|---|---|---|---|---|---|
| Epithelial membrane antigen (EMA) | 75-kDa transmembrane glycoprotein (related to breast mucin) | Glandular epithelium and mesothelium (indicative of epithelial differentiation as a supplement to cytokeratins); squamous epithelial but not basaloid cells | Cytoplasmic and membranous | Mouse monoclonal (Leica Biosystems, Newcastle, UK) | Prediluted |
| Ber-EP4 | Antibody that recognizes 34-kDa and 30-kDa noncovalently linked glycopolypeptides | Secretory portion of eccrine glands; follicular germinative cells; basal but not squamous cell carcinoma of the skin; malignant mesothelioma | Membranous | Mouse monoclonal (Dako, Carpinteria, California, USA) | 1:50 |
| p53 | Transcription factor protein encoded by the p53 tumor suppressor gene, which induces apoptosis or cell cycle arrest in cells with damaged DNA | Mutant protein is overexpressed in many malignant conditions | Nuclear | Mouse monoclonal (Leica Biosystems, Newcastle, UK) | Prediluted |
| Ki-67 | Nuclear protein associated with cellular proliferation | Cells in active premitotic phases (G1, S, G2, and M) of the cell cycle undergoing DNA synthesis | Nuclear | Mouse monoclonal (Dako, Carpinteria, California, USA) | 1:200 |
| AE1 | Keratin proteins of low to intermediate molecular weights (56.5, 50, 48, and 40 kDa) in the acidic subfamily | Epithelial cells in early stages of cell development | Cytoplasmic | Mouse monoclonal (Invitrogen Corp, Camarillo, California, USA) | 1:1000 |
| AE3 | Keratin proteins of intermediate to high molecular weights (65-67, 64, 59, 58, 56, and 52 kDa) in the basic subfamily | Maturing epithelial cells including squamous cells | Cytoplasmic | Mouse monoclonal (Invitrogen Corp, Camarillo, California, USA) | 1:100 |
| Cytokeratin 7 (CK7) | Cytoplasmic intermediate filament a ; 54 kDa; basic | Epithelia of a large number of simple glands; eccrine and apocrine gland secretory coils but not their ducts; lacrimal gland acini and ducts; transitional (urothelial) epithelium; conjunctival epithelium; adenocarcinomas of lung and breast (including signet ring cell variants) and other metastases originating above the diaphragm; mucoepidermoid and epithelial-myoepithelial carcinomas; cutaneous adnexal (sweat gland) tumors; sigmoid and mesothelial sarcomas; sebaceous carcinoma; Paget disease | Cytoplasmic | Mouse monoclonal (Dako, Carpinteria, California, USA) | 1:3 |
| Cytokeratin 8 (CK8) | Intermediate filament; 52 kDa; basic | Secretory nonsquamous epithelia in skin, lung, breast, and gastrointestinal tract; synovial, epithelial, and mesothelial sarcomas; mucoepidermoid and adenoid cystic carcinoma | Cytoplasmic | Mouse monoclonal (Dako, Carpinteria, California, USA) | 1:200 |
| Cytokeratin 10 (CK10) | Intermediate filament; 56.5 kDa; acidic | Keratinized stratified epithelium; large epidermoid (prekeratinizing) cells; differentiated squamous cell carcinomas; uterine and cervical carcinoma | Cytoplasmic | Mouse monoclonal (Dako, Carpinteria, California, USA) | 1:200 |
| Cytokeratin 14 (CK14) | Intermediate filament; 50 kDa; acidic | Basal layer of squamous (conjunctival) and glandular epithelia; myoepithelial cells; mesothelium; syringoma; sebaceous tumors; mucosal carcinomas | Cytoplasmic | Mouse monoclonal (Leica Biosystems, Newcastle, UK) | 1:100 |
| Cytokeratin 17 (CK17) | Intermediate filament; 46 kDa; acidic | Basal layer of glandular epithelia; myoepithelial cells; conjunctival basal cells; Rathke pouch cyst; craniopharyngiomas; malignant myoepithelioma | Cytoplasmic | Mouse monoclonal (Leica Biosystems, Newcastle, UK) | Prediluted |
| Cytokeratin 18 (CK18) | Intermediate filament; 45 kDa; acidic | Glandular epithelia of gastrointestinal and respiratory tracts; conjunctival basal cells; thyroid, breast, renal carcinomas; rhabdoid tumors; adenocarcinoma of stomach and prostate | Cytoplasmic | Mouse monoclonal (Dako, Carpinteria, California, USA) | 1:100 |
| Cytokeratin 19 (CK19) | Intermediate filament; 40 kDa; acidic | Simple and complex epithelia; glandular-type epithelia; some squamous epithelial cells including full-thickness conjunctival epithelium; syringoma; mucosal squamous cell carcinoma; mucoepidermoid and adenoid cystic carcinoma | Cytoplasmic | Mouse monoclonal (Leica Biosystems, Newcastle, UK) | Prediluted |
| Cytokeratin 20 (CK 20) | Intermediate filament; 46 kDa; acidic | Simple epithelia of gastrointestinal tract; Merkel cells and their tumors; metastases originating below the diaphragm; transitional cell carcinoma; totally negative in conjunctiva (no Merkel cells present) | Cytoplasmic | Mouse monoclonal (Leica Biosystems, Newcastle, UK) | Prediluted |
a Other cytoplasmic intermediate filaments (average diameter between thin actin and thick myosin) are vimentin, desmin, neurofilament, and glial fibrillary acidic protein (GFAP).
