Purpose
To compare the outcomes of cataract surgery performed with 3 incision size–dependent phacoemulsification groups (1.8, 2.2, and 3.0 mm).
Design
Prospective randomized comparative study.
Methods
One hundred twenty eyes of 120 patients with age-related cataract (grades 2 to 4) were categorized according to the Lens Opacities Classification System III. Eligible subjects were randomly assigned to 3 surgical groups using coaxial phacoemulsification through 3 clear corneal incision sizes (1.8, 2.2, and 3.0 mm). Different intraoperative and postoperative outcome measures were obtained, with corneal incision size and surgically induced astigmatism as the main clinical outcomes.
Results
There were no statistically significant differences in most of the intraoperative and postoperative outcome measures among the 3 groups. However, the mean cord length of the clear corneal incision was increased in each group after surgery. The mean maximal clear corneal incision thickness in the 1.8-mm group was significantly greater than for the other groups at 1 month. The mean surgically induced astigmatism in the 1.8- and 2.2-mm groups was significantly less than that in the 3.0-mm group after 1 month, without significant difference between the 1.8- and 2.2-mm groups.
Conclusions
With appropriate equipment, smaller incisions may result in less astigmatism, but the particular system used will influence incision stress and wound integrity, and may thus limit the reduction in incision size and astigmatism that is achievable.
It is generally the case that smaller clear corneal cataract surgical incisions are associated with more rapid wound healing, more stable corneal biomechanical properties, and less surgically induced astigmatism. With the development of phacoemulsification and foldable intraocular lenses (IOLs) during recent decades, the size of clear corneal incisions has been reduced from 3.2 mm (coaxial small incision) to 1.4 mm (bimanual microincision). Microincision cataract surgery, including bimanual and microcoaxial phacoemulsification, has attracted much interest recently, because of its safety and simplicity. However, the superiority of coaxial microincision cataract surgery as compared to conventional coaxial cataract surgery is still not certain, because microincision phacoemulsification may result in longer ultrasound time, the use of more ultrasonic power, and consequently higher endothelial cell loss.
In our previous studies of the OZil torsional phacoemulsification system (Infiniti; Alcon, Fort Worth, Texas, USA), we reported that the clinical outcomes of cataract surgery are influenced by many factors, including the blade used to create the incision, the phacoemulsification apparatus, and the IOL used and mode of insertion, which together constitute a surgical system, the outcomes of which are restricted by the best performance of each component. Today, microcoaxial phacoemulsification is in wide use for cataract surgery, but the lower limits of incision size should be understood in the context of the various components of the surgical system.
In this study, we compared the associated morbidity and surgical efficiency of 3 different incision size–dependent phacoemulsification systems, 1.8, 2.2, and 3.0 mm, and evaluated the relationship between incision size and surgically induced astigmatism.
Subjects and Methods
This prospective randomized study included 120 patients (120 eyes) with age-related cataract enrolled between July 5, 2010 and January 20, 2011 at the Zhongshan Ophthalmic Center, Guangzhou, China.
Inclusion Criteria
Inclusion criteria for enrollment included age between 55 and 85 years, the presence of nuclear or corticonuclear cataract of grades 2.0 to 4.0 (Lens Opacities Classification System III), a transparent central cornea, pupil dilation ≥7 mm at the time of preoperative examination, and a preoperative central endothelial cell count of ≥1500 cells per square millimeter. Potential subjects with previous intraocular surgery, glaucoma, pseudoexfoliation, uveitis, high myopia, and diabetes mellitus were excluded from participation in the study.
Phacoemulsification Systems
1.8-mm-incision-size phacoemulsification system
In this system, a self-sealing temporal clear corneal incision was made with a 1.8-mm calibrated knife (Bausch & Lomb, Rochester, New York, USA), phacoemulsification was performed with the Stellaris phacoemulsification machine (Bausch & Lomb), and an Akreos MI 60 IOL (Bausch & Lomb) was implanted in the capsular bag with the Viscojet 1.8 injector system (Bausch & Lomb), with care being taken to avoid unnecessary enlargement of the incision.
2.2-mm-incision-size phacoemulsification system
In this system, a temporal clear corneal incision was created with a 2.2-mm calibrated knife (Alcon Laboratories). Phacoemulsification was performed with the INTREPID System (Alcon Laboratories) and the OZil torsional handpiece (Mini-Flare ABS & Ultra Sleeve) set to continuous mode without axial ultrasound. An SN60WF IOL (Alcon Laboratories) was implanted with the Monarch III and Cartridge D injector system.
3.0-mm-incision-size phacoemulsification system
In this system, a temporal clear corneal incision was created with a 3.0-mm calibrated knife (Alcon Laboratories). Phacoemulsification was performed with the Infiniti Vision System (Alcon Laboratories) and the OZil torsional handpiece (Micro Tip ABS & Micro Sleeve) set to continuous mode without axial ultrasound. An SA60AT IOL (Alcon Laboratories) was implanted in the capsular bag with the Monarch II and Cartridge C injector system.
