Clinical Examination
Ear
John Hill
Examination of the ear
In infective cases it is worth checking behind the ear to see if there is any swelling of the post-auricular lymph nodes or a subperiosteal abscess (1.1; see acute mastoiditis, 4.32,4.33 and 4.34). The best view of the drum is obtained by using an auriscope which is inserted into the lateral third of the ear canal only (1.2). Avoid putting the tip of the speculum into the medial two-thirds of the canal as it is much more sensitive. The view is improved by elevating the pinna upwards and backwards in an adult or straight backwards in a child. Holding the auriscope horizontally, rather than vertically, means the patient’s shoulder is less likely to get in the way. Holding the little finger out extended towards the cheek is a useful technique in children because if the child turns towards the examiner unexpectedly it reduces the chance of twisting the speculum of the auriscope in the ear canal, which can be painful. If the drum is difficult to see it is often worth looking more superiorly by tilting the patient’s head away from the examiner (1.3).
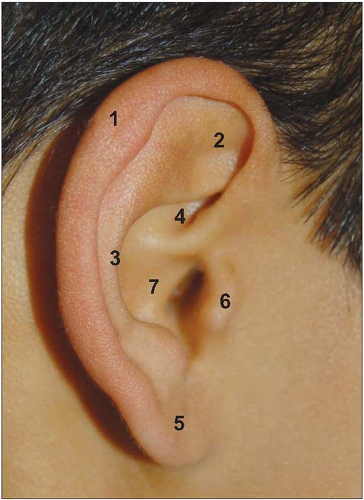 1.1 Normal pinna showing the main anatomical features: helical fold (1), triangular fossa (2), antihelical fold (3), scaphoid fossa (4), lobule (5), tragus (6), and conchal bowl (7). |
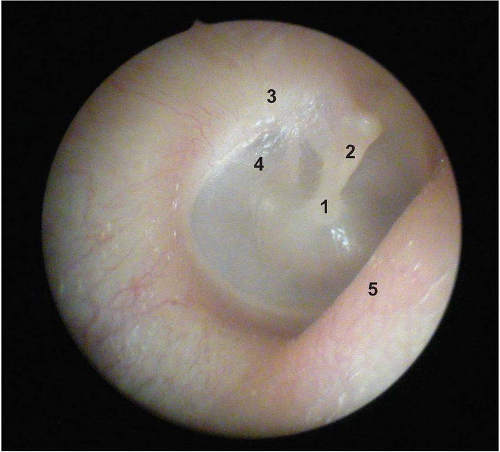 1.2 Normal right tympanic membrane showing the main features: umbo (1), handle of the malleus (2), pars flaccida (3), long process of the incus visible through the pars tensa (4), and bulge of the anterior wall of the ear canal (5). |
 1.3 Position of auriscope during otoscopy. |
 1.4 Rinne test 1. ‘Can you hear this?’ |
 1.5 Rinne test 2. ‘Is this louder or quieter?’ |
 1.6 Weber test. ‘Does this sound as if the sound is in the middle or coming from the side? Which side?’ |
Tuning fork tests
The traditional Rinne and Weber tuning fork tests using a 512 Hz tuning fork are still of value in establishing whether hearing loss is conductive or sensorineural in nature. Hearing loss due to disease in the external ear canal or middle ear will give a conductive loss. Diseases affecting the inner ear cause a sensorineural loss.
Rinne test
The tuning fork is placed on the mastoid process behind the ear and counter pressure applied to the side of the head to make sure of good contact. The patient is asked: (1) Can you hear the tuning fork? The tuning fork is then held alongside the ear approximately 2-3 cm from the meatus and the patient is asked: (2) Is this louder or quieter (1.4, 1.5)? A positive Rinne response means that the tuning fork was heard louder beside the ear rather than placed on the mastoid behind. A negative Rinne response is the converse.
Weber test
The tuning fork is placed in the centre of the patient’s forehead. The patient is asked: (1) Can you hear the tuning fork? (2) Is it louder in one ear or is it equally heard in both ears (1.6)?
Interpretation
A Rinne positive response is present if the hearing is either normal or the hearing loss is sensorineural in nature. If the Rinne test is negative, hearing loss will be due to a conductive loss. If a conductive hearing loss is present, a Weber test should be loudest in the affected ear. If sensorineural hearing loss is present a Weber test should be heard loudest in the unaffected ear.
Nose
Wolfgang Issing
Examination of the nose
Traditional anterior rhinoscopy using Thudicum’s speculum and a headlight or head mirror is helpful in detecting gross anatomical variations such as septal deviation, dislocation of the collumella (1.7) and hypertrophic inferior turbinates. With the help of a rigid (1.8) or flexible endoscope, the whole of the nasal cavity and the postnasal space can be examined. The middle meatus, into which most of the sinuses drain, can be thoroughly examined (1.9) and bony crests, spurs (1.10) and other abnormalities farther back in the nasal cavity can be identified. Rigid endoscopes give the clearest view but flexible endoscopes help if the nasal anatomy does not allow passage of the rigid endoscope. Decongestion of the nose, using sprays containing pseudo-ephedrine or pseudoephedrine plus lignocaine may be necessary to achieve optimum results and improve tolerance. The examination should be done to document findings systematically in the inferior and the middle meatus and the spheno-ethmoidal recess. Several anatomic variations exist in the nasal cavity that may contribute to an infection (1.11, 1.12). Possible findings include the presence of mucus or mucopus, polyps, and other mass lesions. Except for the posterior ethmoid and the sphenoid sinuses, all the sinuses drain into the middle meatus. Thus, the majority of sinus infections present with signs in the middle meatus.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