Positivity in the immunoperoxidase preparations was determined for the cytokeratins as an all-or-none phenomenon when any intensity of immunohistochemical staining was observed in 50% or more of cells constituting the entire thickness of the epithelium. An assessment of graded intensities of positivity was not attempted except for p53 immunostaining. Specific cell counts for nuclear positivity were performed for p53 and Ki-67 only. Two counts in different areas of each lesion were averaged and reported as a percent of positive cells among those counted per high-power field (so-called proliferation index for Ki-67). In cases of moderate dysplasia, Ki-67 counts were confined to the bottom half of involved epithelium, whereas the p53 counts were made throughout the full thickness of the epithelium in both moderate and severe dysplasias. Cytokeratin (CK) staining patterns of normal and lesional conjunctival epithelium were also evaluated based on selective basilar, suprabasilar, and superficial expression of positivity. The results were collected for each diagnostic category of lesion and the categories were compared with each other and with the staining results manifested by the attached normal segments of conjunctiva in the surgical specimens.
Results
Clinical Findings
The clinical features of all 12 lesions in this series are summarized in Table 2 .
| Diagnosis | Age/Sex | Laterality, Location, a and Relevant History | Duration of Symptoms | Length of Follow-up | Recurrence |
|---|---|---|---|---|---|
| Large cell acanthoma | 51/F | Left eye, nasal limbus; sessile | 14 years | 14 years | 4 times |
| Dysplasia 1 | 79/M | Left eye, nasal limbus; sessile | “Many years” | 4 years | None |
| Dysplasia 2 | 45/M | Right eye, temporal limbus; sessile | 4 months | 3 years | None |
| Dysplasia 3 | 79/M | Right eye, inferotemporal limbus; gelatinous, opalescent b ; positive rose bengal staining | 3-4 months | 2 years | None |
| Dysplasia 4 | 69/M | Right eye, nasal limbus; gelatinous, sessile | 5-6 months | 6 months | None |
| Dysplasia 5 | 83/M | Right eye, temporal limbus, gelatinous, sessile | 3 months | 6 months | None |
| Dysplasia 6 | 39/F | Right eye, temporal limbus; pigmented, gelatinous, sessile; African-American; HIV positive | 8 years | 4 months | None |
| Dysplasia 7 | 91/M | Left eye, nasal limbus; vascular, gelatinous, sessile; pterygium excision; glaucoma | 2-3 years | 7 months | None |
| Papilloma 1 | 56/M | Right eye, inferotemporal epibulbar; yellow-colored, fleshy, sessile | 3-4 months | 4 months | None |
| Papilloma 2 | 70/F | Left eye, nasal inferior fornix and caruncle/plica; punctate vessels; sessile; focal pigmentation due to coincidental nevus | 3 months | 1 year and 3 months | None |
| Papilloma 3 | 62/M | Left eye, lower palpebral near eyelid margin; sessile | 3 months | 6 years | 2 times |
| Papilloma 4 | 39/M | Left eye, nasal bulbar and caruncle/plica; pedunculated | 4 months | 1 year and 7 months | Once (earlier treated with interferon for 3 months) |
a All lesions involved the corneal epithelium, which generally constituted 25% or less of the overall lesional size.