Randomization
Patients meeting the inclusion criteria were prospectively randomized to the 3 incision size–dependent phacoemulsification groups: incision size 1.8 mm (Group I), 2.2 mm (Group II), and 3.0 mm (Group III). A number between 1 and 120, generated by a random number generator, was assigned to each subject. The number was divided by 3. If the remainder was 1, the patient was assigned to Group I; if the remainder was 2, the patient was assigned to Group II; and if the number was divisible by 3, the patient was assigned to Group III.
Intraoperative and Postoperative Procedures
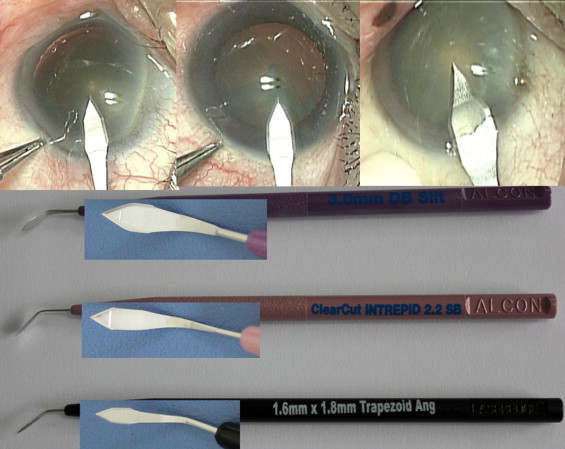
All surgeries were performed by the same experienced surgeon (Y.L.). Topical anesthesia consisting of a single drop of proparacaine 0.5% (Alcaine; Alcon Laboratories) was administered 3 times at intervals of 5 minutes prior to surgery. Then 1 of the 3 incision size–dependent phacoemulsification systems was used to carry out surgery depending on the patient’s group assignment, according to the following protocol. After a temporal clear corneal incision was made ( Figure 1 ) , sodium hyaluronate was used to reform and stabilize the anterior chamber and to protect the corneal endothelium. A 5.5- to 6.0-mm central continuous curvilinear capsulorrhexis was created with a bent 26-gauge disposable needle. Hydrodissection and hydrodelineation were carried out using balanced salt solution (BSS). A standard quick chop was performed to remove the lens nucleus, and residual cortical material was removed by irrigation and aspiration. No sutures were used to close the clear corneal incision. Postoperative topical therapy included 0.3% tobramycin and 0.1% dexamethasone eye drops (Tobradex; Alcon Laboratories) 4 times per day and 0.3% tobramycin and 0.1% dexamethasone eye ointment (Tobradex; Alcon Laboratories) every night for 1 month. All patients were followed up at 1 day, 1 week, 1 month, and 3 months after surgery.
Measurement of Outcomes
Cumulative dissipated energy and surgically induced astigmatism were the 2 main efficiency outcomes, and central cornea endothelial cell loss was the principal morbidity outcome.
Intraoperative outcome measures, including ultrasound time, surgical time, cumulative dissipated energy, total BSS volume, and surgical complications, were recorded at the end of each surgery. In addition, the corneal incision size was also measured with calipers (microincision gauge) by the same surgeon (Y.L.) before and after phacoemulsification and irrigation/aspiration (I/A), as well as after IOL implantation.
The best-corrected visual acuity (BCVA) was measured, using an ETDRS chart and autorefraction as refined by an ophthalmologist, preoperatively and at postoperative 1 day, 1 week, 1 month, and 3 months. The architectural profile of the wound, including maximal incision thickness, presence or absence of local Descemet membrane detachment, incision gaping, and misalignment, was documented by anterior segment optical coherence tomography (AS-OCT; Zeiss Meditec, Dublin, California, USA). Central corneal endothelial cell density was recorded preoperatively and at each postoperative visit by noncontact specular microscopy (SP2000P; Topcon, Tokyo, Japan). Central cornea endothelial cell loss was calculated on the basis of preoperative and postoperative endothelial cell density. Corneal astigmatism was measured using an eye scanner (Pentacam; Oculus, Wetzlar, Germany), and the surgically induced astigmatism was calculated at each postoperative visit using the following equation :
where K 2 represents the vector of surgically induced astigmatism, K 1 and K 3 stand for preoperative and postoperative corneal astigmatism respectively, and θ 1 and θ 3 indicate the preoperative and postoperative axes of corneal astigmatism.
All patients were examined by the same technician (Y.Y.). Both the technician and the surgeon were masked during postoperative examinations to the patients’ group assignment.
Statistical Methods
The SPSS software package (version 17.0; SPSS Inc, Chicago, Illinois, USA) was used for statistical analysis. Mean ultrasound time, surgical time, cumulative dissipated energy, total BSS volume, and surgically induced astigmatism were compared using multifactor analysis of variance. Univariate logistic regression was used to compare the clear corneal incision profile parameters, and Pearson χ 2 test was used to compare sex, nucleus grade, and preoperative and postoperative BCVA. All statistical tests were 2-tailed with α = 0.05. A P value of <.05 was considered statistically significant.