Large cell acanthoma
Because of its rarity and disputed nature, the clinical history of the patient with the large cell acanthoma is presented in more detail. A 51-year-old woman of Lithuanian and Irish descent developed over a period of 1 year gradual blurring of vision of the left eye associated with a foreign body sensation and occasional eye redness. Her past medical history was remarkable for pre–Waldenstrom macroglobulinemia and hypertension. She had undergone excision of atypical skin lesions in the past, but had never received a diagnosis of skin cancer. She grew up in New England and had extensive sun exposure. Best-corrected visual acuity was 20/20 OU. In 1998, slit-lamp examination showed an irregular, elevated, opalescent lesion located at the nasal limbus OS (unfortunately, a clinical photograph is not available). There was positive punctate corneal and interpalpebral conjunctival epithelial staining with fluorescein and rose bengal. The Schirmer test was abnormal (OD 3 mm, OS 1 mm). The patient was initially diagnosed with keratitis sicca, OS>OD. Debridement of the limbal lesion, which prevented pathologic evaluation of the lesional margins, was done and the patient was given punctal plugs and artificial tears. The lesion recurred after 6 months and was noted to involve more of the corneal surface, prompting another excision (1998). One year later, it recurred for the second time, and was re-excised and submitted for histopathologic evaluation (1999), which we were able to reevaluate and which showed abnormal cells at the surgical margins. During the interim, most of the ocular surface remained stable. The lesion recurred, however, for a third time after 6 years, leading to a third excisional biopsy (2005), which we were unable to review. Seven years after the last excision, the lesion recurred once again (2012). The latest lesion was located at the nasal limbus from 7-11 o’clock, appeared fimbriated, and extended 3 mm onto the cornea. Ocular surface surgery was recommended. Alcohol-assisted superficial keratectomy was performed on the affected corneal epithelium with surgical removal of adjacent involved conjunctiva. The surgical specimen displayed an uninvolved conjunctival margin but the corneal margin was positive. The ocular surface was then reconstructed with an amniotic membrane graft. The patient was treated postoperatively with topical steroids and antibiotics, with rapid resolution of the epithelial defect. There has been no recurrence after 8 months of follow-up.
Squamous dysplasias
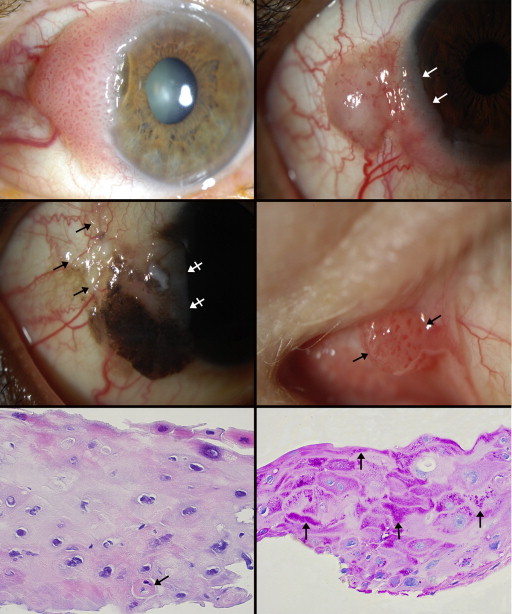
The clinical characteristics and epibulbar locations of the remaining 11 cases in this series are briefly described in Table 2 , which includes the 7 squamous dysplasias. There were 6 men and 1 woman with an average age of 69 years. All lesions arose at the limbus. The right eye was affected in 5 cases and the left in 2. The patients were symptomatic for an average of 24 months. All lesions were gelatinous or opalescent rather than leukoplakic, signifying the absence of keratinization. The lesions typically manifested a placoid or sessile papillary growth pattern with regularly distributed punctate vessels, indicating an underlying fibrovascular/papillary supporting architecture. The lesions bestrode the limbus extending onto the peripheral cornea as frosted epithelium, which constituted less than a quarter of their total size ( Figure 1 , Top left, Top right, and Middle left), with the largest portion situated in the juxtalimbal conjunctiva. One lesion in an African-American woman was partially pigmented ( Figure 1 , Middle left). The pigmentation extended within the epithelium onto the peripheral nonvascularized cornea. The average follow-up was 19 months, with no recurrences arising after a variety of therapies, including wide local excision of the conjunctival portion of the lesion, excision or scraping of the corneal extension, alcohol scrubbing of the denuded Bowman membrane, and adjuvant cryotherapy and/or topical antimetabolites to eradicate any remaining tumor cells.
Squamous papillomas
The 4 benign squamous papillomas were found in 3 men and 1 woman with an average age of 57 years. They were usually symptomatic for 3-4 months. Lesions arose in the epibulbar, plica/caruncular ( Figure 1 , Middle right), forniceal, and palpebral regions of the conjunctival sac, but not at the limbus. Three were sessile and 1 was pedunculated. The average follow-up was 28 months, during which 2 lesions recurred, requiring re-excision without adjuvant therapy.
Histopathologic and Immunohistochemical Findings
The immunohistochemical findings for all types of squamous lesions are summarized in Table 3 .
| EMA | BerEP4 | P53 | Ki-67 | AE1 | AE3 | CK7 | CK8 | CK10 | CK14 | CK17 | CK18 | CK19 | CK20 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Normal conjunctiva a (+/−) | 11/0 | 0/11 | 1.2% | 2.4% | 11/0 | 11/0 | 11/0 | 0/11 | 0/11 | 11 b /0 | 4 b /7 | 4 b /7 | 11/0 | 0/11 |
| Large cell acanthoma | + | − | 59.6% | 3.3% | + c | + | − | − | − | + | − | − | + | − |
| Dysplasia 1 | + | − | 87.8% | 37.2% | + | + | − | − | − d | + | − d | − | + | − |
| Dysplasia 2 | + | − | 91.9% | 42.8% | + | + | + | − | − d | + | + | − | + | − |
| Dysplasia 3 | + | − | 77.1% | 44.7% | + | + | − | − | − | + | + | − | + | − |
| Dysplasia 4 | + | − | − e | 32.6% | + | + | − | − | − | + | + | − | − | − |
| Dysplasia 5 | + | − | 83.9% | 39.6% | + | + | − | − d | − d | + | − d | − | + | − |
| Dysplasia 6 | + | − | 70.2% | 45.8% | + | + | + | − | − d | + | + | + | + | − |
| Dysplasia 7 | + | − | 84.9% | 24.6% | + | + | − | − d | − d | + | − d | − | + | − |
| Papilloma 1 | + | − | 11.2% | 17.5% | + | + | + | − | − | − b | − | − | + | − |
| Papilloma 2 | + | − | 21.5% | 12.9% | + | + | + | − | − | − b | − b | − | + | − |
| Papilloma 3 | + | − | 7.5% | 28.4% | + | + | + | − | − | − b | − | − | + | − |
| Papilloma 4 | + | − | 8.4% | 27.5% | + | + | + | − | − | − b | − | − | + | − |
a Number of specimens with normal control conjunctiva = 11.
b Basilar cell positivity only.
c Positivity for the various cytokeratins without an explanatory notation indicates staining of 50%-100% of cells throughout the entire epithelium; negativity indicates staining of fewer than 50% of cells.
d Focal positivity in suprabasilar cells and often in large atypical epidermoid cells.
e Negative staining was either an authentic finding or an artifact attributable to poor antigen preservation.
Large cell acanthoma
The last excision of the recurrent large cell acanthoma measured 0.7 × 0.5 × 0.1 cm. The lesion grew as a diffuse placoid thickening of the epithelium without an underlying papillary structure. It was composed of large, polygonal, eosinophilic cells 2-3 times the size of normal conjunctival keratinocytes with commensurately large nuclei containing small nuceloli. Many intercellular attachments (desmosomes) were seen during high-power microscopy. These features were detected in the first biopsy (1999) that could be reviewed ( Figure 1 , Bottom left and Bottom right) and persisted up to the final excision ( Figure 2 , Top left, Top right, and Middle left). Some variability in the size of the nuclei was focally detected ( Figure 2 , Top right) without any mitotic activity among the basilar and suprabasilar cells. The large tumor cells formed an abrupt interface with the adjacent normal conjunctival epithelium ( Figure 2 , Middle right) but were present at the corneal edge. The PAS stain highlighted prominent cytoplasmic positivity in the first available and last specimens ( Figure 1 , Bottom right, and Figure 2 , Bottom left), which could be abolished by means of pretreatment with diastase ( Figure 2 , Bottom right). This established that the stainable material was glycogen. Subepithelial chronic inflammation was not noted. p53 and Ki-67 nuclear staining ( Figure 3 , Top left and Top right) were the lowest cell counts of all the neoplasms in this series. Most notable were CK7 negativity ( Figure 3 , Middle left), in contrast to its consistent positivity in normal conjunctival epithelium; CK18 negativity, which is sometimes positive among the normal conjunctival basilar cells’ epithelium and rarely in suprabasilar cells ( Figure 3 , Middle right); and full-thickness epithelial positivity for CK14, which is present only in the basilar cells of the normal epithelium.