Results
One hundred twenty patients (120 eyes) meeting the inclusion criteria were enrolled and randomly divided into 3 groups of 40 subjects each. All patients completed all follow-up visits. The distribution of age, sex, surgical eye, and nuclear cataract grade was comparable among the 3 groups at baseline ( Table 1 ).
| Demographics | Group I | Group II | Group III | P Value |
|---|---|---|---|---|
| Initial corneal incision size (mm) | 1.8 | 2.2 | 3.0 | – |
| Patients/eyes (n) | 40/40 | 40/40 | 40/40 | – |
| Mean age (y) ± SD | 73.95 ± 6.05 | 71.37 ± 7.19 | 72.48 ± 6.15 | .221 |
| Male/female (n) | 21/19 | 18/22 | 19/21 | – |
| Right/left eye (n) | 19/21 | 22/18 | 21/19 | – |
| Nuclear density a | ||||
| Grade 2 (n/%) | 5/12.5 | 4/10 | 3/7.5 | – |
| Grade 3 (n/%) | 29/72.5 | 29/72.5 | 31/77.5 | – |
| Grade 4 (n/%) | 6/15 | 7/17.5 | 6/15 | – |
| Mean nuclear density | 2.98 ± 0.56 | 3.11 ± 0.59 | 3.02 ± 0.39 | .549 |
a Graded by the Lens Opacities Classification System (LOCS) III.
All 120 cataract surgeries were successfully completed. No intraoperative complications (posterior capsular tear, vitreous loss, retained lens fragments, or wound burns) occurred.
Table 2 indicates the ultrasound time, surgical time, cumulative dissipated energy, and the total BSS volume for each group. There were no statistically significant differences in the main intraoperative outcome measure of surgical efficiency (cumulative dissipated energy) or other surgical parameters among the 3 groups.
| Parameters a | Group I (1.8-mm Incision) | Group II (2.2-mm Incision) | Group III (3.0-mm Incision) | P Value b |
|---|---|---|---|---|
| UST(sec) | 41.17 ± 11.43 | 45.46 ± 22.39 | 48.47 ± 20.11 | .215 |
| ST (min) | 6.32 ± 0.47 | 6.45 ± 0.61 | 6.53 ± 0.50 | .228 |
| CDE (%) | 9.10 ± 2.88 | 10.93 ± 7.61 | 11.54 ± 5.90 | .152 |
| V BSS (mL) | 32.60 ± 11.62 | 39.05 ± 13.86 | 36.18 ± 9.07 | .051 |
| Complications(n) | 0 | 0 | 0 | — |
Table 3 shows the values for 3 intraoperative measurements of corneal incision size during surgery for each group. After phacoemulsification and I/A, the proportional enlargement of incision size in Group I was significantly greater compared to Groups II and III (5.69% vs 1.14% and 0.42% respectively, F = 81.524, P = .001). However, there was no statistically significant difference between Groups II and III ( P = .11). After IOL implantation, increase in clear corneal incision cord width was greater in Group I as compared to Groups II and III (5.39% vs 0.45% and 0%, F = 88.57, P = .001). There was no statistically significant difference between Groups II and III ( P = .32). Overall, the clear corneal incision size showed a significantly greater proportional increase in Group I than in the other 2 groups (11.41% vs 1.59% and 0.42%, F = 165.65, P = .001). No statistically significant difference was found between Groups II and III ( P = .079).
| Group I | Group II | Group III | P Value a | |
|---|---|---|---|---|
| Mean primary incision size (mm) | 1.80 | 2.20 | 3.00 | — |
| Mean size after phacoemulsification + I/A (mm) | 1.90 ± 0.06 | 2.23 ± 0.04 | 3.01 ± 0.03 | — |
| Incision enlargement (mm) | 0.10 ± 0.05 | 0.03 ± 0.04 | 0.01 ± 0.03 | .001 b |
| Change (%) | 5.69 | 1.14 | 0.42 | .001 b |
| Mean incision size after IOL implantation (mm) | 2.00 ± 0.09 | 2.24 ± 0.048 | 3.01 ± 0.03 | — |
| Incision enlargement (mm) | 0.10 ± 0.06 | 0.01 ± 0.02 | 0 | .001 b |
| Change (%) | 5.39 | 0.45 | 0 | .001 b |
| Total enlargement (mm) | 0.21 ± 0.08 | 0.04 ± 0.04 | 0.01 ± 0.03 | .001 b |
| Total change (%) | 11.41 | 1.59 | 0.42 | .001 b |
b A statistically significant difference was present between the 3 groups, but not between Group II and Group III.
Architectural Profile of Clear Corneal Incision
Table 4 shows the change in maximal clear corneal incision thickness as evaluated by AS-OCT at 1 day, 1 week, 1 month, and 3 months after surgery. The architectural profile of the clear corneal incision was stable after 1 month postoperatively.