Squamous dysplasias
For the 7 conventional dysplasias, the average size of the excised specimens was 1.4 × 0.6 × 0.1 cm (range, 2.8 × 0.6 × 0.1 cm – 0.5 × 0.3 × 0.1 cm). All grew in a placoid or low papillary sessile pattern. Two were interpreted as moderately severe dysplasias with approximately 50% of the epithelial thickness replaced by atypical cells, whereas the other 5 lesions were severe dysplasias or carcinomas in situ with near to complete epithelial replacement. The moderate dysplasias with both basilar and suprabasilar mitoses were composed of small epidermoid/squamoid cells with eosinophilic cytoplasm and small round or oval nuclei with small nucleoli ( Figure 3 , Bottom left). These cells occupied the bottom half of the epithelium above the basement membrane, while the upper or outer 50% of the epithelium displayed more elongated eosinophilic cells with narrower nuclei oriented parallel to the surface. In the severe dysplasias and carcinomas in situ (from a practical point of view, this distinction is more notional than applicable), virtually the entire thickness of the epithelium was replaced by varying grades of atypical cells containing multiform hyperchromatic nuclei ( Figure 3 , Bottom right, and Figure 4 , Top left). In 3 lesions, there were large, bizarre, pleomorphic, and sometimes multinucleated epidermoid cells forming small clusters or eosinophilic tracts within a sea of smaller basaloid cells ( Figure 4 , Top left; Figure 4 , Top right and Bottom left inset). No lesion was exclusively composed of basaloid cells with inconspicuous cytoplasm. In the pigmented dysplasia, dendritic melanocytes were interspersed among the basaloid cells and transferred negligible pigment granules to them ( Figure 4 , Top right, Bottom right inset), as highlighted by MART-1 immunostaining. There was an abrupt demarcation of the dysplastic cells from the adjacent normal epithelial cells ( Figure 4 , Middle left). The PAS stain with and without diastase disclosed prominent cytoplasmic accumulations of glycogen in 5 cases, present either in the small squamoid cells or in the large epidermoid cells; there was a complete absence of goblet cells within the lesions ( Figure 4 , Middle right and inset). Chronic inflammation in the form of a variably prominent but typically modest infiltrative band in the superficial substantia propria was present in all lesions. The most salient immunohistochemical results ( Table 3 ) were p53 and Ki-67 nuclear staining in the lower half of the epithelium of the moderately severe lesions, whereas there was full-thickness staining with these biomarkers in the severe lesions ( Figure 4 , Bottom left and Bottom right; Figure 5 , Top left and Top right). The average percent of positive nuclei was 82.6% for p53 and 38.2% for Ki-67. Curiously, the larger epidermoid cells tended not to stain with Ki-67 ( Figure 5 , Middle left) but did for p53. Some horizontally flattened superficial cells were both p53 and Ki-67 positive. The surrounding normal conjunctival epithelium had close to zero p53 counts and low Ki-67 expression ( Table 3 ). With respect to immunostaining for the various cytokeratins, the dysplasias were overwhelmingly CK7 negative, in contrast to normal conjunctiva ( Figure 5 , Middle right). In a few instances, CK7 positivity was discovered among the basilar cells, at the surface of the lesions, or in their midst, generally within the large epidermoid cells ( Figure 5 , Bottom left). The dysplasias were more likely to express CK17 ( Figure 5 , Bottom right) than the other lesions and were full-thickness CK14 positive, whereas this marker is present only in the basilar cells of normal conjunctiva.



